David D Berg, Erin A Bohula, Siddharth M Patel, Carlos E Alfonso, Carlos L Alviar, Vivian M Baird-Zars, Christopher F Barnett, Gregory W Barsness, Courtney E Bennett, Sunit-Preet Chaudhry, Christopher B Fordyce, Shahab Ghafghazi, Umesh K Gidwani, Michael J Goldfarb, Jason N Katz, Venu Menon, P Elliott Miller, L Kristin Newby, Alexander I Papolos, Jeong-Gun Park, Matthew J Pierce, Alastair G Proudfoot, Shashank S Sinha, Lakshmi Sridharan, Andrea D Thompson, Sean van Diepen, David A Morrow
{"title":"Epidemiology of cardiogenic shock using the Shock Academic Research Consortium (SHARC) consensus definitions.","authors":"David D Berg, Erin A Bohula, Siddharth M Patel, Carlos E Alfonso, Carlos L Alviar, Vivian M Baird-Zars, Christopher F Barnett, Gregory W Barsness, Courtney E Bennett, Sunit-Preet Chaudhry, Christopher B Fordyce, Shahab Ghafghazi, Umesh K Gidwani, Michael J Goldfarb, Jason N Katz, Venu Menon, P Elliott Miller, L Kristin Newby, Alexander I Papolos, Jeong-Gun Park, Matthew J Pierce, Alastair G Proudfoot, Shashank S Sinha, Lakshmi Sridharan, Andrea D Thompson, Sean van Diepen, David A Morrow","doi":"10.1093/ehjacc/zuae098","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>The Shock Academic Research Consortium (SHARC) recently proposed pragmatic consensus definitions to standardize classification of cardiogenic shock (CS) in registries and clinical trials. We aimed to describe contemporary CS epidemiology using the SHARC definitions in a cardiac intensive care unit (CICU) population.</p><p><strong>Methods and results: </strong>The Critical Care Cardiology Trials Network (CCCTN) is a multinational research network of advanced CICUs coordinated by the TIMI Study Group (Boston, MA). Cardiogenic shock was defined as a cardiac disorder resulting in SBP < 90 mmHg for ≥30 min [or the need for vasopressors, inotropes, or mechanical circulatory support (MCS) to maintain SBP ≥ 90 mmHg] with evidence of hypoperfusion. Primary aetiologic categories included acute myocardial infarction-related CS (AMI-CS), heart failure-related CS (HF-CS), and non-myocardial (secondary) CS. Post-cardiotomy CS was not included. Heart failure-related CS was further subcategorized as de novo vs. acute-on-chronic HF-CS. Patients with both cardiogenic and non-cardiogenic components of shock were classified separately as mixed CS. Of 8974 patients meeting shock criteria (2017-23), 65% had isolated CS and 17% had mixed shock. Among patients with CS (n = 5869), 27% had AMI-CS (65% STEMI), 59% HF-CS (72% acute-on-chronic, 28% de novo), and 14% secondary CS. Patients with AMI-CS and de novo HF-CS were most likely to have had concomitant cardiac arrest (P < 0.001). Patients with AMI-CS and mixed CS were most likely to present in more severe shock stages (SCAI D or E; P < 0.001). Temporary MCS use was highest in AMI-CS (59%). In-hospital mortality was highest in mixed CS (48%), followed by AMI-CS (41%), similar in de novo HF-CS (31%) and secondary CS (31%), and lowest in acute-on-chronic HF-CS (25%; P < 0.001).</p><p><strong>Conclusion: </strong>SHARC consensus definitions for CS classification can be pragmatically applied in contemporary registries and reveal discrete subpopulations of CS with distinct phenotypes and outcomes that may be relevant to clinical practice and future research.</p>","PeriodicalId":11861,"journal":{"name":"European Heart Journal: Acute Cardiovascular Care","volume":" ","pages":"709-714"},"PeriodicalIF":4.6000,"publicationDate":"2024-10-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11518926/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Heart Journal: Acute Cardiovascular Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ehjacc/zuae098","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: The Shock Academic Research Consortium (SHARC) recently proposed pragmatic consensus definitions to standardize classification of cardiogenic shock (CS) in registries and clinical trials. We aimed to describe contemporary CS epidemiology using the SHARC definitions in a cardiac intensive care unit (CICU) population.
