Nelleke Pietronella Maria Brouwer, Ayse Selcen Oguz Erdogan, Shannon van Vliet, Natasja Rutgers, Nikki Knijn, Gesina van Lijnschoten, Jessica Juliana Tan, Johannes Hendrik Willem de Wilt, Niek Hugen, Gina Brown, Femke Simmer, Iris Dionne Nagtegaal
{"title":"Unraveling the routes to distant metastases in colorectal cancer: Tumor deposits and lymph node metastases as the gateway","authors":"Nelleke Pietronella Maria Brouwer, Ayse Selcen Oguz Erdogan, Shannon van Vliet, Natasja Rutgers, Nikki Knijn, Gesina van Lijnschoten, Jessica Juliana Tan, Johannes Hendrik Willem de Wilt, Niek Hugen, Gina Brown, Femke Simmer, Iris Dionne Nagtegaal","doi":"10.1002/cac2.12598","DOIUrl":null,"url":null,"abstract":"<p>Currently, lymph node metastases (LNM) are seen as the gateway to distant metastases in CRC and play a crucial role in the Tumor Node Metastasis (TNM) staging system [<span>1, 2</span>]. Tumor deposits (TD) have been identified as another histological feature with a strong prognostic impact but are currently only deemed clinically relevant in the absence of LNM [<span>2, 3</span>]. TD are clusters of tumor cells in the fat surrounding the bowel and are often associated with nerves, vessels and lymphatic tissue, giving the cancer cells access to multiple routes of spread [<span>4</span>].</p><p>To study whether TD could indeed form an alternative gateway to distant metastases, we have used polyG-based phylogenetics on formalin-fixed paraffin-embedded (FFPE) tissue to investigate the role of histologically defined TD and LNM in CRC evolution and distant metastatic spread to the liver and peritoneum.</p><p>We collected data from patients who were diagnosed with colorectal liver or peritoneal metastases between January 2015 and January 2022 and not previously treated with chemotherapy. DNA was isolated from the TD and LNM (Figure 1A), normal tissue (which was sampled at the edge of the resection specimen) and distant metastases. Three distinct tissue parts of the primary tumor were sampled to account for intra-tumor heterogeneity (Figure 1B), yielding a total of 480 samples (Supplementary Table S1). Polymerase chain reaction (PCR) was used to genotype up to 24 polyG regions for every sample (Supplementary Table S2). Sequentially, phylogenetic trees were constructed based on the peak distribution of all PCR results from the polyG regions using an analysis pipeline previously developed by Naxerova et al. in R software (version 4.3.1) [<span>5</span>]. Phylogenetic trees are graphical representations of the evolutionary relationship between biological entities, in this case, the different tissue samples. After quality control of PCR results (i.e., poor quality DNA), impurity (i.e., contamination of samples with non-tumorous cells, Supplementary Figure S1), and branching confidence (i.e., values < 50% were deemed unreliable), 47 CRC patients with a total of 43 individual liver metastases and 30 individual peritoneal metastases were included in the final results (Supplementary Table S3-S5). The distribution of origins (TD, LNM, primary tumor or a mix of these) was compared between the group of liver and the group of peritoneal metastases using Fisher's exact test. Potential confounding clinicopathological factors were analyzed using the Kruskal-Wallis of Fisher's exact test. <i>P</i> values < 0.05 were considered significant. Full descriptions of the materials and methods are provided in the Supplementary Materials.</p><p>Phylogenetic analysis showed that the primary tumor, TD, and LNM could be possible origins of liver metastases. An exemplary phylogenetic tree is shown in Figure 1C, where different subclones gave rise to different LNMs, and several liver metastases with common ancestry were related to the TD. Taken together, TD, LNM, primary tumor or a mix of these were found to be the origin of liver metastases in 23%, 23%, 23% and 30%, respectively (Figure 1D). Several clinicopathological variables were tested for biasing the results, of which only the number of included TDs was significantly different between the liver metastases related to TD and PT (<i>P</i> = 0.03), all other comparisons showed no differences significantly with the number of metastases related to TD (Supplementary Figures S2-S3). Our data show that LNM can form a gateway to liver metastases in 23% of cases, which is in line with an earlier smaller study, where 0-35% of liver metastases were found to be related to LNM [<span>5</span>]. These results are in contrast with the idea that LNM is the main gateway to distant metastases, which is the basis for the current TNM staging system. Importantly, TD were identified as an alternative gateway in 23% of liver metastases, which confirms the prognostic evidence that shows an increased risk of liver metastases in patients with TD [<span>3</span>].</p><p>In contrast to liver metastases, peritoneal metastases were most often related to TD with 40% of cases and second most often to the primary tumor with 37%. LNMs or a mix of the different structures formed the origin in 7% and 10% of peritoneal metastases, respectively (Figure 1E). These results provide phylogenetic evidence that supports previous studies showing that the presence of TDs is associated with an increased risk of peritoneal metastases [<span>6</span>].