Initial empirical antibiotic therapy in kidney transplant recipients with pyelonephritis: A global survey of current practice and opinions across 19 countries on six continents.
Julien Coussement, Shyam B Bansal, Anne Scemla, My H S Svensson, Laura A Barcan, Olivia C Smibert, Wanessa T Clemente, Francisco Lopez-Medrano, Tomer Hoffman, Umberto Maggiore, Concetta Catalano, Luuk Hilbrands, Oriol Manuel, Tinus DU Toit, Terence Kee Yi Shern, Nizamuddin Chowdhury, Ondrej Viklicky, Rainer Oberbauer, Samuel Markowicz, Hannah Kaminski, Matthieu Lafaurie, Ligia C Pierrotti, Tiago L Cerqueira, Dafna Yahav, Nassim Kamar, Camille N Kotton
{"title":"Initial empirical antibiotic therapy in kidney transplant recipients with pyelonephritis: A global survey of current practice and opinions across 19 countries on six continents.","authors":"Julien Coussement, Shyam B Bansal, Anne Scemla, My H S Svensson, Laura A Barcan, Olivia C Smibert, Wanessa T Clemente, Francisco Lopez-Medrano, Tomer Hoffman, Umberto Maggiore, Concetta Catalano, Luuk Hilbrands, Oriol Manuel, Tinus DU Toit, Terence Kee Yi Shern, Nizamuddin Chowdhury, Ondrej Viklicky, Rainer Oberbauer, Samuel Markowicz, Hannah Kaminski, Matthieu Lafaurie, Ligia C Pierrotti, Tiago L Cerqueira, Dafna Yahav, Nassim Kamar, Camille N Kotton","doi":"10.1111/tid.14362","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Despite the burden of pyelonephritis after kidney transplantation, there is no consensus on initial empirical antibiotic management.</p><p><strong>Methods: </strong>We surveyed clinicians throughout the world on their practice and opinions about the initial empirical therapy of post-transplant pyelonephritis, using clinical vignettes. A panel of experts from 19 countries on six continents designed this survey, and invited 2145 clinicians to participate.</p><p><strong>Results: </strong>A total of 721 clinicians completed the survey (response rate: 34%). In the hypothetical case of a kidney transplant recipient admitted with pyelonephritis but not requiring intensive care, most respondents reported initiating either a 3rd-generation cephalosporin (37%) or piperacillin-tazobactam (21%) monotherapy. Several patient-level factors dictated the selection of broader-spectrum antibiotics, including having a recent urine culture showing growth of a resistant organism (85% for extended-spectrum ß-lactamase-producing organisms, 90% for carbapenemase-producing organisms, and 94% for Pseudomonas aeruginosa). Respondents attributed high importance to the appropriateness of empirical therapy, which 87% judged important to prevent mortality. Significant practice and opinion variations were observed between and within countries.</p><p><strong>Conclusion: </strong>High-quality studies are needed to guide the empirical management of post-transplant pyelonephritis. In particular, whether prior urine culture results should systematically be reviewed and considered remains to be determined. Studies are also needed to clarify the relationship between the appropriateness of initial empirical therapy and outcomes of post-transplant pyelonephritis.</p>","PeriodicalId":23318,"journal":{"name":"Transplant Infectious Disease","volume":" ","pages":"e14362"},"PeriodicalIF":2.6000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11666887/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplant Infectious Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/tid.14362","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/26 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Despite the burden of pyelonephritis after kidney transplantation, there is no consensus on initial empirical antibiotic management.
Methods: We surveyed clinicians throughout the world on their practice and opinions about the initial empirical therapy of post-transplant pyelonephritis, using clinical vignettes. A panel of experts from 19 countries on six continents designed this survey, and invited 2145 clinicians to participate.
