Shina Menon, Michelle C Starr, Huaiyu Zang, Michaela Collins, Mihaela A Damian, Dana Fuhrman, Kelli Krallman, Danielle E Soranno, Tennille N Webb, Cara Slagle, Catherine Joseph, Susan D Martin, Tahagod Mohamed, Morgan E Beebe, Zaccaria Ricci, Nicholas Ollberding, David Selewski, Katja M Gist
{"title":"Characteristics and outcomes of children ≤ 10 kg receiving continuous kidney replacement therapy: a WE-ROCK study.","authors":"Shina Menon, Michelle C Starr, Huaiyu Zang, Michaela Collins, Mihaela A Damian, Dana Fuhrman, Kelli Krallman, Danielle E Soranno, Tennille N Webb, Cara Slagle, Catherine Joseph, Susan D Martin, Tahagod Mohamed, Morgan E Beebe, Zaccaria Ricci, Nicholas Ollberding, David Selewski, Katja M Gist","doi":"10.1007/s00467-024-06438-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Continuous kidney replacement therapy (CKRT) is often used for acute kidney injury (AKI) or fluid overload (FO) in children ≤ 10 kg. Intensive care unit (ICU) mortality in children ≤ 10 kg reported by the prospective pediatric CRRT (ppCRRT, 2001-2003) registry was 57%. We aimed to evaluate characteristics associated with ICU mortality using a contemporary registry.</p><p><strong>Methods: </strong>The Worldwide Exploration of Renal Replacement Outcomes Collaborative in Kidney Disease (WE-ROCK) registry is a retrospective, multinational, observational study of children and young adults aged 0-25 years receiving CKRT (2015-2021) for AKI or FO. This analysis included patients ≤ 10 kg at hospital admission.</p><p><strong>Primary and secondary outcomes: </strong>ICU mortality and major adverse kidney events at 90 days (MAKE-90) defined as death, persistent kidney dysfunction, or dialysis within 90 days, respectively.</p><p><strong>Results: </strong>A total of 210 patients were included (median age 0.53 years (IQR, 0.1, 0.9)). ICU mortality was 46.5%. MAKE-90 occurred in 150/207 (72%). CKRT was initiated at a median 3 days (IQR 1, 9) after ICU admission and lasted a median 6 days (IQR 3, 16). On multivariable analysis, pediatric logistic organ dysfunction score (PELOD-2) at CKRT initiation was associated with increased odds of ICU mortality (aOR 2.64, 95% CI 1.68-4.16), and increased odds of MAKE-90 (aOR 2.2, 95% CI 1.31-3.69). Absence of comorbidity was associated with lower MAKE-90 (aOR 0.29, 95%CI 0.13-0.65).</p><p><strong>Conclusions: </strong>We report on a contemporary cohort of children ≤ 10 kg treated with CKRT for acute kidney injury and/or fluid overload. ICU mortality is decreased compared to ppCRRT. The extended risk of death and morbidity at 90 days highlights the importance of close follow-up.</p>","PeriodicalId":19735,"journal":{"name":"Pediatric Nephrology","volume":" ","pages":"253-264"},"PeriodicalIF":2.6000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11969683/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Nephrology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00467-024-06438-x","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/20 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Continuous kidney replacement therapy (CKRT) is often used for acute kidney injury (AKI) or fluid overload (FO) in children ≤ 10 kg. Intensive care unit (ICU) mortality in children ≤ 10 kg reported by the prospective pediatric CRRT (ppCRRT, 2001-2003) registry was 57%. We aimed to evaluate characteristics associated with ICU mortality using a contemporary registry.
Methods: The Worldwide Exploration of Renal Replacement Outcomes Collaborative in Kidney Disease (WE-ROCK) registry is a retrospective, multinational, observational study of children and young adults aged 0-25 years receiving CKRT (2015-2021) for AKI or FO. This analysis included patients ≤ 10 kg at hospital admission.
Primary and secondary outcomes: ICU mortality and major adverse kidney events at 90 days (MAKE-90) defined as death, persistent kidney dysfunction, or dialysis within 90 days, respectively.
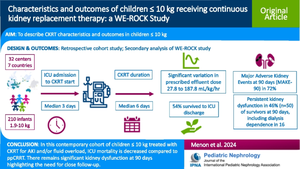
Results: A total of 210 patients were included (median age 0.53 years (IQR, 0.1, 0.9)). ICU mortality was 46.5%. MAKE-90 occurred in 150/207 (72%). CKRT was initiated at a median 3 days (IQR 1, 9) after ICU admission and lasted a median 6 days (IQR 3, 16). On multivariable analysis, pediatric logistic organ dysfunction score (PELOD-2) at CKRT initiation was associated with increased odds of ICU mortality (aOR 2.64, 95% CI 1.68-4.16), and increased odds of MAKE-90 (aOR 2.2, 95% CI 1.31-3.69). Absence of comorbidity was associated with lower MAKE-90 (aOR 0.29, 95%CI 0.13-0.65).
Conclusions: We report on a contemporary cohort of children ≤ 10 kg treated with CKRT for acute kidney injury and/or fluid overload. ICU mortality is decreased compared to ppCRRT. The extended risk of death and morbidity at 90 days highlights the importance of close follow-up.
期刊介绍:
International Pediatric Nephrology Association
Pediatric Nephrology publishes original clinical research related to acute and chronic diseases that affect renal function, blood pressure, and fluid and electrolyte disorders in children. Studies may involve medical, surgical, nutritional, physiologic, biochemical, genetic, pathologic or immunologic aspects of disease, imaging techniques or consequences of acute or chronic kidney disease. There are 12 issues per year that contain Editorial Commentaries, Reviews, Educational Reviews, Original Articles, Brief Reports, Rapid Communications, Clinical Quizzes, and Letters to the Editors.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
