Patrick Heindel, James J Fitzgibbon, Eric Secemsky, Deepak L Bhatt, Mohammed Al-Omran, Subodh Verma, Ibrahim A Almaghlouth, Arin Madenci, Mohamad A Hussain
{"title":"Colchicine for cardiovascular and limb risk reduction in Medicare beneficiaries with peripheral artery disease: emulation of target trials.","authors":"Patrick Heindel, James J Fitzgibbon, Eric Secemsky, Deepak L Bhatt, Mohammed Al-Omran, Subodh Verma, Ibrahim A Almaghlouth, Arin Madenci, Mohamad A Hussain","doi":"10.1093/ehjopen/oeae062","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Recent evidence from randomized trials demonstrates that colchicine can reduce the risk of major adverse cardiovascular events (MACE) in patients with coronary artery disease. Colchicine's effect on lower-extremity peripheral artery disease (PAD) is not known.</p><p><strong>Methods and results: </strong>To make inferences about the real-world effectiveness of colchicine in PAD, we emulated two target trials leveraging the variable prescribing practice of adding colchicine vs. a non-steroidal anti-inflammatory drug (NSAID) to urate-lowering therapy in patients with gout and PAD. Emulated Trial 1 compared colchicine initiators with NSAID initiators. Emulated Trial 2 compared long-term (indefinite) and short-term (3 months) treatment strategies after initiating colchicine. Eligible individuals were those continuously enrolled in Medicare receiving care at a multicentre academic health system between July 2007 and December 2019. The primary outcome for both trials was a 2 year composite of major adverse limb events (MALE), MACE, and all-cause mortality. Secondary outcomes included MALE and death, MACE and death, and individual components of the primary outcome. Inverse probability weighting was used to adjust for confounding. Percentile-based 95% confidence intervals (CIs) were estimated using non-parametric bootstrapping. A total of 1820 eligible patients were included; the mean age was 77 years [standard deviation (SD) 7], 32% were female, and 9% were non-White. The mean (SD) duration of colchicine and NSAID therapy was 247 (345) and 137 (237) days, respectively. In the emulation of Trial 1, the risk of the primary composite outcome of MALE, MACE, and death at 2 years was 29.9% (95% CI 27.2%, 32.3%) in the colchicine group and 31.5% (28.3%, 34.6%) in the NSAID group, with a risk difference of -1.7% (95% CI -6.5%, 3.1%) and a risk ratio of 0.95 (95% CI 0.83, 1.07). Similar findings were noted in the emulation of Trial 2, with a risk of the primary composite outcome at 2 years of 30.7% (95% CI 23.7%, 38.1%) in the long-term colchicine group and 33.4% (95% CI 29.4%, 37.7%) in the short-term group, with a risk difference of -2.7% (95% CI -10.3%, 5.4%) and risk ratio of 0.92 (95% CI 0.70, 1.16).</p><p><strong>Conclusion: </strong>In a real-world sample of patients with PAD and gout, estimates of the effect of colchicine were consistent across two analyses and provided no conclusive evidence that colchicine decreased the risk of adverse cardiovascular or limb events and death. The cardiovascular and limb benefits of colchicine in older, comorbid populations with PAD and advanced systematic atherosclerosis remain uncertain.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"4 4","pages":"oeae062"},"PeriodicalIF":0.0000,"publicationDate":"2024-08-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11339712/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeae062","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: Recent evidence from randomized trials demonstrates that colchicine can reduce the risk of major adverse cardiovascular events (MACE) in patients with coronary artery disease. Colchicine's effect on lower-extremity peripheral artery disease (PAD) is not known.
