Giovanni Balato, Vincenzo De Matteo, Amedeo Guarino, Domenico De Mauro, Dario Baldi, Carlo Cavaliere, Marco Salvatore, Mustafa Citak, Massimo Mariconda
{"title":"A comparison between 3D printed models and standard 2D planning in the use of metal block augments in revision knee arthroplasty.","authors":"Giovanni Balato, Vincenzo De Matteo, Amedeo Guarino, Domenico De Mauro, Dario Baldi, Carlo Cavaliere, Marco Salvatore, Mustafa Citak, Massimo Mariconda","doi":"10.52312/jdrs.2024.1591","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>The study focused on the ability to predict the need and size of femoral and tibial augmentation using standard two-dimensional (2D) templates and models created with three-dimensional (3D) printing in surgical planning.</p><p><strong>Patients and methods: </strong>This observational cohort study included 28 consecutive patients (22 females, 6 males; mean age: 71±7.3 years; range, 54 to 82 years) with periprosthetic joint infection recruited between March 2021 and September 2023 undergoing revision total knee arthroplasty revision (TKA). Standard planning was made using calibrated X-ray images. The 3D planning started with computed tomography scans to generate a 3D template of the distal femur and proximal tibia. The model was exported to a 3D printer to produce a patient-specific phantom. The surgery was then simulated on the 3D phantom using revision knee arthroplasty instrumentation to evaluate the appropriate augmentation to use until a correct alignment was obtained.</p><p><strong>Results: </strong>Three-dimensional planning predicted the need for femoral and tibial augments in 22 (78.6%) cases at both the tibial and femoral components, while 2D planning correctly predicted the need for augmentation in 17 (60.7%) for the tibial side and 18 (64.3%) for the femoral side. The Cohen's kappa demonstrated a significant agreement between the 3D planning for the femoral metal block and the intraoperative requirement (kappa=0.553), whereas 2D planning showed only nonsignificant poor agreement (kappa=0.083). In contrast, the agreement between 2D or 3D preoperative planning for tibial augment and the intraoperative requirement was nonsignificant (kappa=0.130 and kappa=0.158, respectively). On the femoral side, 2D planning showed only a fair nonsignificant correlation (r=0.35, p=0.069), whereas 3D planning exhibited substantial agreement with the actual thickness of the implanted augment (r=0.65, p<0.001). On the tibial side, 3D and 2D planning showed substantial agreement with the actual size of implanted augments (3D planning, r=0.73, p<0.001; 2D planning, r=0.69, p<0.001).</p><p><strong>Conclusion: </strong>Prediction based on 3D computed tomography segmentation showed significant agreement with the intraoperative need for augmentations in revision TKA. The results suggest that planning with 3D printed models represents a stronger aid in this kind of surgery rather than standard 2D planning, providing greater accuracy in the prediction of the required augmentation in revision TKA.</p>","PeriodicalId":73560,"journal":{"name":"Joint diseases and related surgery","volume":"35 3","pages":"473-482"},"PeriodicalIF":1.9000,"publicationDate":"2024-08-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11411891/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Joint diseases and related surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.52312/jdrs.2024.1591","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: The study focused on the ability to predict the need and size of femoral and tibial augmentation using standard two-dimensional (2D) templates and models created with three-dimensional (3D) printing in surgical planning.
