{"title":"Medical management of post-sublobar resection pulmonary granulomatous lesion: a report of two cases.","authors":"Hideki Endoh, Nariaki Oura, Satoru Yanagisawa, Nobutoshi Morozumi, Nobuhiro Nishizawa, Ryohei Yamamoto, Yukitoshi Satoh","doi":"10.1186/s40792-024-01969-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Automatic stapling devices are commonly utilized in pulmonary resections, including sublobar segmentectomy. Large tumors can develop around the staple line, posing challenges in distinguishing them from cancer recurrence or inflammatory changes. In this report, we present two cases of symptomatic staple granulomatous lesion effectively managed with medications.</p><p><strong>Case presentation: </strong>A 74-year-old man presented with a persistent cough and sputum production six years post-segmentectomy for a hamartoma in the left upper lobe. Chest computed tomography (CT) revealed a large tumor around the staple line. Laboratory investigations and bronchoscopic examination revealed no malignancy. The patient received corticosteroids and a cyclooxygenase-2 inhibitor; despite experiencing adverse reactions to steroids, both tumor size and respiratory symptoms were significantly reduced. The second case involved a 78-year-old woman who underwent pulmonary resection for suspected lung cancer. Despite a non-malignant tumor diagnosis, she reported a cough six months post-surgery. Chest CT revealed extensive shadow around the surgical staple, which was diagnosed as mycobacterium granuloma. Low-dose erythromycin induced inflammatory changes but effectively reduced the lesion.</p><p><strong>Conclusions: </strong>Granulomatous lesions around the staple can be effectively managed with medication, and monitoring the treatment response proves valuable in distinguishing them from tumor recurrence post-pulmonary resection.</p>","PeriodicalId":22096,"journal":{"name":"Surgical Case Reports","volume":"10 1","pages":"193"},"PeriodicalIF":0.7000,"publicationDate":"2024-08-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11335699/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40792-024-01969-9","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Automatic stapling devices are commonly utilized in pulmonary resections, including sublobar segmentectomy. Large tumors can develop around the staple line, posing challenges in distinguishing them from cancer recurrence or inflammatory changes. In this report, we present two cases of symptomatic staple granulomatous lesion effectively managed with medications.
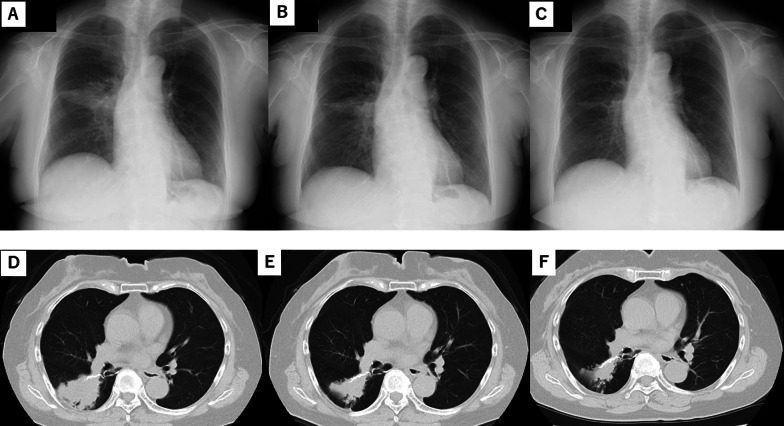
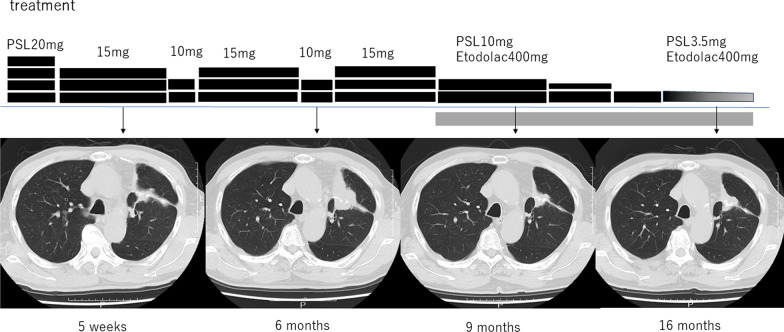
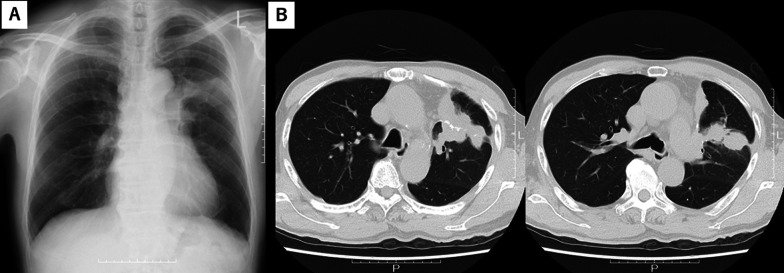
Case presentation: A 74-year-old man presented with a persistent cough and sputum production six years post-segmentectomy for a hamartoma in the left upper lobe. Chest computed tomography (CT) revealed a large tumor around the staple line. Laboratory investigations and bronchoscopic examination revealed no malignancy. The patient received corticosteroids and a cyclooxygenase-2 inhibitor; despite experiencing adverse reactions to steroids, both tumor size and respiratory symptoms were significantly reduced. The second case involved a 78-year-old woman who underwent pulmonary resection for suspected lung cancer. Despite a non-malignant tumor diagnosis, she reported a cough six months post-surgery. Chest CT revealed extensive shadow around the surgical staple, which was diagnosed as mycobacterium granuloma. Low-dose erythromycin induced inflammatory changes but effectively reduced the lesion.
Conclusions: Granulomatous lesions around the staple can be effectively managed with medication, and monitoring the treatment response proves valuable in distinguishing them from tumor recurrence post-pulmonary resection.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
