Endovascular treatment of contained ruptured internal thoracic artery aneurysm mimicking a tumor in a patient with neurofibromatosis type 1: a case report.
{"title":"Endovascular treatment of contained ruptured internal thoracic artery aneurysm mimicking a tumor in a patient with neurofibromatosis type 1: a case report.","authors":"Ryoma Oda, Daisuke Endo, Takeshi Udagawa, Shingo Okada, Ryohei Kuwatsuru, Minoru Tabata","doi":"10.1186/s40792-024-02002-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>An internal thoracic artery aneurysm (ITAA) is an exceedingly rare condition, with approximately two-thirds of reported cases being iatrogenic pseudoaneurysms. The remainder are attributed to various causes, including vasculitis, connective tissue disease, and neurofibromatosis type 1 (NF-1). NF-1 is an autosomal dominant disorder characterized by distinct clinical manifestations that occasionally include life-threatening vascular complications. Although NF-1 patients may develop various vascular abnormalities, ruptured ITAA is rarely reported, with only seven published cases.</p><p><strong>Case presentation: </strong>A 32-year-old man with NF-1 consulted for a three-day history of persistent left back and upper arm pain. Initial chest radiography indicated left pleural effusion and an opacity at the left lung apex. Computed tomography scan revealed a mass in the left upper mediastinum that was initially suspected to be a tumor. Subsequent contrast-enhanced computed tomography revealed the mass to be a subclavian artery aneurysm. Detailed contrast-enhanced computed tomography with 1-mm slices was performed for surgical planning, identifying the mass as a left ITAA with contained rupture. Given the risk of re-rupture, emergency angiography was performed, which confirmed rupture of the left ITAA without extravasation. The ITAA was successfully treated with multiple microcoils at the proximal and distal ends. The patient had an uneventful recovery and was discharged on the fourth postoperative day.</p><p><strong>Conclusions: </strong>This case highlights the importance of considering vascular lesions in NF-1 patients who present with pleural effusion. It also emphasizes the challenges in diagnosing ITAA and the effectiveness of thin-slice contrast-enhanced computed tomography scans and endovascular treatment.</p>","PeriodicalId":22096,"journal":{"name":"Surgical Case Reports","volume":"10 1","pages":"203"},"PeriodicalIF":0.7000,"publicationDate":"2024-08-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11362441/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40792-024-02002-9","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: An internal thoracic artery aneurysm (ITAA) is an exceedingly rare condition, with approximately two-thirds of reported cases being iatrogenic pseudoaneurysms. The remainder are attributed to various causes, including vasculitis, connective tissue disease, and neurofibromatosis type 1 (NF-1). NF-1 is an autosomal dominant disorder characterized by distinct clinical manifestations that occasionally include life-threatening vascular complications. Although NF-1 patients may develop various vascular abnormalities, ruptured ITAA is rarely reported, with only seven published cases.
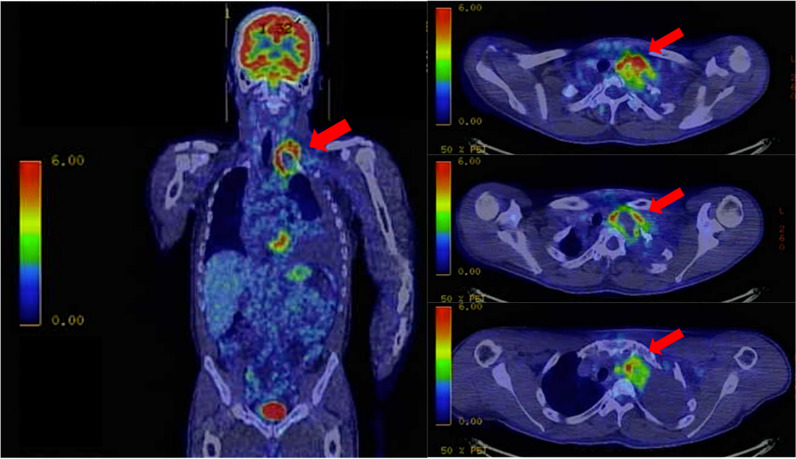
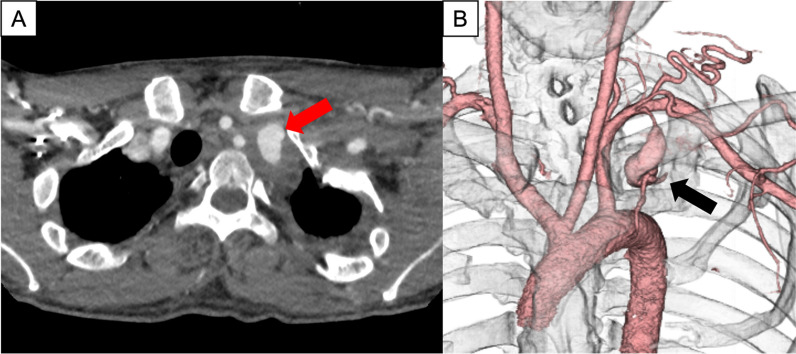
Case presentation: A 32-year-old man with NF-1 consulted for a three-day history of persistent left back and upper arm pain. Initial chest radiography indicated left pleural effusion and an opacity at the left lung apex. Computed tomography scan revealed a mass in the left upper mediastinum that was initially suspected to be a tumor. Subsequent contrast-enhanced computed tomography revealed the mass to be a subclavian artery aneurysm. Detailed contrast-enhanced computed tomography with 1-mm slices was performed for surgical planning, identifying the mass as a left ITAA with contained rupture. Given the risk of re-rupture, emergency angiography was performed, which confirmed rupture of the left ITAA without extravasation. The ITAA was successfully treated with multiple microcoils at the proximal and distal ends. The patient had an uneventful recovery and was discharged on the fourth postoperative day.
Conclusions: This case highlights the importance of considering vascular lesions in NF-1 patients who present with pleural effusion. It also emphasizes the challenges in diagnosing ITAA and the effectiveness of thin-slice contrast-enhanced computed tomography scans and endovascular treatment.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