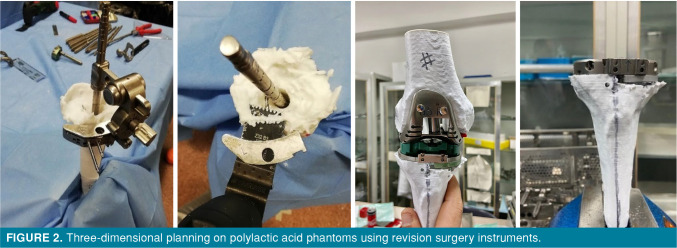
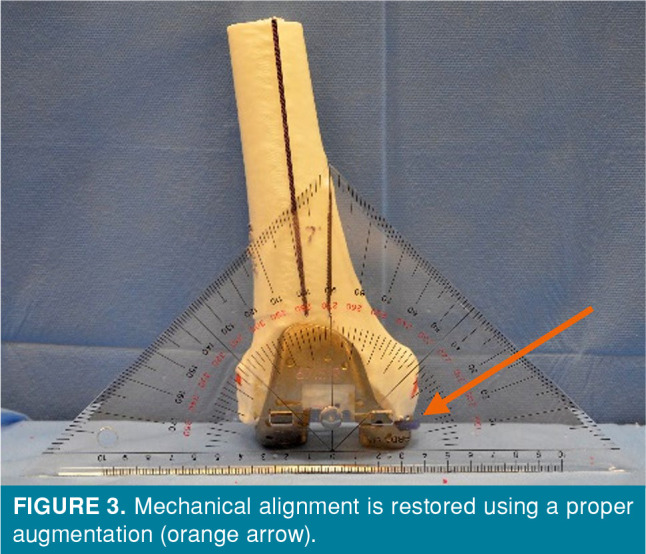
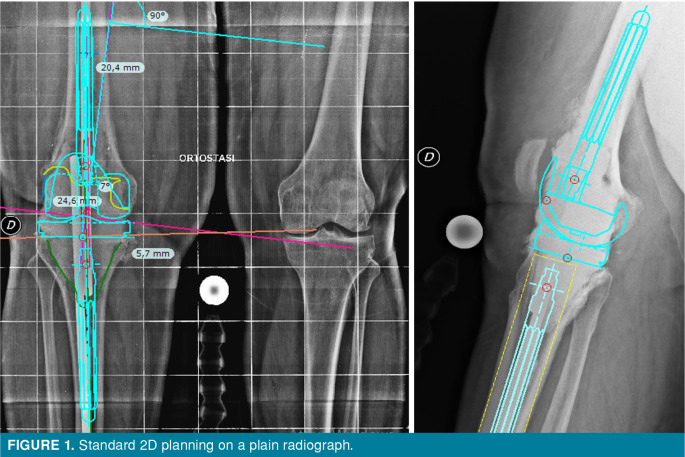
Patients and methods: This observational cohort study included 28 consecutive patients (22 females, 6 males; mean age: 71±7.3 years; range, 54 to 82 years) with periprosthetic joint infection recruited between March 2021 and September 2023 undergoing revision total knee arthroplasty revision (TKA). Standard planning was made using calibrated X-ray images. The 3D planning started with computed tomography scans to generate a 3D template of the distal femur and proximal tibia. The model was exported to a 3D printer to produce a patient-specific phantom. The surgery was then simulated on the 3D phantom using revision knee arthroplasty instrumentation to evaluate the appropriate augmentation to use until a correct alignment was obtained.
Results: Three-dimensional planning predicted the need for femoral and tibial augments in 22 (78.6%) cases at both the tibial and femoral components, while 2D planning correctly predicted the need for augmentation in 17 (60.7%) for the tibial side and 18 (64.3%) for the femoral side. The Cohen's kappa demonstrated a significant agreement between the 3D planning for the femoral metal block and the intraoperative requirement (kappa=0.553), whereas 2D planning showed only nonsignificant poor agreement (kappa=0.083). In contrast, the agreement between 2D or 3D preoperative planning for tibial augment and the intraoperative requirement was nonsignificant (kappa=0.130 and kappa=0.158, respectively). On the femoral side, 2D planning showed only a fair nonsignificant correlation (r=0.35, p=0.069), whereas 3D planning exhibited substantial agreement with the actual thickness of the implanted augment (r=0.65, p<0.001). On the tibial side, 3D and 2D planning showed substantial agreement with the actual size of implanted augments (3D planning, r=0.73, p<0.001; 2D planning, r=0.69, p<0.001).
Conclusion: Prediction based on 3D computed tomography segmentation showed significant agreement with the intraoperative need for augmentations in revision TKA. The results suggest that planning with 3D printed models represents a stronger aid in this kind of surgery rather than standard 2D planning, providing greater accuracy in the prediction of the required augmentation in revision TKA.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
