First-Line Combination with Proteasome Inhibitor-Based Treatment and Zoledronic Acid Is Effective in Reducing Later Fractures in Multiple Myeloma Irrespective of Multiple Myeloma Bone Disease at Diagnosis.
Veera Eskelinen, Elise Nivakoski, Kirsi Launonen, Anu Partanen, Sakari Kakko, Milla E L Kuusisto
{"title":"First-Line Combination with Proteasome Inhibitor-Based Treatment and Zoledronic Acid Is Effective in Reducing Later Fractures in Multiple Myeloma Irrespective of Multiple Myeloma Bone Disease at Diagnosis.","authors":"Veera Eskelinen, Elise Nivakoski, Kirsi Launonen, Anu Partanen, Sakari Kakko, Milla E L Kuusisto","doi":"10.3390/hematolrep16030051","DOIUrl":null,"url":null,"abstract":"<p><p>The present study provides real-world evidence on the treatment of multiple myeloma (MM) bone disease with various bisphosphonates combined for different myeloma-specific treatments as no validated data regarding the best combination treatment for bone disease associated with MM are available. We examined retrospectively 345 MM patients treated with autologous stem cell transplantation in Finland during 1996-2020. The median age of the patients was 60 years with a median follow-up time of 50 months (1-339). At diagnosis, 72.1% of the patients had myeloma-associated bone disease and 45.8% had fractures. Most patients (58.8%) received proteasome inhibitor (PI)-containing treatment at first line. MM bone disease was treated in 91.6% of the patients; 49.9% received zoledronic acid (ZA) and 29.9% pamidronate. Inferior overall survival was associated with MM bone disease at diagnosis (<i>p</i> = 0.005) or a fracture at diagnosis (<i>p</i> = 0.003). A later fracture was identified in 29% of the patients, and in those patients without MM bone disease at diagnosis later fractures were less common after ZA treatment (<i>p</i> = 0.049). PI-based treatment plus ZA (<i>p</i> = 0.019) seemed to be the best combination to prevent later fractures, even though the same patient subgroup was more likely to experience relapse (<i>p</i> = 0.018), and also when excluding patients with previous induction therapy without novel agents (<i>p</i> = 0.008). To conclude, this study suggests that the best therapy to prevent later fractures in MM might be PI-based treatment combined with ZA.