</p><p>This study demonstrated a clear difference in the evolution of liver and peritoneal metastases, with a significantly different distribution of origins (<i>P</i> < 0.05, Figure 1D-E) and 40% of peritoneal metastases versus 23% of liver metastases being related to TD. This could be explained by biologically different pathways to metastases. Liver metastases are thought to develop through the invasion-metastasis cascade where tumor cells spread to distant organs via the circulatory system [<span>7</span>]. Both LNMs and TDs formed possible gateways to liver metastases in the phylogenetic analyses and have their own way of accessing the systemic circulation. For LNMs, mouse studies showed that tumor cells could either invade small blood vessels surrounding the lymph node or travel through the lymphatic system and enter the systemic circulation at the thoracic duct [<span>8</span>]. Still, the exact mechanism is being widely debated, and in humans, the mechanism remains unclear. For TDs, it is more widely accepted that they have access to the blood circulation as it is reflected in their histology [<span>4</span>]. In line with literature, our study demonstrated a vascular component in 69% of TD related to liver metastases (Supplementary Figure S4). An alternative to the invasion-metastasis cascade has been proposed for peritoneal metastases involving more direct migration of tumor cells to the peritoneum [<span>7</span>]. We previously showed that the molecular phenotype needed for tumor cells to actively migrate to and invade the peritoneum is overexpressed in TD compared with LNM [<span>9</span>]. Therefore, it is likely that tumor cells with the ability to form TD are also capable of further migration through the serosal surface and invasion of the peritoneum, more so than the tumor cells in LNM.</p><p>There are some limitations to this study. Firstly, although all cases complied with the guideline quality of more than 12 sampled lymph nodes per CRC, and TD were scored by two pathologists and an expert researcher, there is a small chance that some TD or LNM were missed during the sampling of resection specimens. Secondly, it would be recommended that all phylogenetic studies be validated using a different method, such as whole genome or exome sequencing, to show whether the results are generalizable and robust [<span>10</span>]. Thirdly, due to time and financial restraints, this study only included the most common metastatic sites in CRC, liver and peritoneum. Including other metastatic sites would provide a more comprehensive overview of the process of metastatic spread in CRC.</p><p>In conclusion, with the use of phylogenic analysis, this study shows that both TDs and LNMs can be related to liver or peritoneal metastases in CRC. Moreover, the origin of metastases differs per metastatic site, with liver metastases being equally related to TDs and LNMs and peritoneal metastases being significantly more often related to TDs. Therefore, future research should focus on whether patients with TDs are at increased risk of peritoneal metastases, as this could impact follow-up and treatment decisions. Also, since we showed that a significant number of liver and peritoneal metastases were related to TDs, it should be questioned whether the current method of including TDs as less important than LNMs in the staging for CRC patients is justified. We propose that TDs should merit more attention by including them as equally important to LNMs in the nodal category and continuing to register them for future research.</p><p><i>Conceptualization</i>: Gina Brown, Femke Simmer, Iris Dionne Nagtegaal. <i>Methodology</i>: Nelleke Pietronella Maria Brouwer, Ayse Selcen Oguz Erdogan, Niek Hugen, Femke Simmer, Iris Dionne Nagtegaal. <i>Funding acquisition</i>: Gina Brown, Iris Dionne Nagtegaal. <i>Acquisition and analysis of data</i>: Nelleke Pietronella Maria Brouwer, Ayse Selcen Oguz Erdogan, Shannon van Vliet, Natasja Rutgers. <i>Statistical analysis</i>: Nelleke Pietronella Maria Brouwer, Ayse Selcen Oguz Erdogan, Shannon van Vliet, Natasja Rutgers, Femke Simmer. <i>Material support</i>: Nikki Knijn, Gesina van Lijnschoten, Jessica Juliana Tan, Gina Brown. <i>Writing—original draft</i>: Nelleke Pietronella Maria Brouwer, Ayse Selcen Oguz Erdogan, Niek Hugen, Femke Simmer, Iris Dionne Nagtegaal. <i>Writing—review & editing</i>: Nelleke Pietronella Maria Brouwer, Ayse Selcen Oguz Erdogan, Shannon van Vliet, Natasja Rutgers, Nikki Knijn, Gesina van Lijnschoten, Jessica Juliana Tan, Johannes Hendrik Willem de Wilt, Niek Hugen, Gina Brown, Femke Simmer, Iris Dionne Nagtegaal.</p><p>All authors declare no conflicts of interest.</p><p>This study was supported by the Dutch Cancer Society (KUN 2019-12640).</p><p>The study was performed according to the Dutch “Federa, Human Tissue and Medical Research: Code of Conduct for Responsible Use (2011)” regulations, not requiring patient informed consent. This study was approved by the Ethics Committee (CMO) of the Radboudumc (approval number 2020-7172).</p>","PeriodicalId":9495,"journal":{"name":"Cancer Communications","volume":"44 10","pages":"1209-1213"},"PeriodicalIF":24.9000,"publicationDate":"2024-08-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cac2.12598","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer Communications","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cac2.12598","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Currently, lymph node metastases (LNM) are seen as the gateway to distant metastases in CRC and play a crucial role in the Tumor Node Metastasis (TNM) staging system [1, 2]. Tumor deposits (TD) have been identified as another histological feature with a strong prognostic impact but are currently only deemed clinically relevant in the absence of LNM [2, 3]. TD are clusters of tumor cells in the fat surrounding the bowel and are often associated with nerves, vessels and lymphatic tissue, giving the cancer cells access to multiple routes of spread [4].
