Effects of intranasal dexmedetomidine versus intranasal midazolam as premedication in children with tetralogy of Fallot undergoing corrective cardiac surgery: A randomized trial.
{"title":"Effects of intranasal dexmedetomidine versus intranasal midazolam as premedication in children with tetralogy of Fallot undergoing corrective cardiac surgery: A randomized trial.","authors":"Sarvesh Srivastava, Sambhunath Das, Neeti Makhija, Sandeep Chauhan","doi":"10.4103/apc.apc_10_24","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This prospective, randomized, double-blind trial was done to compare intranasal dexmedetomidine and intranasal midazolam as premedication for sedation and ease of child-parent separation in pediatric patients of tetralogy of Fallot (TOF) undergoing corrective cardiac surgery.</p><p><strong>Materials and methods: </strong>Forty children with TOF, between 1 and 10 years, undergoing corrective cardiac surgery were included in the study and, after randomization, were given intranasal midazolam (0.2 mg/kg) or intranasal dexmedetomidine (1 µg/kg), 30 min before shifting to the operation room (OR). Patients were assessed for sedation and child-parent separation, along with hemodynamic parameters, respiratory rate, and oxygen saturation (SpO2) 30 min after drug administration, at the time of shifting inside the OR, and at the time of induction of anesthesia.</p><p><strong>Results: </strong>Both groups had comparable child-parent scores, hemodynamic parameters, SpO2, and respiratory rate. However, the dexmedetomidine group had significantly better sedation levels than the midazolam group patients at the time of shifting inside the OR (dexmedetomidine group: 3.55 ± 0.82 vs. midazolam group: 2.80 ± 0.83; <i>P</i> = 0.007) and at the time of induction of anesthesia (dexmedetomidine group: 3.40 ± 0.75 vs. midazolam group: 2.70 ± 0.86; P = 0.009).</p><p><strong>Conclusion: </strong>Intranasal dexmedetomidine provides better sedation than midazolam, with similar child-parent separation scores and hemodynamic parameters, respiratory rate, and SpO2. No adverse events were observed in both groups. A study on a larger population will help in further establishing the safety and superiority of dexmedetomidine and will further its regular use as an intranasal premedication.</p>","PeriodicalId":8026,"journal":{"name":"Annals of Pediatric Cardiology","volume":"17 2","pages":"109-115"},"PeriodicalIF":0.7000,"publicationDate":"2024-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11343385/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Pediatric Cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/apc.apc_10_24","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/20 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: This prospective, randomized, double-blind trial was done to compare intranasal dexmedetomidine and intranasal midazolam as premedication for sedation and ease of child-parent separation in pediatric patients of tetralogy of Fallot (TOF) undergoing corrective cardiac surgery.
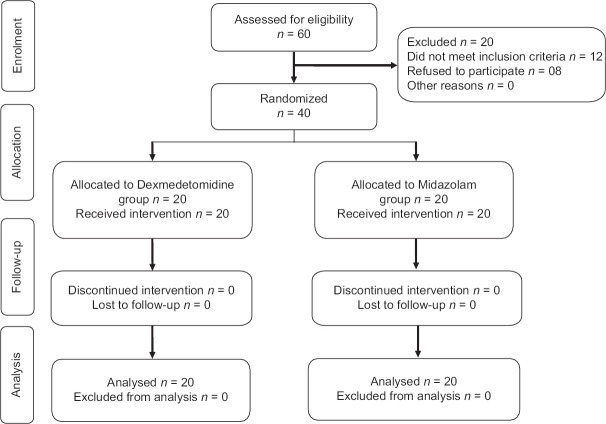
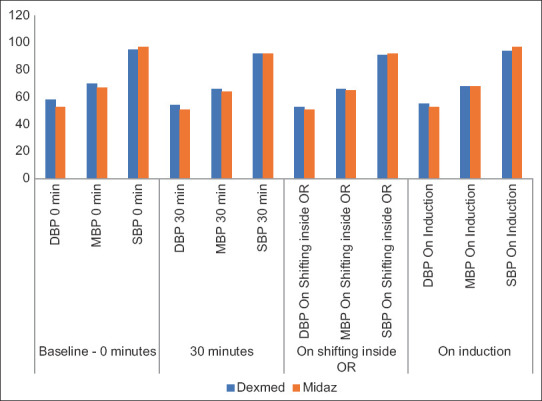
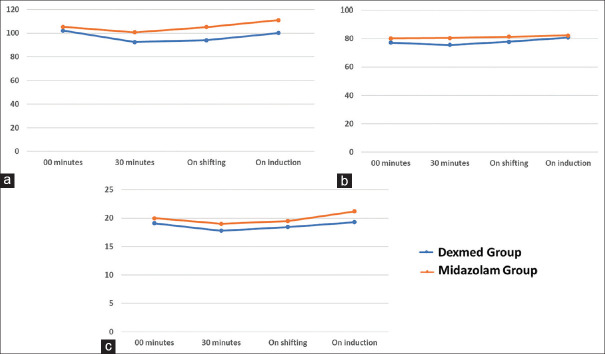
Materials and methods: Forty children with TOF, between 1 and 10 years, undergoing corrective cardiac surgery were included in the study and, after randomization, were given intranasal midazolam (0.2 mg/kg) or intranasal dexmedetomidine (1 µg/kg), 30 min before shifting to the operation room (OR). Patients were assessed for sedation and child-parent separation, along with hemodynamic parameters, respiratory rate, and oxygen saturation (SpO2) 30 min after drug administration, at the time of shifting inside the OR, and at the time of induction of anesthesia.
Results: Both groups had comparable child-parent scores, hemodynamic parameters, SpO2, and respiratory rate. However, the dexmedetomidine group had significantly better sedation levels than the midazolam group patients at the time of shifting inside the OR (dexmedetomidine group: 3.55 ± 0.82 vs. midazolam group: 2.80 ± 0.83; P = 0.007) and at the time of induction of anesthesia (dexmedetomidine group: 3.40 ± 0.75 vs. midazolam group: 2.70 ± 0.86; P = 0.009).
Conclusion: Intranasal dexmedetomidine provides better sedation than midazolam, with similar child-parent separation scores and hemodynamic parameters, respiratory rate, and SpO2. No adverse events were observed in both groups. A study on a larger population will help in further establishing the safety and superiority of dexmedetomidine and will further its regular use as an intranasal premedication.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
