Sameh Hany Emile, Giovanna Dasilva, Nir Horesh, Zoe Garoufalia, Rachel Gefen, Peige Zhou, Mariana Berho, Steven D Wexner
{"title":"Pathologic Outcomes and Survival in Patients with Rectal Cancer and Increased Body Mass Index.","authors":"Sameh Hany Emile, Giovanna Dasilva, Nir Horesh, Zoe Garoufalia, Rachel Gefen, Peige Zhou, Mariana Berho, Steven D Wexner","doi":"10.1159/000541085","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>We assessed the association between increased body mass index (BMI) and rectal cancer outcomes.</p><p><strong>Methods: </strong>We included patients who underwent surgery for stage I-III rectal adenocarcinoma who were divided according to BMI at diagnosis: ideal BMI (18.5-24.9 kg/m2) and increased BMI (≥25 kg/m2). Groups were compared using univariate association analyses relative to baseline characteristics, pathologic outcomes, overall survival (OS), and disease-free survival (DFS). Main outcome measures involved circumferential resection margin (CRM), pathologic TNM stage, total mesorectal incision (TME) grade, OS, and DFS.</p><p><strong>Results: </strong>243 patients (64.6% male; median age 59 years) with a median BMI of 26.3 kg/m2 were included. 62.1% had BMI ≥25 kg/m2. Increased BMI patients had similar proportions of males (66.9% vs. 60.9%; p = 0.407) and comorbidities (ASA III: 47% vs. 37.4%; p = 0.24) to ideal BMI patients. There were no significant differences in cN1-2 stage (p = 0.279) or positive CRM (p = 0.062) rates. The groups had similar complete/near-complete TME, pathologic TN stage, and survival rates. Pathologic and survival outcomes were also similar with a BMI cutoff of 30.</p><p><strong>Conclusions: </strong>There was a trend toward more nodal involvement in preoperative assessment and less CRM involvement in the final pathology of patients with increased BMI. Complete/near-complete TME and survival rates were comparable between the groups.</p>","PeriodicalId":11241,"journal":{"name":"Digestive Surgery","volume":" ","pages":"194-203"},"PeriodicalIF":1.2000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11506326/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Digestive Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1159/000541085","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/23 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: We assessed the association between increased body mass index (BMI) and rectal cancer outcomes.
Methods: We included patients who underwent surgery for stage I-III rectal adenocarcinoma who were divided according to BMI at diagnosis: ideal BMI (18.5-24.9 kg/m2) and increased BMI (≥25 kg/m2). Groups were compared using univariate association analyses relative to baseline characteristics, pathologic outcomes, overall survival (OS), and disease-free survival (DFS). Main outcome measures involved circumferential resection margin (CRM), pathologic TNM stage, total mesorectal incision (TME) grade, OS, and DFS.
