{"title":"Spontaneous atraumatic epipericardial fat necrosis in the context of recent oocyte retrieval and ovarian hyperstimulation syndrome","authors":"Lea Tiffany, Ranjit Singh, Lincoln J Lim","doi":"10.1111/1754-9485.13750","DOIUrl":null,"url":null,"abstract":"<p>Epipericardial fat necrosis (EFN) is a rare benign, self-limiting cause of acute chest pain that mimics serious clinical conditions such as acute coronary syndrome and pulmonary embolism.<span><sup>1</sup></span></p><p>The exact prevalence is unknown due to its rare occurrence.<span><sup>1</sup></span> Seventy to ninety per cent of EFN cases are misdiagnosed and often result in over-investigation and unnecessary invasive biopsies.<span><sup>2</sup></span> Clinically, EFN manifests as acute chest pain, tachycardia and diaphoresis.<span><sup>1, 3</sup></span> Blood results may include elevated D-dimer, CRP and white blood cell counts.<span><sup>1, 3</sup></span> Serum troponin levels are usually within normal limits.<span><sup>1</sup></span></p><p>Given the low specificity of clinical findings and blood tests, computed tomography (CT) is paramount for its opportunistic diagnosis. The main CT findings include an encapsulated or well-circumscribed ovoid fatty lesion with surrounding inflammatory changes within epicardial fat.<span><sup>1, 3</sup></span></p><p>A 39-year-old woman (Gravida-2, Para-1) presented with acute retrosternal chest pain, pleurisy and palpitations 4 days after an egg retrieval procedure. Her past medical history includes stage four endometriosis and mild–moderate ovarian hyperstimulation syndrome (conservatively managed).</p><p>Her medications include Orgalutran (gonadotrophin-releasing hormone antagonist), and Ovidrel trigger shot (beta-human chorionic gonadotrophin) administered 48 h before oocyte retrieval. There was no history of sepsis or preceding trauma.</p><p>The patient was mildly hypertensive (143/92 mmHg) and tachycardic (107 bpm) with good oxygen saturation (98%) and normal respiratory rate (12/min). She had vague focal tenderness on palpation over the left parasternal region. She had an elevated white blood cell count 16.5 (×10<sup>9</sup>/L) (4–11 × 10<sup>9</sup>/L) with neutrophilia 15.5 (×10<sup>9</sup>/L) (2–8 × 10<sup>9</sup>/L), C-reactive protein 56 mg/L (<10 mg/L), D-dimer 14.96 μg/mL (<0.5 μg/mL) and troponin 4 ng/L (<11 ng/L). ECG showed sinus tachycardia. The remaining clinical and biochemical profiles were unremarkable.</p><p>Computed tomography pulmonary angiogram was negative for pulmonary embolism. Within the epicardial fat, there was a 15 × 18 × 10 mm soft tissue density structure with surrounding extensive fat stranding (Figs 1-3). There was no pericardial effusion or overlying chondroosseous fracture.</p><p>The patient was discharged with a working diagnosis of EFN and had a 3-month follow-up CT which demonstrated complete resolution of the ovoid soft tissue structure with mild residual fat stranding (Figs 4,5).</p><p>The exact pathophysiology of EFN is not well understood. Major theories include inflammatory changes within the epipericardial fat and necrosis triggered by torsion of a vascularised fat appendage, Valsalva manoeuvre and trauma.<span><sup>1, 3</sup></span></p><p>Although in vitro fertilisation (IVF)-induced EFN has not been reported in the literature, perhaps inflammation and cardiometabolic changes associated with IVF may have contributed to EFN in our patient. Firstly, inflammatory cascades tend to target highly lipogenic epipericadial fat.<span><sup>4</sup></span> Moreover, high oestrogen concentrations are associated with a transient increase in left ventricular end-diastolic volume and a decrease in left ventricular ejection fraction up to 7 days post-oocyte retrieval, contributing to ventricular hypertrophy/dilation.<span><sup>5</sup></span> Elevated steroid levels in ovarian stimulation also increase susceptibility to arrhythmia.<span><sup>5</sup></span> The exact pathophysiology and association of IVF with EFN remains unclear and should be further explored with future research.</p><p>This case aims to increase the awareness of this rare phenomenon which could be opportunistically diagnosed on CT imaging. This would help with the detection, diagnosis and prevent unnecessary invasive investigations. We also hope that this will widen the differential diagnosis of acute chest pain.</p><p>Magnetic resonance imaging, a superior imaging modality, could be an alternative imaging alternative to distinguish EFN from fat-containing tumours/lipomatous lesions.<span><sup>1</sup></span> Despite its unique fat suppression techniques and potential for further characterisation with post-contrast imaging, the downside would be cost, availability of scan slots and lack of cardiac MRI-trained imaging specialists.</p>","PeriodicalId":16218,"journal":{"name":"Journal of Medical Imaging and Radiation Oncology","volume":"68 6","pages":"696-698"},"PeriodicalIF":1.4000,"publicationDate":"2024-08-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/1754-9485.13750","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Medical Imaging and Radiation Oncology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/1754-9485.13750","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 0
Abstract
Epipericardial fat necrosis (EFN) is a rare benign, self-limiting cause of acute chest pain that mimics serious clinical conditions such as acute coronary syndrome and pulmonary embolism.1
The exact prevalence is unknown due to its rare occurrence.1 Seventy to ninety per cent of EFN cases are misdiagnosed and often result in over-investigation and unnecessary invasive biopsies.2 Clinically, EFN manifests as acute chest pain, tachycardia and diaphoresis.1, 3 Blood results may include elevated D-dimer, CRP and white blood cell counts.1, 3 Serum troponin levels are usually within normal limits.1
Given the low specificity of clinical findings and blood tests, computed tomography (CT) is paramount for its opportunistic diagnosis. The main CT findings include an encapsulated or well-circumscribed ovoid fatty lesion with surrounding inflammatory changes within epicardial fat.1, 3
A 39-year-old woman (Gravida-2, Para-1) presented with acute retrosternal chest pain, pleurisy and palpitations 4 days after an egg retrieval procedure. Her past medical history includes stage four endometriosis and mild–moderate ovarian hyperstimulation syndrome (conservatively managed).
