Jonghee Han, Su Young Yoon, Junepill Seok, Jin Young Lee, Jin Suk Lee, Jin Bong Ye, Younghoon Sul, Se Heon Kim, Hong Rye Kim
{"title":"Geriatric Trauma Outcome Score for Predicting Mortality among Older Korean Adults with Trauma: Is It Applicable in All Cases?","authors":"Jonghee Han, Su Young Yoon, Junepill Seok, Jin Young Lee, Jin Suk Lee, Jin Bong Ye, Younghoon Sul, Se Heon Kim, Hong Rye Kim","doi":"10.4235/agmr.24.0095","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This study aimed to validate the Geriatric Trauma Outcome Score (GTOS) for predicting mortality associated with trauma in older Korean adults and compare the GTOS with the Trauma and Injury Severity Score (TRISS).</p><p><strong>Methods: </strong>This study included patients aged ≥65 years who visited the Chungbuk National University Hospital Regional Trauma Center between January 2016 and December 2022. We used receiver operating characteristic curves and calibration plots to assess the discrimination and calibration of the scoring systems.</p><p><strong>Results: </strong>Among 3,053 patients, the median age was 77 years, and the mortality rate was 5.2%. The overall GTOS-predicted mortality and 1-TRISS were 5.4% (interquartile range [IQR], 3.7-9.5) and 4.7% (IQR, 4.7-4.7), respectively. The areas under the curves (AUCs) of 1-TRISS and GTOS for the total population were 0.763 (95% confidence interval [CI], 0.719-0.806) and 0.794 (95% CI, 0.755-0.833), respectively. In the Glasgow Coma Scale (GCS) ≤12 group, the in-hospital mortality rate was 27.5% (79 deaths). The GTOS-predicted mortality and 1-TRISS in this group were 18.6% (IQR, 7.5-34.7) and 26.9% (IQR, 11.9-73.1), respectively. The AUCs of 1-TRISS and GTOS for the total population were 0.800 (95% CI, 0.776-0.854) and 0.744 (95% CI, 0.685-0.804), respectively.</p><p><strong>Conclusion: </strong>The GTOS and TRISS demonstrated comparable accuracy in predicting mortality, while the GTOS offered the advantage of simpler calculations. However, the GTOS tended to underestimate mortality in patients with GCS ≤12; thus, its application requires care in such cases.</p>","PeriodicalId":44729,"journal":{"name":"Annals of Geriatric Medicine and Research","volume":" ","pages":"484-490"},"PeriodicalIF":3.2000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11695760/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Geriatric Medicine and Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4235/agmr.24.0095","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/28 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: This study aimed to validate the Geriatric Trauma Outcome Score (GTOS) for predicting mortality associated with trauma in older Korean adults and compare the GTOS with the Trauma and Injury Severity Score (TRISS).
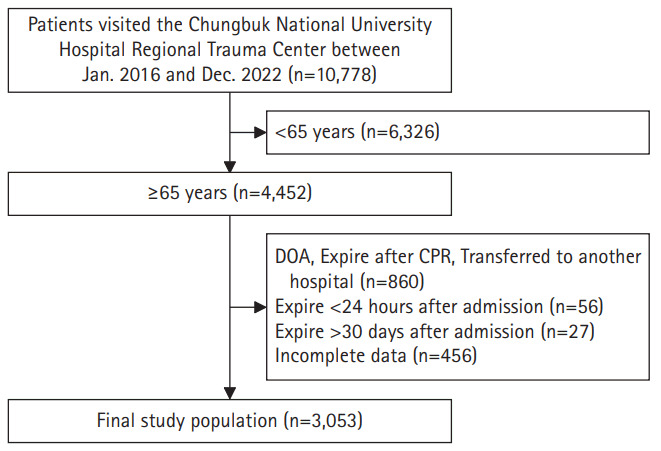
Methods: This study included patients aged ≥65 years who visited the Chungbuk National University Hospital Regional Trauma Center between January 2016 and December 2022. We used receiver operating characteristic curves and calibration plots to assess the discrimination and calibration of the scoring systems.