</p>","PeriodicalId":12829,"journal":{"name":"Hematology Reports","volume":"16 3","pages":"529-540"},"PeriodicalIF":1.2000,"publicationDate":"2024-08-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11348108/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hematology Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/hematolrep16030051","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
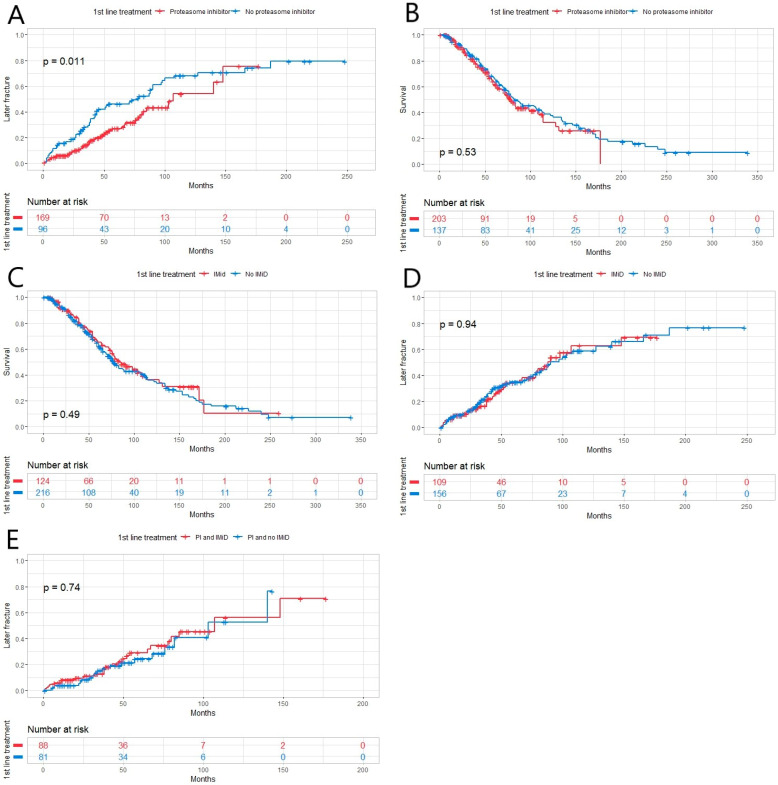
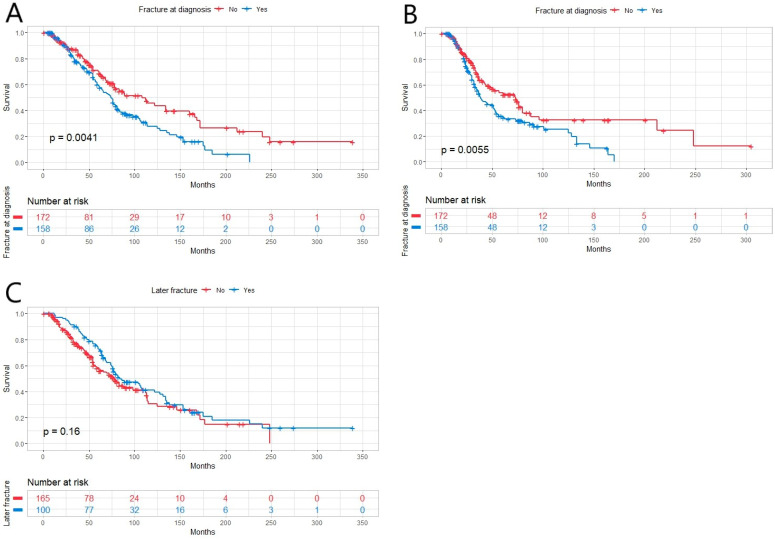
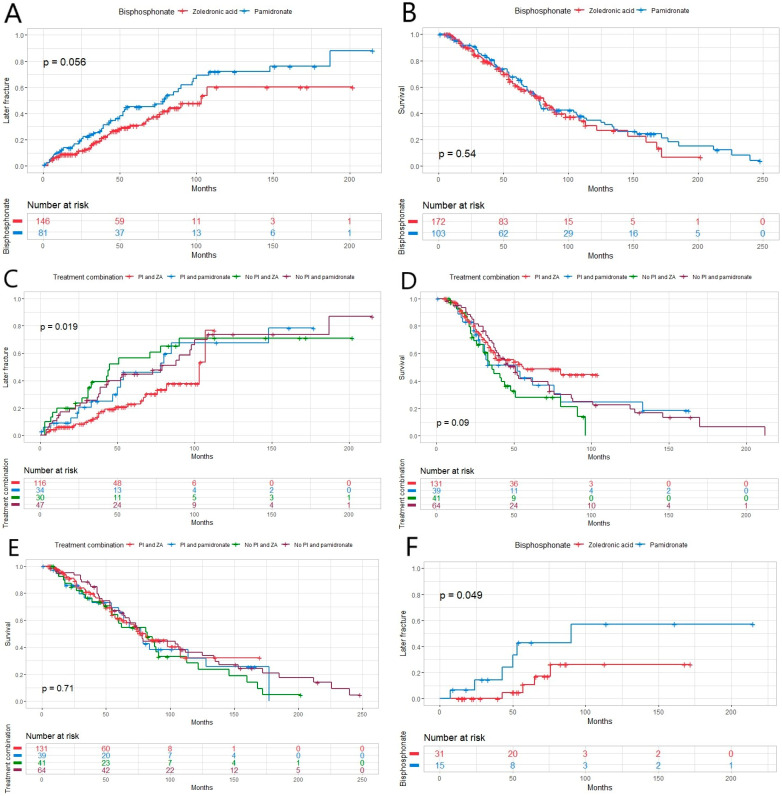
The present study provides real-world evidence on the treatment of multiple myeloma (MM) bone disease with various bisphosphonates combined for different myeloma-specific treatments as no validated data regarding the best combination treatment for bone disease associated with MM are available. We examined retrospectively 345 MM patients treated with autologous stem cell transplantation in Finland during 1996-2020. The median age of the patients was 60 years with a median follow-up time of 50 months (1-339). At diagnosis, 72.1% of the patients had myeloma-associated bone disease and 45.8% had fractures. Most patients (58.8%) received proteasome inhibitor (PI)-containing treatment at first line. MM bone disease was treated in 91.6% of the patients; 49.9% received zoledronic acid (ZA) and 29.9% pamidronate. Inferior overall survival was associated with MM bone disease at diagnosis (p = 0.005) or a fracture at diagnosis (p = 0.003). A later fracture was identified in 29% of the patients, and in those patients without MM bone disease at diagnosis later fractures were less common after ZA treatment (p = 0.049). PI-based treatment plus ZA (p = 0.019) seemed to be the best combination to prevent later fractures, even though the same patient subgroup was more likely to experience relapse (p = 0.018), and also when excluding patients with previous induction therapy without novel agents (p = 0.008). To conclude, this study suggests that the best therapy to prevent later fractures in MM might be PI-based treatment combined with ZA.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