Her medications include Orgalutran (gonadotrophin-releasing hormone antagonist), and Ovidrel trigger shot (beta-human chorionic gonadotrophin) administered 48 h before oocyte retrieval. There was no history of sepsis or preceding trauma.
The patient was mildly hypertensive (143/92 mmHg) and tachycardic (107 bpm) with good oxygen saturation (98%) and normal respiratory rate (12/min). She had vague focal tenderness on palpation over the left parasternal region. She had an elevated white blood cell count 16.5 (×109/L) (4–11 × 109/L) with neutrophilia 15.5 (×109/L) (2–8 × 109/L), C-reactive protein 56 mg/L (<10 mg/L), D-dimer 14.96 μg/mL (<0.5 μg/mL) and troponin 4 ng/L (<11 ng/L). ECG showed sinus tachycardia. The remaining clinical and biochemical profiles were unremarkable.
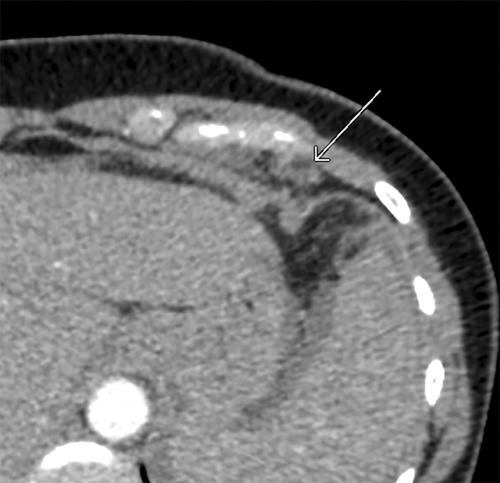
Computed tomography pulmonary angiogram was negative for pulmonary embolism. Within the epicardial fat, there was a 15 × 18 × 10 mm soft tissue density structure with surrounding extensive fat stranding (Figs 1-3). There was no pericardial effusion or overlying chondroosseous fracture.
The patient was discharged with a working diagnosis of EFN and had a 3-month follow-up CT which demonstrated complete resolution of the ovoid soft tissue structure with mild residual fat stranding (Figs 4,5).
The exact pathophysiology of EFN is not well understood. Major theories include inflammatory changes within the epipericardial fat and necrosis triggered by torsion of a vascularised fat appendage, Valsalva manoeuvre and trauma.1, 3
Although in vitro fertilisation (IVF)-induced EFN has not been reported in the literature, perhaps inflammation and cardiometabolic changes associated with IVF may have contributed to EFN in our patient. Firstly, inflammatory cascades tend to target highly lipogenic epipericadial fat.4 Moreover, high oestrogen concentrations are associated with a transient increase in left ventricular end-diastolic volume and a decrease in left ventricular ejection fraction up to 7 days post-oocyte retrieval, contributing to ventricular hypertrophy/dilation.5 Elevated steroid levels in ovarian stimulation also increase susceptibility to arrhythmia.5 The exact pathophysiology and association of IVF with EFN remains unclear and should be further explored with future research.
This case aims to increase the awareness of this rare phenomenon which could be opportunistically diagnosed on CT imaging. This would help with the detection, diagnosis and prevent unnecessary invasive investigations. We also hope that this will widen the differential diagnosis of acute chest pain.
Magnetic resonance imaging, a superior imaging modality, could be an alternative imaging alternative to distinguish EFN from fat-containing tumours/lipomatous lesions.1 Despite its unique fat suppression techniques and potential for further characterisation with post-contrast imaging, the downside would be cost, availability of scan slots and lack of cardiac MRI-trained imaging specialists.
期刊介绍:
Journal of Medical Imaging and Radiation Oncology (formerly Australasian Radiology) is the official journal of The Royal Australian and New Zealand College of Radiologists, publishing articles of scientific excellence in radiology and radiation oncology. Manuscripts are judged on the basis of their contribution of original data and ideas or interpretation. All articles are peer reviewed.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