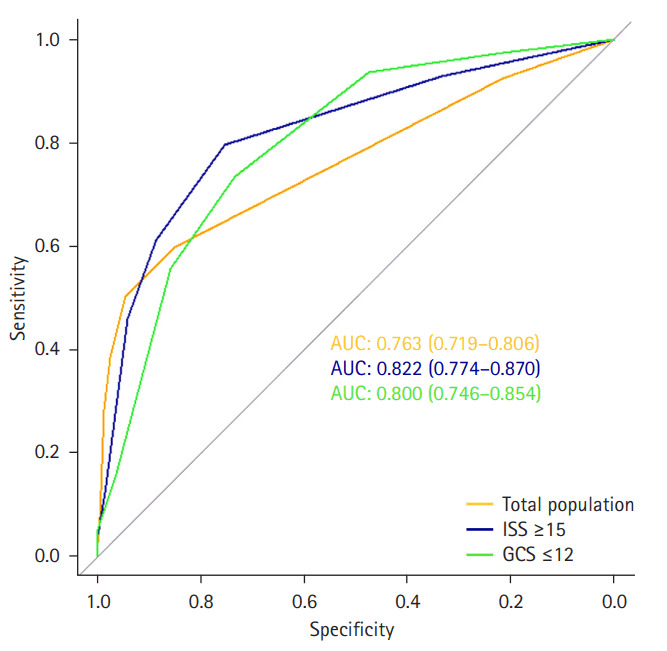
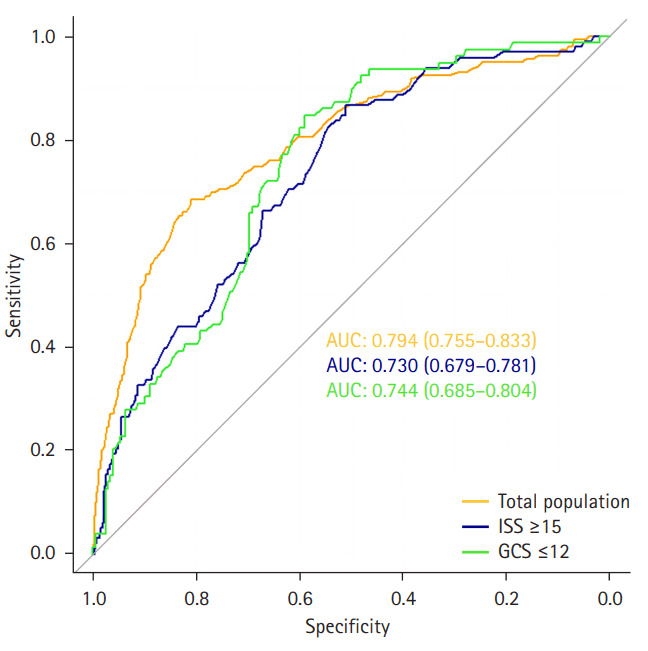
Results: Among 3,053 patients, the median age was 77 years, and the mortality rate was 5.2%. The overall GTOS-predicted mortality and 1-TRISS were 5.4% (interquartile range [IQR], 3.7-9.5) and 4.7% (IQR, 4.7-4.7), respectively. The areas under the curves (AUCs) of 1-TRISS and GTOS for the total population were 0.763 (95% confidence interval [CI], 0.719-0.806) and 0.794 (95% CI, 0.755-0.833), respectively. In the Glasgow Coma Scale (GCS) ≤12 group, the in-hospital mortality rate was 27.5% (79 deaths). The GTOS-predicted mortality and 1-TRISS in this group were 18.6% (IQR, 7.5-34.7) and 26.9% (IQR, 11.9-73.1), respectively. The AUCs of 1-TRISS and GTOS for the total population were 0.800 (95% CI, 0.776-0.854) and 0.744 (95% CI, 0.685-0.804), respectively.
Conclusion: The GTOS and TRISS demonstrated comparable accuracy in predicting mortality, while the GTOS offered the advantage of simpler calculations. However, the GTOS tended to underestimate mortality in patients with GCS ≤12; thus, its application requires care in such cases.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
