Sara Poggi, Teresa Strisciuglio, Assunta Iuliano, Giorgio Spiniello, Vincenzo Schillaci, Alberto Arestia, Gergana Shopova, Armando Mariano Salito, Giovanni Marano, Vincenzo La Rocca, Alessia Agresta, Riccardo Ricciolino, Cosimo Damiano Di Candia, Tommaso Infusino, Marco Micillo, Antonio De Simone, Francesco Solimene, Giuseppe Stabile
{"title":"Peri-procedural anesthesia and patient pain experience in pulmonary vein isolation by means of very high-power short-duration radiofrequency ablation.","authors":"Sara Poggi, Teresa Strisciuglio, Assunta Iuliano, Giorgio Spiniello, Vincenzo Schillaci, Alberto Arestia, Gergana Shopova, Armando Mariano Salito, Giovanni Marano, Vincenzo La Rocca, Alessia Agresta, Riccardo Ricciolino, Cosimo Damiano Di Candia, Tommaso Infusino, Marco Micillo, Antonio De Simone, Francesco Solimene, Giuseppe Stabile","doi":"10.1007/s10840-024-01913-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Very high-power short-duration (vHPSD) temperature-controlled radiofrequency ablation (vHPSD) may reduce ablation times and improve patient tolerability, permitting pulmonary vein (PV) isolation under mild conscious sedation. We evaluated of the anesthetic drugs use and patients' pain experience during vHPSD PV isolation.</p><p><strong>Methods: </strong>Fifty-eight patients, with paroxysmal and persistent atrial fibrillation (AF), treated with QDot Micro catheter and vHPSD (90 w for 4 s) (vHPSD group), were compared with the last 33 patients treated with a surround flow contact force-sensing catheter guided by the ablation index (450 anteriorly at 50 W, 330 posteriorly at 40 W) (AI group). Anesthetic drugs use was compared as well as pain experience, measured using a 0-10 scale.</p><p><strong>Results: </strong>All PVs were acutely isolated. Procedural time (78 ± 10 min vs 84 ± 12 min, p = 0.012), fluoroscopy time (369 ± 139 s vs 441 ± 172 s, p = 0.03), and RF time in the vHPSD group (8.3 ± 2.1 min) were shorter than in the AI group (25 ± 11 min, p < 0.001). Only 4 patients experienced an access site-related vascular complication (groin hematoma). Midazolam was required in 36 (62%) vHPSD group patients vs 31 (94%) AI group patients (p < 0.001). Fentanyl was required in 4 (7%) vHPSD group patients vs 25 (76%) AI group patients (p < 0.001). No patients required general anesthesia. Twenty-two (38%) vHPSD group patients underwent PV isolation without any anesthetic drug. Pain experience was significantly lower in vHPSD group (4.9 ± 2 vs 6.6 ± 1.8, p < 0.001).</p><p><strong>Conclusions: </strong>vHPSD radiofrequency ablation for PVI can be performed under conscious sedation using only benzodiazepine in most of patients without compromising patient pain experience.</p>","PeriodicalId":16202,"journal":{"name":"Journal of Interventional Cardiac Electrophysiology","volume":" ","pages":"141-147"},"PeriodicalIF":2.6000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Interventional Cardiac Electrophysiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10840-024-01913-9","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/30 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Very high-power short-duration (vHPSD) temperature-controlled radiofrequency ablation (vHPSD) may reduce ablation times and improve patient tolerability, permitting pulmonary vein (PV) isolation under mild conscious sedation. We evaluated of the anesthetic drugs use and patients' pain experience during vHPSD PV isolation.
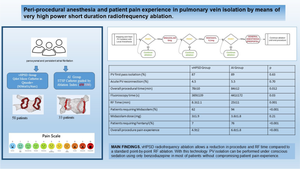
Methods: Fifty-eight patients, with paroxysmal and persistent atrial fibrillation (AF), treated with QDot Micro catheter and vHPSD (90 w for 4 s) (vHPSD group), were compared with the last 33 patients treated with a surround flow contact force-sensing catheter guided by the ablation index (450 anteriorly at 50 W, 330 posteriorly at 40 W) (AI group). Anesthetic drugs use was compared as well as pain experience, measured using a 0-10 scale.
Results: All PVs were acutely isolated. Procedural time (78 ± 10 min vs 84 ± 12 min, p = 0.012), fluoroscopy time (369 ± 139 s vs 441 ± 172 s, p = 0.03), and RF time in the vHPSD group (8.3 ± 2.1 min) were shorter than in the AI group (25 ± 11 min, p < 0.001). Only 4 patients experienced an access site-related vascular complication (groin hematoma). Midazolam was required in 36 (62%) vHPSD group patients vs 31 (94%) AI group patients (p < 0.001). Fentanyl was required in 4 (7%) vHPSD group patients vs 25 (76%) AI group patients (p < 0.001). No patients required general anesthesia. Twenty-two (38%) vHPSD group patients underwent PV isolation without any anesthetic drug. Pain experience was significantly lower in vHPSD group (4.9 ± 2 vs 6.6 ± 1.8, p < 0.001).
Conclusions: vHPSD radiofrequency ablation for PVI can be performed under conscious sedation using only benzodiazepine in most of patients without compromising patient pain experience.
期刊介绍:
The Journal of Interventional Cardiac Electrophysiology is an international publication devoted to fostering research in and development of interventional techniques and therapies for the management of cardiac arrhythmias. It is designed primarily to present original research studies and scholarly scientific reviews of basic and applied science and clinical research in this field. The Journal will adopt a multidisciplinary approach to link physical, experimental, and clinical sciences as applied to the development of and practice in interventional electrophysiology. The Journal will examine techniques ranging from molecular, chemical and pharmacologic therapies to device and ablation technology. Accordingly, original research in clinical, epidemiologic and basic science arenas will be considered for publication. Applied engineering or physical science studies pertaining to interventional electrophysiology will be encouraged. The Journal is committed to providing comprehensive and detailed treatment of major interventional therapies and innovative techniques in a structured and clinically relevant manner. It is directed at clinical practitioners and investigators in the rapidly growing field of interventional electrophysiology. The editorial staff and board reflect this bias and include noted international experts in this area with a wealth of expertise in basic and clinical investigation. Peer review of all submissions, conflict of interest guidelines and periodic editorial board review of all Journal policies have been established.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