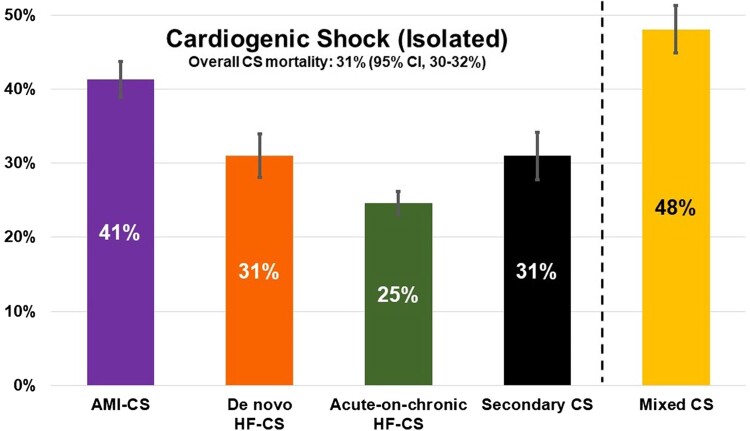
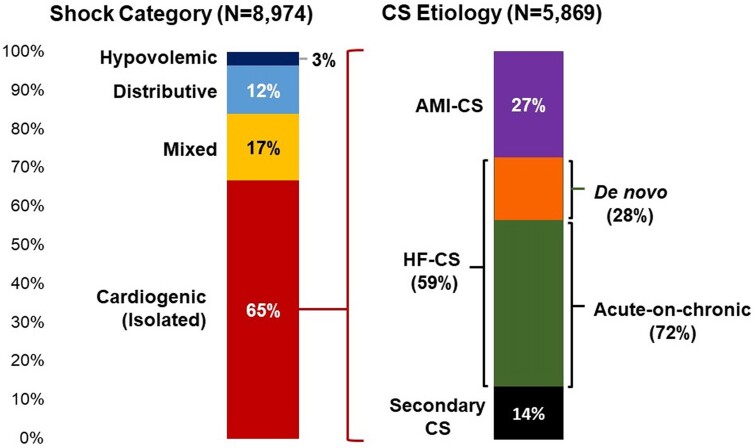
Methods and results: The Critical Care Cardiology Trials Network (CCCTN) is a multinational research network of advanced CICUs coordinated by the TIMI Study Group (Boston, MA). Cardiogenic shock was defined as a cardiac disorder resulting in SBP < 90 mmHg for ≥30 min [or the need for vasopressors, inotropes, or mechanical circulatory support (MCS) to maintain SBP ≥ 90 mmHg] with evidence of hypoperfusion. Primary aetiologic categories included acute myocardial infarction-related CS (AMI-CS), heart failure-related CS (HF-CS), and non-myocardial (secondary) CS. Post-cardiotomy CS was not included. Heart failure-related CS was further subcategorized as de novo vs. acute-on-chronic HF-CS. Patients with both cardiogenic and non-cardiogenic components of shock were classified separately as mixed CS. Of 8974 patients meeting shock criteria (2017-23), 65% had isolated CS and 17% had mixed shock. Among patients with CS (n = 5869), 27% had AMI-CS (65% STEMI), 59% HF-CS (72% acute-on-chronic, 28% de novo), and 14% secondary CS. Patients with AMI-CS and de novo HF-CS were most likely to have had concomitant cardiac arrest (P < 0.001). Patients with AMI-CS and mixed CS were most likely to present in more severe shock stages (SCAI D or E; P < 0.001). Temporary MCS use was highest in AMI-CS (59%). In-hospital mortality was highest in mixed CS (48%), followed by AMI-CS (41%), similar in de novo HF-CS (31%) and secondary CS (31%), and lowest in acute-on-chronic HF-CS (25%; P < 0.001).
Conclusion: SHARC consensus definitions for CS classification can be pragmatically applied in contemporary registries and reveal discrete subpopulations of CS with distinct phenotypes and outcomes that may be relevant to clinical practice and future research.
期刊介绍:
The European Heart Journal - Acute Cardiovascular Care (EHJ-ACVC) offers a unique integrative approach by combining the expertise of the different sub specialties of cardiology, emergency and intensive care medicine in the management of patients with acute cardiovascular syndromes.
Reading through the journal, cardiologists and all other healthcare professionals can access continuous updates that may help them to improve the quality of care and the outcome for patients with acute cardiovascular diseases.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
