{"title":"Isolated Pulmonic Valve Endocarditis: A Rare Clinical Entity.","authors":"Abera Wondie Gizaw, Abilo Tadesse, Hailemaryam Alemu, Abebe Worku, Samuel Dereje Chanie, Getasew Muluken","doi":"10.1177/11795476241277329","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Isolated pulmonic valve endocarditis is a rare heart valve infection, and constitutes about 1% to 2% of all infective endocarditis cases. Modified Duke's criteria were used to diagnose culture negative pulmonic valve endocarditis.</p><p><strong>Case presentation: </strong>A 52-year-old male patient presented with generalized body swelling of 1 month duration associated with prolonged fever, malaise, fatigue, and lassitude. He had productive cough, dyspnea on mild exertion, and reddish discoloration of urine. Upon physical examination, blood pressure (BP) = 140/90 mmHg, pulse rate (PR) = 104 beats per minute, respiratory rate (RR) = 26 breaths per minute, temperature (T<sup>0</sup>) = 38.3°C, and Sp0<sub>2</sub> = 90% at ambient air. He had signs of bilateral pleural effusion. Cardiovascular examination revealed tachycardia, raised jugular venous pressure, murmurs of pulmonic regurgitation, and tricuspid regurgitation. There was grade 2 ascites and bilateral leg edema. On laboratory investigation, there were normochromic, normocytic anemia; raised ESR; positive Rheumatoid factor, elevated serum creatinine; and active urinary sediments on urinalysis. Two sets of blood culture were negative on days 1, 5, and 7. Chest-X-ray showed cardiomegaly with bilateral pleural effusion. ECG revealed sinus tachycardia with regular P-waves and QRS complexes. 2D Transthoracic echo showed vegetation on pulmonic valves, pulmonary valve lesions, dilated right atrium and right ventricle, and elevated right ventricular systolic pressure. Abdominal ultrasound revealed enlarged and echogenic kidneys, and ascites. Definitive diagnosis of PVE was made using modified Duke's criteria which was evidenced by 1 major (echo-proven vegetation on pulmonic valve), and 3 minors (suspected congenital pulmonic stenosis, fever, and immunologic phenomena [acute glomerulonephritis, positive rheumatoid factor]). The patient's clinical condition markedly improved after 2 weeks of intravenous antibiotics and loop diuretics, and discharged home after completing 6 weeks of parenteral antibiotics.</p><p><strong>Conclusion: </strong>Modified Duke's criteria could play a major role in the management decision about diagnosis and empiric treatment of infective endocarditis in the absence of positive bacterial cultures.</p>","PeriodicalId":10357,"journal":{"name":"Clinical Medicine Insights. Case Reports","volume":"17 ","pages":"11795476241277329"},"PeriodicalIF":0.6000,"publicationDate":"2024-08-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11348358/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights. Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11795476241277329","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Isolated pulmonic valve endocarditis is a rare heart valve infection, and constitutes about 1% to 2% of all infective endocarditis cases. Modified Duke's criteria were used to diagnose culture negative pulmonic valve endocarditis.
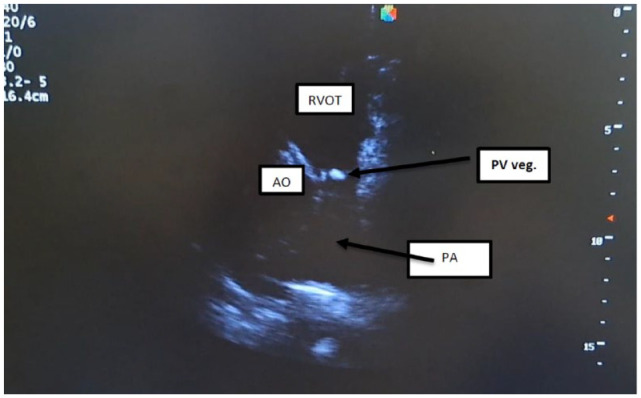
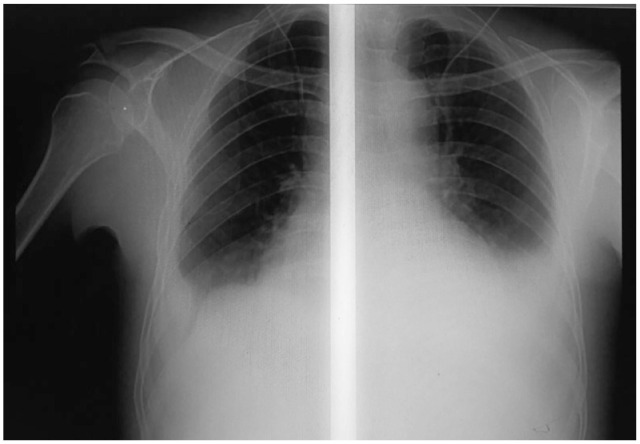
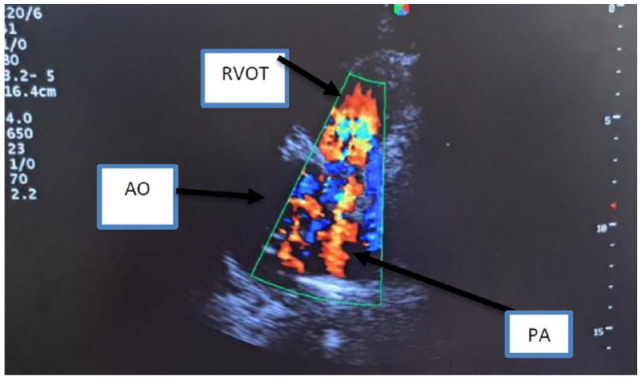
Case presentation: A 52-year-old male patient presented with generalized body swelling of 1 month duration associated with prolonged fever, malaise, fatigue, and lassitude. He had productive cough, dyspnea on mild exertion, and reddish discoloration of urine. Upon physical examination, blood pressure (BP) = 140/90 mmHg, pulse rate (PR) = 104 beats per minute, respiratory rate (RR) = 26 breaths per minute, temperature (T0) = 38.3°C, and Sp02 = 90% at ambient air. He had signs of bilateral pleural effusion. Cardiovascular examination revealed tachycardia, raised jugular venous pressure, murmurs of pulmonic regurgitation, and tricuspid regurgitation. There was grade 2 ascites and bilateral leg edema. On laboratory investigation, there were normochromic, normocytic anemia; raised ESR; positive Rheumatoid factor, elevated serum creatinine; and active urinary sediments on urinalysis. Two sets of blood culture were negative on days 1, 5, and 7. Chest-X-ray showed cardiomegaly with bilateral pleural effusion. ECG revealed sinus tachycardia with regular P-waves and QRS complexes. 2D Transthoracic echo showed vegetation on pulmonic valves, pulmonary valve lesions, dilated right atrium and right ventricle, and elevated right ventricular systolic pressure. Abdominal ultrasound revealed enlarged and echogenic kidneys, and ascites. Definitive diagnosis of PVE was made using modified Duke's criteria which was evidenced by 1 major (echo-proven vegetation on pulmonic valve), and 3 minors (suspected congenital pulmonic stenosis, fever, and immunologic phenomena [acute glomerulonephritis, positive rheumatoid factor]). The patient's clinical condition markedly improved after 2 weeks of intravenous antibiotics and loop diuretics, and discharged home after completing 6 weeks of parenteral antibiotics.
Conclusion: Modified Duke's criteria could play a major role in the management decision about diagnosis and empiric treatment of infective endocarditis in the absence of positive bacterial cultures.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