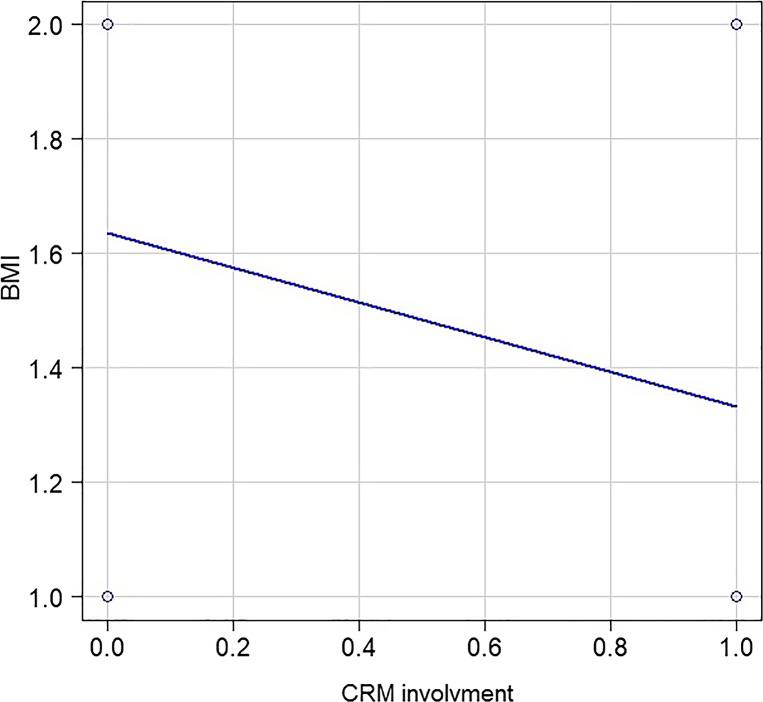
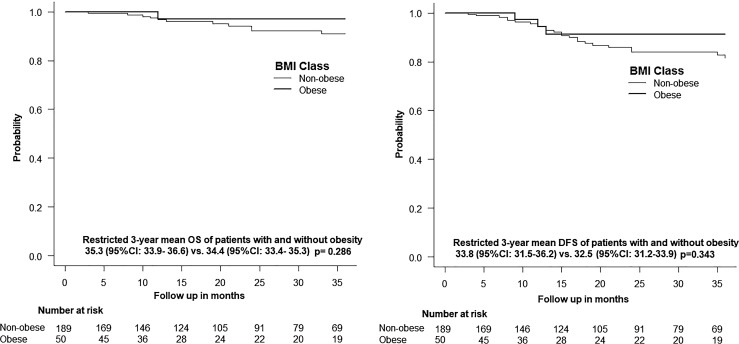
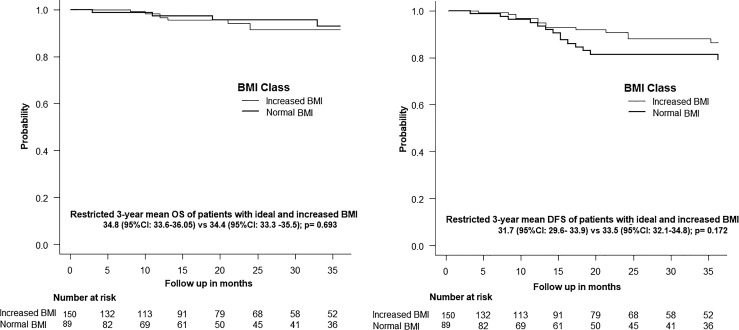
Results: 243 patients (64.6% male; median age 59 years) with a median BMI of 26.3 kg/m2 were included. 62.1% had BMI ≥25 kg/m2. Increased BMI patients had similar proportions of males (66.9% vs. 60.9%; p = 0.407) and comorbidities (ASA III: 47% vs. 37.4%; p = 0.24) to ideal BMI patients. There were no significant differences in cN1-2 stage (p = 0.279) or positive CRM (p = 0.062) rates. The groups had similar complete/near-complete TME, pathologic TN stage, and survival rates. Pathologic and survival outcomes were also similar with a BMI cutoff of 30.
Conclusions: There was a trend toward more nodal involvement in preoperative assessment and less CRM involvement in the final pathology of patients with increased BMI. Complete/near-complete TME and survival rates were comparable between the groups.
期刊介绍:
''Digestive Surgery'' presents a comprehensive overview in the field of gastrointestinal surgery. Interdisciplinary in scope, the journal keeps the specialist aware of advances in all fields that contribute to improvements in the diagnosis and treatment of gastrointestinal disease. Particular emphasis is given to articles that evaluate not only recent clinical developments, especially clinical trials and technical innovations such as new endoscopic and laparoscopic procedures, but also relevant translational research. Each contribution is carefully aligned with the need of the digestive surgeon. Thus, the journal is an important component of the continuing medical education of surgeons who want their practice to benefit from a familiarity with new knowledge in all its dimensions.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