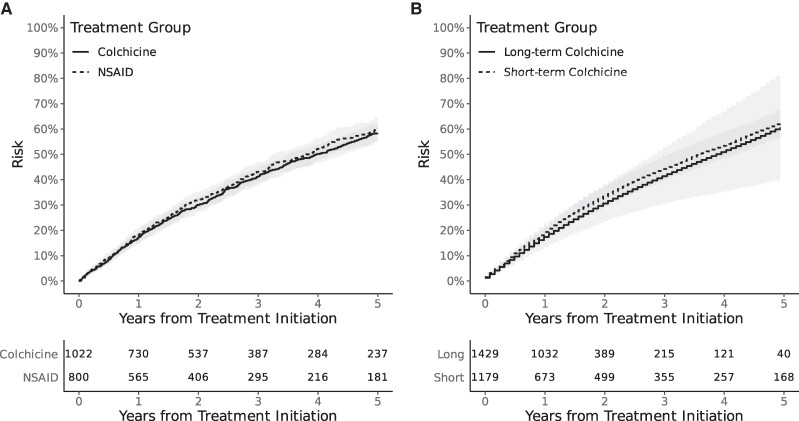
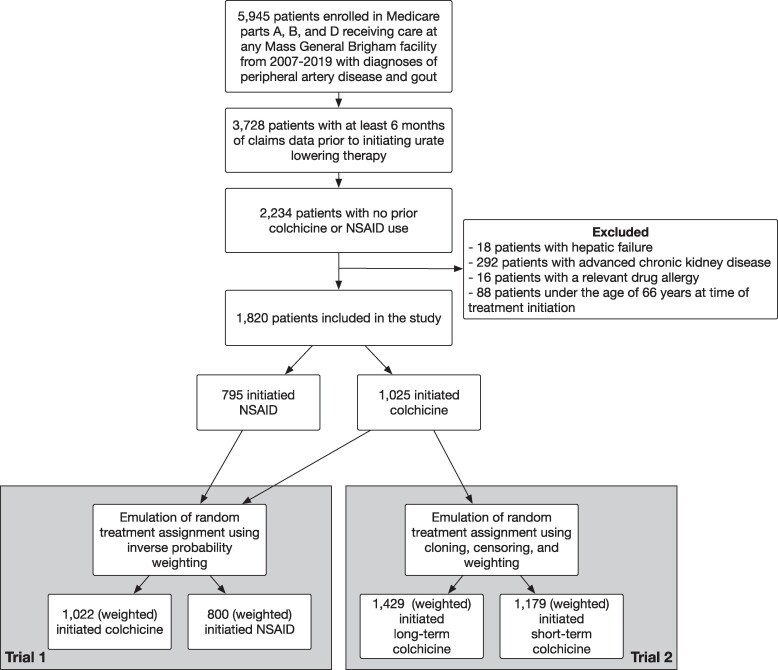
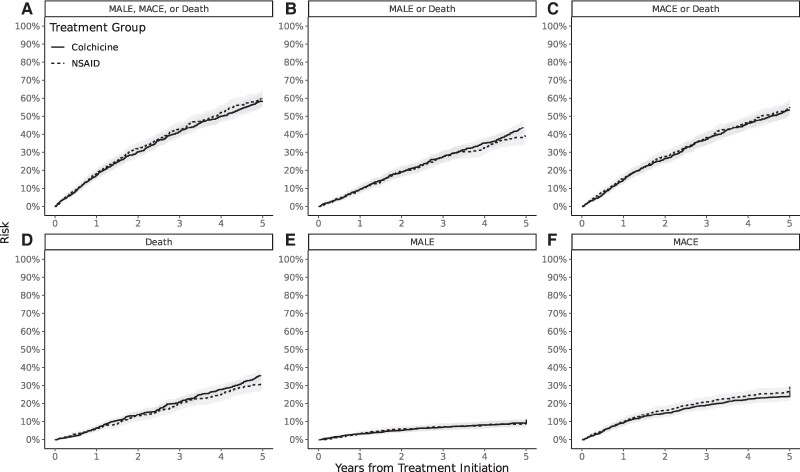
Methods and results: To make inferences about the real-world effectiveness of colchicine in PAD, we emulated two target trials leveraging the variable prescribing practice of adding colchicine vs. a non-steroidal anti-inflammatory drug (NSAID) to urate-lowering therapy in patients with gout and PAD. Emulated Trial 1 compared colchicine initiators with NSAID initiators. Emulated Trial 2 compared long-term (indefinite) and short-term (3 months) treatment strategies after initiating colchicine. Eligible individuals were those continuously enrolled in Medicare receiving care at a multicentre academic health system between July 2007 and December 2019. The primary outcome for both trials was a 2 year composite of major adverse limb events (MALE), MACE, and all-cause mortality. Secondary outcomes included MALE and death, MACE and death, and individual components of the primary outcome. Inverse probability weighting was used to adjust for confounding. Percentile-based 95% confidence intervals (CIs) were estimated using non-parametric bootstrapping. A total of 1820 eligible patients were included; the mean age was 77 years [standard deviation (SD) 7], 32% were female, and 9% were non-White. The mean (SD) duration of colchicine and NSAID therapy was 247 (345) and 137 (237) days, respectively. In the emulation of Trial 1, the risk of the primary composite outcome of MALE, MACE, and death at 2 years was 29.9% (95% CI 27.2%, 32.3%) in the colchicine group and 31.5% (28.3%, 34.6%) in the NSAID group, with a risk difference of -1.7% (95% CI -6.5%, 3.1%) and a risk ratio of 0.95 (95% CI 0.83, 1.07). Similar findings were noted in the emulation of Trial 2, with a risk of the primary composite outcome at 2 years of 30.7% (95% CI 23.7%, 38.1%) in the long-term colchicine group and 33.4% (95% CI 29.4%, 37.7%) in the short-term group, with a risk difference of -2.7% (95% CI -10.3%, 5.4%) and risk ratio of 0.92 (95% CI 0.70, 1.16).
Conclusion: In a real-world sample of patients with PAD and gout, estimates of the effect of colchicine were consistent across two analyses and provided no conclusive evidence that colchicine decreased the risk of adverse cardiovascular or limb events and death. The cardiovascular and limb benefits of colchicine in older, comorbid populations with PAD and advanced systematic atherosclerosis remain uncertain.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
