Testing of a risk-stratified patient decision aid to facilitate shared decision-making for extended postoperative thromboprophylaxis after major abdominal surgery for cancer.
Victoria Ivankovic, Megan Delisle, Dawn Stacey, Jad Abou-Khalil, Fady Balaa, Kimberly A Bertens, Brittany Dingley, Guillaume Martel, Kristen McAlpine, Carolyn Nessim, Shaheer Tadros, Marc Carrier, Rebecca C Auer
{"title":"Testing of a risk-stratified patient decision aid to facilitate shared decision-making for extended postoperative thromboprophylaxis after major abdominal surgery for cancer.","authors":"Victoria Ivankovic, Megan Delisle, Dawn Stacey, Jad Abou-Khalil, Fady Balaa, Kimberly A Bertens, Brittany Dingley, Guillaume Martel, Kristen McAlpine, Carolyn Nessim, Shaheer Tadros, Marc Carrier, Rebecca C Auer","doi":"10.1503/cjs.014722","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Use of extended pharmacologic thromboprophylaxis after major abdominopelvic cancer surgery should depend on best-available scientific evidence and patients' informed preferences. We developed a risk-stratified patient decision aid to facilitate shared decision-making and sought to evaluate its effect on decision-making quality regarding use of extended thromboprophylaxis.</p><p><strong>Methods: </strong>We enrolled patients undergoing major abdominopelvic cancer surgery at an academic tertiary care centre in this pre-post study. We evaluated change in decisional conflict, readiness to decide, decision-making confidence, and change in patient knowledge. Participants were provided the appropriate risk-stratified decision aid (according to their Caprini score) in either the preoperative or postoperative setting. A sample size calculation determined that we required 17 patients to demonstrate whether the decision aid meaningfully reduced decisional conflict. We used the Wilcoxon matched-pairs signed ranks test for interval scaled measures.</p><p><strong>Results: </strong>We included 17 participants. The decision aid significantly reduced decisional conflict (median decisional conflict score 2.37 [range 1.00-3.81] v. 1.3 [range 1.00-3.25], <i>p</i> < 0.01). With the decision aid, participants had high confidence (median 86.4 [range 15.91-100]) and felt highly prepared to make a decision (median 90 [range 55-100]). Median knowledge scores increased from 50% (range 0%-100%) to 75% (range 25%-100%).</p><p><strong>Conclusion: </strong>Our risk-stratified, evidence-based decision aid on extended thromboprophylaxis after major abdominopelvic surgery significantly improved decision-making quality. Further research is needed to evaluate the usability and feasibility of this decision aid in the perioperative setting.</p>","PeriodicalId":9573,"journal":{"name":"Canadian Journal of Surgery","volume":"67 4","pages":"E320-E328"},"PeriodicalIF":2.2000,"publicationDate":"2024-08-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11349336/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1503/cjs.014722","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/1 0:00:00","PubModel":"Print","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Use of extended pharmacologic thromboprophylaxis after major abdominopelvic cancer surgery should depend on best-available scientific evidence and patients' informed preferences. We developed a risk-stratified patient decision aid to facilitate shared decision-making and sought to evaluate its effect on decision-making quality regarding use of extended thromboprophylaxis.
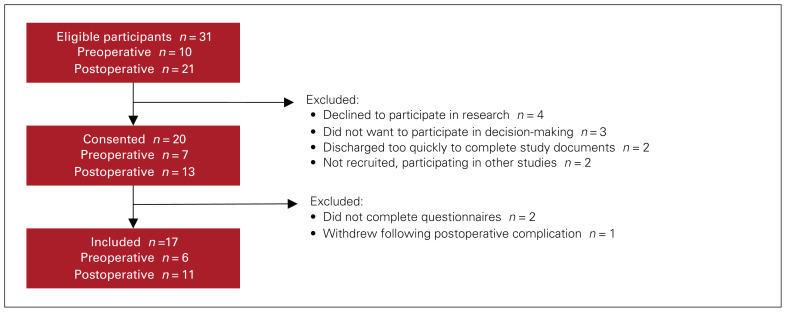
Methods: We enrolled patients undergoing major abdominopelvic cancer surgery at an academic tertiary care centre in this pre-post study. We evaluated change in decisional conflict, readiness to decide, decision-making confidence, and change in patient knowledge. Participants were provided the appropriate risk-stratified decision aid (according to their Caprini score) in either the preoperative or postoperative setting. A sample size calculation determined that we required 17 patients to demonstrate whether the decision aid meaningfully reduced decisional conflict. We used the Wilcoxon matched-pairs signed ranks test for interval scaled measures.
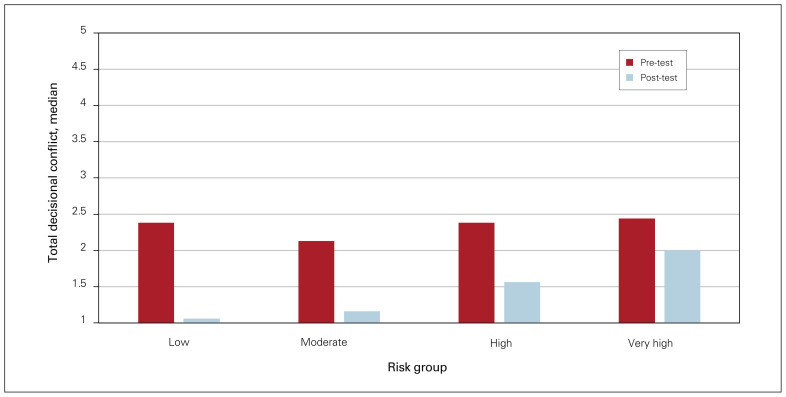
Results: We included 17 participants. The decision aid significantly reduced decisional conflict (median decisional conflict score 2.37 [range 1.00-3.81] v. 1.3 [range 1.00-3.25], p < 0.01). With the decision aid, participants had high confidence (median 86.4 [range 15.91-100]) and felt highly prepared to make a decision (median 90 [range 55-100]). Median knowledge scores increased from 50% (range 0%-100%) to 75% (range 25%-100%).
Conclusion: Our risk-stratified, evidence-based decision aid on extended thromboprophylaxis after major abdominopelvic surgery significantly improved decision-making quality. Further research is needed to evaluate the usability and feasibility of this decision aid in the perioperative setting.
期刊介绍:
The mission of CJS is to contribute to the meaningful continuing medical education of Canadian surgical specialists, and to provide surgeons with an effective vehicle for the dissemination of observations in the areas of clinical and basic science research.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