To study whether TD could indeed form an alternative gateway to distant metastases, we have used polyG-based phylogenetics on formalin-fixed paraffin-embedded (FFPE) tissue to investigate the role of histologically defined TD and LNM in CRC evolution and distant metastatic spread to the liver and peritoneum.
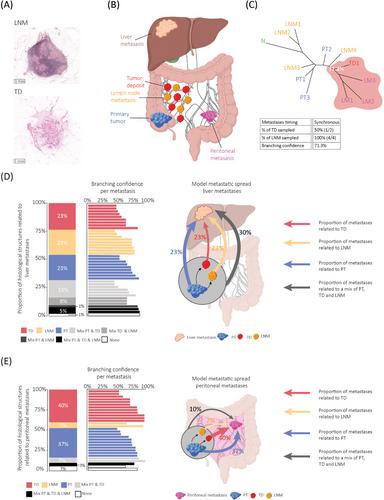
We collected data from patients who were diagnosed with colorectal liver or peritoneal metastases between January 2015 and January 2022 and not previously treated with chemotherapy. DNA was isolated from the TD and LNM (Figure 1A), normal tissue (which was sampled at the edge of the resection specimen) and distant metastases. Three distinct tissue parts of the primary tumor were sampled to account for intra-tumor heterogeneity (Figure 1B), yielding a total of 480 samples (Supplementary Table S1). Polymerase chain reaction (PCR) was used to genotype up to 24 polyG regions for every sample (Supplementary Table S2). Sequentially, phylogenetic trees were constructed based on the peak distribution of all PCR results from the polyG regions using an analysis pipeline previously developed by Naxerova et al. in R software (version 4.3.1) [5]. Phylogenetic trees are graphical representations of the evolutionary relationship between biological entities, in this case, the different tissue samples. After quality control of PCR results (i.e., poor quality DNA), impurity (i.e., contamination of samples with non-tumorous cells, Supplementary Figure S1), and branching confidence (i.e., values < 50% were deemed unreliable), 47 CRC patients with a total of 43 individual liver metastases and 30 individual peritoneal metastases were included in the final results (Supplementary Table S3-S5). The distribution of origins (TD, LNM, primary tumor or a mix of these) was compared between the group of liver and the group of peritoneal metastases using Fisher's exact test. Potential confounding clinicopathological factors were analyzed using the Kruskal-Wallis of Fisher's exact test. P values < 0.05 were considered significant. Full descriptions of the materials and methods are provided in the Supplementary Materials.
Phylogenetic analysis showed that the primary tumor, TD, and LNM could be possible origins of liver metastases. An exemplary phylogenetic tree is shown in Figure 1C, where different subclones gave rise to different LNMs, and several liver metastases with common ancestry were related to the TD. Taken together, TD, LNM, primary tumor or a mix of these were found to be the origin of liver metastases in 23%, 23%, 23% and 30%, respectively (Figure 1D). Several clinicopathological variables were tested for biasing the results, of which only the number of included TDs was significantly different between the liver metastases related to TD and PT (P = 0.03), all other comparisons showed no differences significantly with the number of metastases related to TD (Supplementary Figures S2-S3). Our data show that LNM can form a gateway to liver metastases in 23% of cases, which is in line with an earlier smaller study, where 0-35% of liver metastases were found to be related to LNM [5]. These results are in contrast with the idea that LNM is the main gateway to distant metastases, which is the basis for the current TNM staging system. Importantly, TD were identified as an alternative gateway in 23% of liver metastases, which confirms the prognostic evidence that shows an increased risk of liver metastases in patients with TD [3].
In contrast to liver metastases, peritoneal metastases were most often related to TD with 40% of cases and second most often to the primary tumor with 37%. LNMs or a mix of the different structures formed the origin in 7% and 10% of peritoneal metastases, respectively (Figure 1E). These results provide phylogenetic evidence that supports previous studies showing that the presence of TDs is associated with an increased risk of peritoneal metastases [6].
