Yong-Hao Yeo , Jia-Yean Thong , Min-Choon Tan , Qi-Xuan Ang , Boon-Jian San , Bryan E-Xin Tan , Arka Chatterjee , Kwan Lee
{"title":"Risk factors for early mortality following transcatheter edge-to-edge repair of mitral regurgitation","authors":"Yong-Hao Yeo , Jia-Yean Thong , Min-Choon Tan , Qi-Xuan Ang , Boon-Jian San , Bryan E-Xin Tan , Arka Chatterjee , Kwan Lee","doi":"10.1016/j.carrev.2024.08.001","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><div>While transcatheter edge-to-edge repair (TEER) with MitraClip is increasingly used, data on the risk stratification for assessing early mortality after this procedure are scarce.</div></div><div><h3>Objective</h3><div>This study aimed to assess early mortality and analyze the risk factors of early mortality among patients who underwent TEER.</div></div><div><h3>Methods</h3><div>Using the all-payer, nationally representative Nationwide Readmissions Database, our study included patients aged 18 years or older who had TEER between January 2017 and November 2020. We categorized the cohort into two groups depending on the occurrence of early mortality (death within 30 days after the procedure). Based on the ICD-10, we identified the trend of early mortality after TEER and further analyzed the risk factors associated with early mortality.</div></div><div><h3>Results</h3><div>A total of 15,931 patients who had TEER were included; 292 (1.8 %) with early mortality and 15,639 (98.2 %) without. There was a decreasing trend in early mortality from 2.8 % in the first quarter of 2017 to 1.2 % in the fourth quarter of 2020, but it was not statistically significant (<em>p</em> = 0.18). In multivariable analysis, the independent risk factors for early mortality were chronic kidney disease not requiring dialysis (adjusted odds ratio [aOR]: 1.57; 95 % confidence interval [CI]: 1.11–2.22, <em>p</em> = 0.01), end-stage renal disease (aOR: 2.34; CI: 1.44–3.79, <em>p</em> < 0.01), chronic liver disease (aOR: 4.90; CI: 3.29–7.29, p < 0.01), coagulation disorder (aOR: 3.42; CI: 2.35–5.03, p < 0.01), systolic heart failure (aOR: 2.81; CI: 1.34–5.90, <em>p</em> < 0.01), diastolic heart failure (aOR: 2.69; CI: 1.24–5.84, <em>p</em> = 0.01) and unspecified heart failure (aOR: 3.23; CI: 1.49–7.01, p < 0.01). Among those who died during 30-day readmission following TEER, the most common cardiac cause and non-cardiac-cause of readmission were heart failure (18.2 %) and infection (26.6 %), respectively.</div></div><div><h3>Conclusion</h3><div>The early mortality following TEER was low at 1.8 %. The independent risk factors associated with early mortality were chronic kidney disease (including end-stage renal disease), chronic liver disease, coagulation disorder, and heart failure (both systolic and diastolic).</div></div>","PeriodicalId":47657,"journal":{"name":"Cardiovascular Revascularization Medicine","volume":"74 ","pages":"Pages 1-7"},"PeriodicalIF":1.9000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiovascular Revascularization Medicine","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S1553838924006262","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/15 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background
While transcatheter edge-to-edge repair (TEER) with MitraClip is increasingly used, data on the risk stratification for assessing early mortality after this procedure are scarce.
Objective
This study aimed to assess early mortality and analyze the risk factors of early mortality among patients who underwent TEER.
Methods
Using the all-payer, nationally representative Nationwide Readmissions Database, our study included patients aged 18 years or older who had TEER between January 2017 and November 2020. We categorized the cohort into two groups depending on the occurrence of early mortality (death within 30 days after the procedure). Based on the ICD-10, we identified the trend of early mortality after TEER and further analyzed the risk factors associated with early mortality.
Results
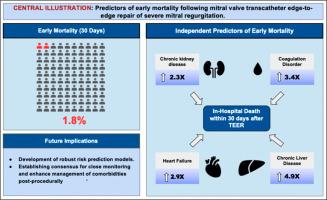
A total of 15,931 patients who had TEER were included; 292 (1.8 %) with early mortality and 15,639 (98.2 %) without. There was a decreasing trend in early mortality from 2.8 % in the first quarter of 2017 to 1.2 % in the fourth quarter of 2020, but it was not statistically significant (p = 0.18). In multivariable analysis, the independent risk factors for early mortality were chronic kidney disease not requiring dialysis (adjusted odds ratio [aOR]: 1.57; 95 % confidence interval [CI]: 1.11–2.22, p = 0.01), end-stage renal disease (aOR: 2.34; CI: 1.44–3.79, p < 0.01), chronic liver disease (aOR: 4.90; CI: 3.29–7.29, p < 0.01), coagulation disorder (aOR: 3.42; CI: 2.35–5.03, p < 0.01), systolic heart failure (aOR: 2.81; CI: 1.34–5.90, p < 0.01), diastolic heart failure (aOR: 2.69; CI: 1.24–5.84, p = 0.01) and unspecified heart failure (aOR: 3.23; CI: 1.49–7.01, p < 0.01). Among those who died during 30-day readmission following TEER, the most common cardiac cause and non-cardiac-cause of readmission were heart failure (18.2 %) and infection (26.6 %), respectively.
Conclusion
The early mortality following TEER was low at 1.8 %. The independent risk factors associated with early mortality were chronic kidney disease (including end-stage renal disease), chronic liver disease, coagulation disorder, and heart failure (both systolic and diastolic).
期刊介绍:
Cardiovascular Revascularization Medicine (CRM) is an international and multidisciplinary journal that publishes original laboratory and clinical investigations related to revascularization therapies in cardiovascular medicine. Cardiovascular Revascularization Medicine publishes articles related to preclinical work and molecular interventions, including angiogenesis, cell therapy, pharmacological interventions, restenosis management, and prevention, including experiments conducted in human subjects, in laboratory animals, and in vitro. Specific areas of interest include percutaneous angioplasty in coronary and peripheral arteries, intervention in structural heart disease, cardiovascular surgery, etc.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
