Clinically important changes and adverse events with centre-based or home-based pulmonary rehabilitation in chronic respiratory disease: A systematic review and meta-analysis.
Janet Bondarenko, Simone Dal Corso, Michael P Dillon, Sally Singh, Belinda R Miller, Caroline Kein, Anne E Holland, Arwel W Jones
{"title":"Clinically important changes and adverse events with centre-based or home-based pulmonary rehabilitation in chronic respiratory disease: A systematic review and meta-analysis.","authors":"Janet Bondarenko, Simone Dal Corso, Michael P Dillon, Sally Singh, Belinda R Miller, Caroline Kein, Anne E Holland, Arwel W Jones","doi":"10.1177/14799731241277808","DOIUrl":null,"url":null,"abstract":"<p><p><b>Objectives:</b> To determine the proportion of people who achieve minimal clinically important differences (MCID) with centre-based or home-based pulmonary rehabilitation and to synthesise data on adverse events.<b>Methods:</b> Cochrane reviews and electronic databases were searched to identify randomised trials comparing centre-based to home-based pulmonary rehabilitation, or either model to usual care, in people with chronic respiratory disease. Primary outcomes were the proportion of participants achieving MCIDs in exercise capacity and disease-specific quality of life. Secondary outcomes were symptoms and adverse events. Cochrane Risk of Bias 1.0 and GRADE were used to assess the risk of bias and certainty of evidence respectively.<b>Results:</b> Forty-nine trials were eligible. Compared to usual care, a higher proportion of pulmonary rehabilitation participants achieved the MCID for exercise capacity (6MWT: 47% vs 20%, <i>p</i> = 0.11), dyspnoea (43% vs 29%, <i>p</i> = 0.0001), fatigue (48% vs 27%, <i>p</i> = 0.0002) and emotional function (37% vs 25%, <i>p</i> = 0.02), with all of these between group differences statistically significant except for exercise capacity. There were no differences between centre-based and home-based pulmonary rehabilitation in the proportion of participants who achieved MCIDs (34%- 58% across studies). Ninety percent of trials reported no adverse events. Certainty of evidence was low-to- moderate with all outcomes except for CRQ-mastery (centre-based vs home-based pulmonary rehabilitation, or pulmonary rehabilitation vs usual care in COPD), ESWT (pulmonary rehabilitation vs usual care in COPD) and 6MWT (pulmonary rehabilitation vs usual care in bronchiectasis) where evidence was very uncertain.<b>Discussion:</b> Clinically meaningful outcomes are achieved by similar proportions of participants in centre-based and home-based pulmonary rehabilitation, with few adverse events. Reporting of trial outcomes according to MCIDs is necessary for informed decision making regarding pulmonary rehabilitation models.</p>","PeriodicalId":10217,"journal":{"name":"Chronic Respiratory Disease","volume":"21 ","pages":"14799731241277808"},"PeriodicalIF":2.3000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11348370/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Chronic Respiratory Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/14799731241277808","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