This study demonstrated a clear difference in the evolution of liver and peritoneal metastases, with a significantly different distribution of origins (P < 0.05, Figure 1D-E) and 40% of peritoneal metastases versus 23% of liver metastases being related to TD. This could be explained by biologically different pathways to metastases. Liver metastases are thought to develop through the invasion-metastasis cascade where tumor cells spread to distant organs via the circulatory system [7]. Both LNMs and TDs formed possible gateways to liver metastases in the phylogenetic analyses and have their own way of accessing the systemic circulation. For LNMs, mouse studies showed that tumor cells could either invade small blood vessels surrounding the lymph node or travel through the lymphatic system and enter the systemic circulation at the thoracic duct [8]. Still, the exact mechanism is being widely debated, and in humans, the mechanism remains unclear. For TDs, it is more widely accepted that they have access to the blood circulation as it is reflected in their histology [4]. In line with literature, our study demonstrated a vascular component in 69% of TD related to liver metastases (Supplementary Figure S4). An alternative to the invasion-metastasis cascade has been proposed for peritoneal metastases involving more direct migration of tumor cells to the peritoneum [7]. We previously showed that the molecular phenotype needed for tumor cells to actively migrate to and invade the peritoneum is overexpressed in TD compared with LNM [9]. Therefore, it is likely that tumor cells with the ability to form TD are also capable of further migration through the serosal surface and invasion of the peritoneum, more so than the tumor cells in LNM.
There are some limitations to this study. Firstly, although all cases complied with the guideline quality of more than 12 sampled lymph nodes per CRC, and TD were scored by two pathologists and an expert researcher, there is a small chance that some TD or LNM were missed during the sampling of resection specimens. Secondly, it would be recommended that all phylogenetic studies be validated using a different method, such as whole genome or exome sequencing, to show whether the results are generalizable and robust [10]. Thirdly, due to time and financial restraints, this study only included the most common metastatic sites in CRC, liver and peritoneum. Including other metastatic sites would provide a more comprehensive overview of the process of metastatic spread in CRC.
In conclusion, with the use of phylogenic analysis, this study shows that both TDs and LNMs can be related to liver or peritoneal metastases in CRC. Moreover, the origin of metastases differs per metastatic site, with liver metastases being equally related to TDs and LNMs and peritoneal metastases being significantly more often related to TDs. Therefore, future research should focus on whether patients with TDs are at increased risk of peritoneal metastases, as this could impact follow-up and treatment decisions. Also, since we showed that a significant number of liver and peritoneal metastases were related to TDs, it should be questioned whether the current method of including TDs as less important than LNMs in the staging for CRC patients is justified. We propose that TDs should merit more attention by including them as equally important to LNMs in the nodal category and continuing to register them for future research.
Conceptualization: Gina Brown, Femke Simmer, Iris Dionne Nagtegaal. Methodology: Nelleke Pietronella Maria Brouwer, Ayse Selcen Oguz Erdogan, Niek Hugen, Femke Simmer, Iris Dionne Nagtegaal. Funding acquisition: Gina Brown, Iris Dionne Nagtegaal. Acquisition and analysis of data: Nelleke Pietronella Maria Brouwer, Ayse Selcen Oguz Erdogan, Shannon van Vliet, Natasja Rutgers. Statistical analysis: Nelleke Pietronella Maria Brouwer, Ayse Selcen Oguz Erdogan, Shannon van Vliet, Natasja Rutgers, Femke Simmer. Material support: Nikki Knijn, Gesina van Lijnschoten, Jessica Juliana Tan, Gina Brown. Writing—original draft: Nelleke Pietronella Maria Brouwer, Ayse Selcen Oguz Erdogan, Niek Hugen, Femke Simmer, Iris Dionne Nagtegaal. Writing—review & editing: Nelleke Pietronella Maria Brouwer, Ayse Selcen Oguz Erdogan, Shannon van Vliet, Natasja Rutgers, Nikki Knijn, Gesina van Lijnschoten, Jessica Juliana Tan, Johannes Hendrik Willem de Wilt, Niek Hugen, Gina Brown, Femke Simmer, Iris Dionne Nagtegaal.
All authors declare no conflicts of interest.
This study was supported by the Dutch Cancer Society (KUN 2019-12640).
The study was performed according to the Dutch “Federa, Human Tissue and Medical Research: Code of Conduct for Responsible Use (2011)” regulations, not requiring patient informed consent. This study was approved by the Ethics Committee (CMO) of the Radboudumc (approval number 2020-7172).
期刊介绍:
Cancer Communications is an open access, peer-reviewed online journal that encompasses basic, clinical, and translational cancer research. The journal welcomes submissions concerning clinical trials, epidemiology, molecular and cellular biology, and genetics.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