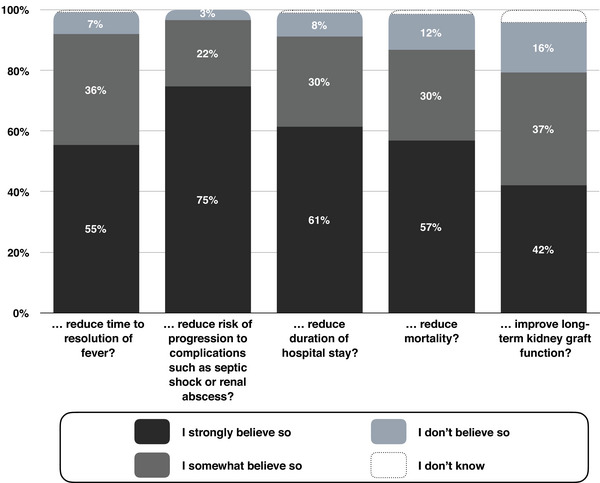
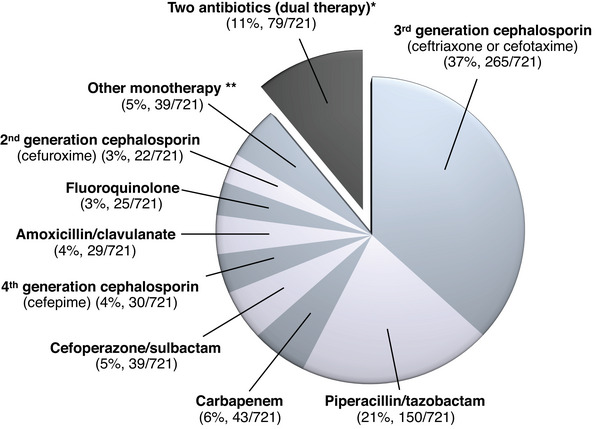
Results: A total of 721 clinicians completed the survey (response rate: 34%). In the hypothetical case of a kidney transplant recipient admitted with pyelonephritis but not requiring intensive care, most respondents reported initiating either a 3rd-generation cephalosporin (37%) or piperacillin-tazobactam (21%) monotherapy. Several patient-level factors dictated the selection of broader-spectrum antibiotics, including having a recent urine culture showing growth of a resistant organism (85% for extended-spectrum ß-lactamase-producing organisms, 90% for carbapenemase-producing organisms, and 94% for Pseudomonas aeruginosa). Respondents attributed high importance to the appropriateness of empirical therapy, which 87% judged important to prevent mortality. Significant practice and opinion variations were observed between and within countries.
Conclusion: High-quality studies are needed to guide the empirical management of post-transplant pyelonephritis. In particular, whether prior urine culture results should systematically be reviewed and considered remains to be determined. Studies are also needed to clarify the relationship between the appropriateness of initial empirical therapy and outcomes of post-transplant pyelonephritis.
期刊介绍:
Transplant Infectious Disease has been established as a forum for presenting the most current information on the prevention and treatment of infection complicating organ and bone marrow transplantation. The point of view of the journal is that infection and allograft rejection (or graft-versus-host disease) are closely intertwined, and that advances in one area will have immediate consequences on the other. The interaction of the transplant recipient with potential microbial invaders, the impact of immunosuppressive strategies on this interaction, and the effects of cytokines, growth factors, and chemokines liberated during the course of infections, rejection, or graft-versus-host disease are central to the interests and mission of this journal.
Transplant Infectious Disease is aimed at disseminating the latest information relevant to the infectious disease complications of transplantation to clinicians and scientists involved in bone marrow, kidney, liver, heart, lung, intestinal, and pancreatic transplantation. The infectious disease consequences and concerns regarding innovative transplant strategies, from novel immunosuppressive agents to xenotransplantation, are very much a concern of this journal. In addition, this journal feels a particular responsibility to inform primary care practitioners in the community, who increasingly are sharing the responsibility for the care of these patients, of the special considerations regarding the prevention and treatment of infection in transplant recipients. As exemplified by the international editorial board, articles are sought throughout the world that address both general issues and those of a more restricted geographic import.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