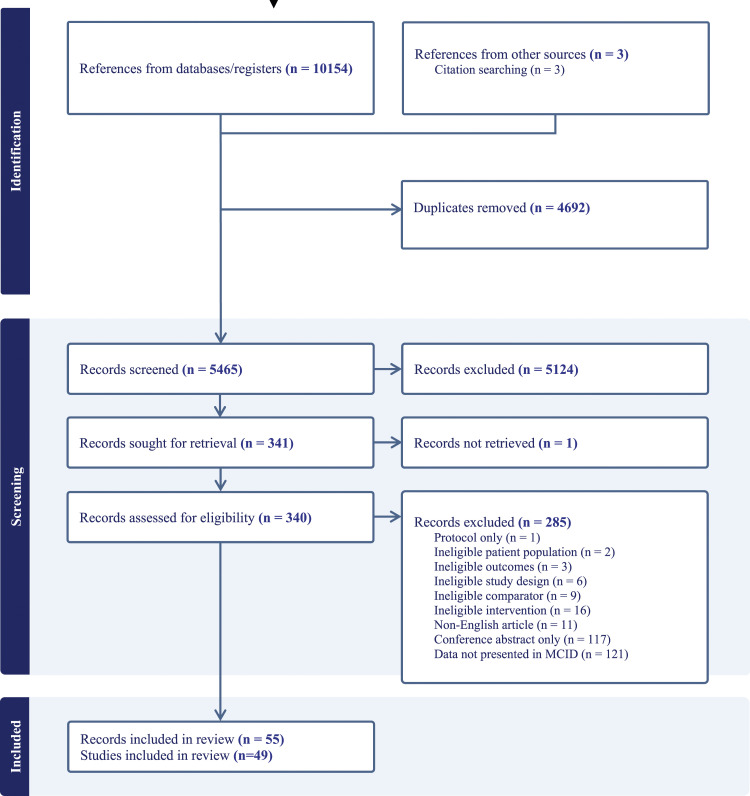
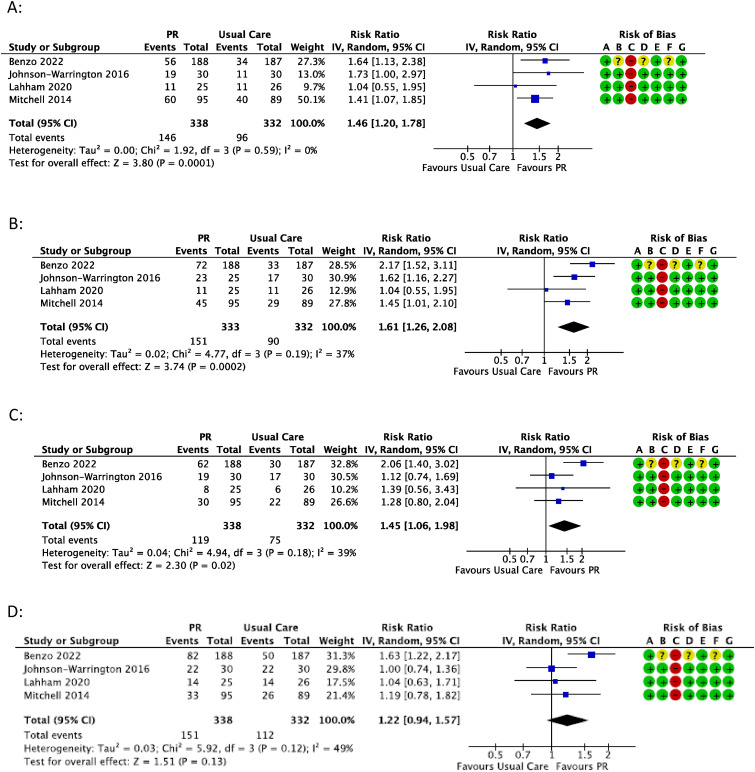
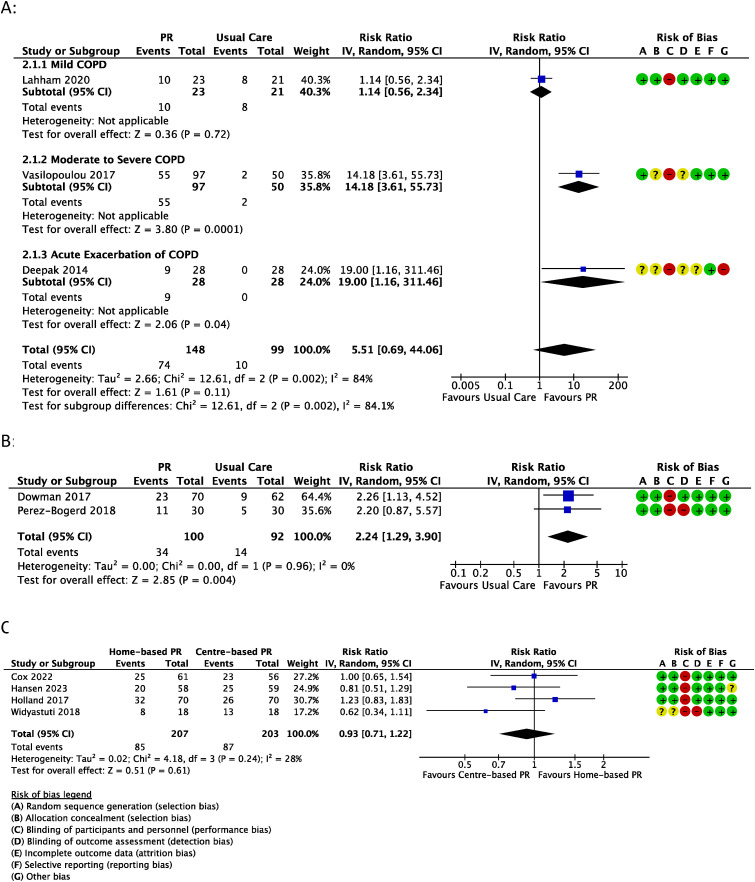
Objectives: To determine the proportion of people who achieve minimal clinically important differences (MCID) with centre-based or home-based pulmonary rehabilitation and to synthesise data on adverse events.Methods: Cochrane reviews and electronic databases were searched to identify randomised trials comparing centre-based to home-based pulmonary rehabilitation, or either model to usual care, in people with chronic respiratory disease. Primary outcomes were the proportion of participants achieving MCIDs in exercise capacity and disease-specific quality of life. Secondary outcomes were symptoms and adverse events. Cochrane Risk of Bias 1.0 and GRADE were used to assess the risk of bias and certainty of evidence respectively.Results: Forty-nine trials were eligible. Compared to usual care, a higher proportion of pulmonary rehabilitation participants achieved the MCID for exercise capacity (6MWT: 47% vs 20%, p = 0.11), dyspnoea (43% vs 29%, p = 0.0001), fatigue (48% vs 27%, p = 0.0002) and emotional function (37% vs 25%, p = 0.02), with all of these between group differences statistically significant except for exercise capacity. There were no differences between centre-based and home-based pulmonary rehabilitation in the proportion of participants who achieved MCIDs (34%- 58% across studies). Ninety percent of trials reported no adverse events. Certainty of evidence was low-to- moderate with all outcomes except for CRQ-mastery (centre-based vs home-based pulmonary rehabilitation, or pulmonary rehabilitation vs usual care in COPD), ESWT (pulmonary rehabilitation vs usual care in COPD) and 6MWT (pulmonary rehabilitation vs usual care in bronchiectasis) where evidence was very uncertain.Discussion: Clinically meaningful outcomes are achieved by similar proportions of participants in centre-based and home-based pulmonary rehabilitation, with few adverse events. Reporting of trial outcomes according to MCIDs is necessary for informed decision making regarding pulmonary rehabilitation models.
期刊介绍:
Chronic Respiratory Disease is a peer-reviewed, open access, scholarly journal, created in response to the rising incidence of chronic respiratory diseases worldwide. It publishes high quality research papers and original articles that have immediate relevance to clinical practice and its multi-disciplinary perspective reflects the nature of modern treatment. The journal provides a high quality, multi-disciplinary focus for the publication of original papers, reviews and commentary in the broad area of chronic respiratory disease, particularly its treatment and management.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
