Sun Woo Nam, Sang-Hwan Do, Jung-Won Hwang, Insun Park, Insung Hwang, Hyo-Seok Na
{"title":"Effects of opioid-sparing general anesthesia on postoperative nausea and vomiting in laparoscopic gynecological surgery.","authors":"Sun Woo Nam, Sang-Hwan Do, Jung-Won Hwang, Insun Park, Insung Hwang, Hyo-Seok Na","doi":"10.4097/kja.24336","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In this study, we aimed to investigate whether opioid-sparing anesthesia (OSA) reduces postoperative nausea and vomiting (PONV) in patients undergoing laparoscopic gynecological surgery.</p><p><strong>Methods: </strong>Adult patients undergoing elective laparoscopic gynecological surgery were randomly assigned to either the opioid-using anesthesia (OUA) or the OSA groups. In the OUA group, remifentanil was administered as an opioid during general anesthesia. In the OSA group, apart from a single dose of 5 μg/kg of alfentanil for tracheal intubation, no other opioids were used. In both groups, a multimodal intravenous non-opioid analgesic regimen was used preferentially in the post-anesthesia care unit (PACU). The primary outcome was the incidence of PONV, assessed by symptoms until the postoperative day 1.</p><p><strong>Results: </strong>A total of 120 patients were included in this study. The incidence of nausea in the PACU was significantly lower in the OSA group compared to in the OUA group (31.7% in the OSA group vs. 51.7% in the OUA group, P = 0.026). Pain scores and the incidence of opioid analgesic administration were lower in the OSA group during PACU stay, resulting in a significantly lower number of patients requiring rescue opioid analgesics (3.3% vs. 18.3%, P = 0.008). There were no significant differences in intraoperative vital signs, hemodynamic interventions, or duration of PACU and hospital stay between the two groups.</p><p><strong>Conclusions: </strong>OSA significantly reduced postoperative nausea, pain scores, and the need for rescue analgesics in the PACU without increasing hemodynamic instability in patients undergoing laparoscopic gynecological surgery.</p>","PeriodicalId":17855,"journal":{"name":"Korean Journal of Anesthesiology","volume":" ","pages":"605-613"},"PeriodicalIF":6.3000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11637591/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean Journal of Anesthesiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4097/kja.24336","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/23 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: In this study, we aimed to investigate whether opioid-sparing anesthesia (OSA) reduces postoperative nausea and vomiting (PONV) in patients undergoing laparoscopic gynecological surgery.
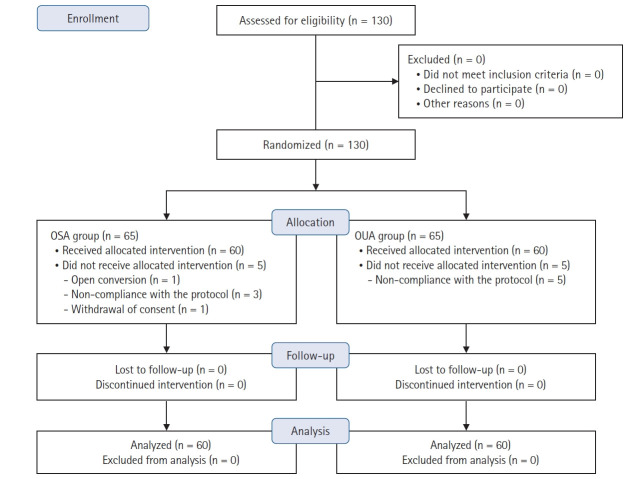
Methods: Adult patients undergoing elective laparoscopic gynecological surgery were randomly assigned to either the opioid-using anesthesia (OUA) or the OSA groups. In the OUA group, remifentanil was administered as an opioid during general anesthesia. In the OSA group, apart from a single dose of 5 μg/kg of alfentanil for tracheal intubation, no other opioids were used. In both groups, a multimodal intravenous non-opioid analgesic regimen was used preferentially in the post-anesthesia care unit (PACU). The primary outcome was the incidence of PONV, assessed by symptoms until the postoperative day 1.
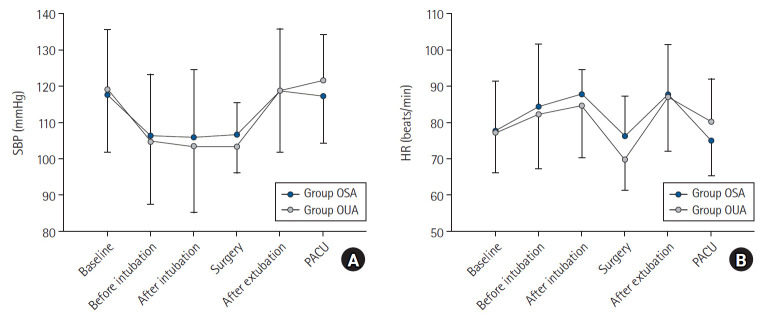
Results: A total of 120 patients were included in this study. The incidence of nausea in the PACU was significantly lower in the OSA group compared to in the OUA group (31.7% in the OSA group vs. 51.7% in the OUA group, P = 0.026). Pain scores and the incidence of opioid analgesic administration were lower in the OSA group during PACU stay, resulting in a significantly lower number of patients requiring rescue opioid analgesics (3.3% vs. 18.3%, P = 0.008). There were no significant differences in intraoperative vital signs, hemodynamic interventions, or duration of PACU and hospital stay between the two groups.
Conclusions: OSA significantly reduced postoperative nausea, pain scores, and the need for rescue analgesics in the PACU without increasing hemodynamic instability in patients undergoing laparoscopic gynecological surgery.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
