Karim Yatim, Ayman Al Jurdi, Christopher El Mouhayyar, Leela Morena, Frank E Hullekes, Ruchama Verhoeff, Guilherme T Ribas, Daniel S Pearson, Leonardo V Riella
{"title":"Safety and Efficacy of a Preemptive Mycophenolate Mofetil Dose Reduction Strategy in Kidney Transplant Recipients.","authors":"Karim Yatim, Ayman Al Jurdi, Christopher El Mouhayyar, Leela Morena, Frank E Hullekes, Ruchama Verhoeff, Guilherme T Ribas, Daniel S Pearson, Leonardo V Riella","doi":"10.1097/TXD.0000000000001697","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>There are no high-quality data to guide long-term mycophenolate mofetil (MMF) dosing in kidney transplant recipients (KTRs) to balance the long-term risks of allograft rejection with that of infections and malignancy. At our center, KTRs are managed with either a \"preemptive\" dose reduction strategy, where the MMF dose is reduced after the first year before the development of adverse events, or with a \"reactive\" dosing strategy, where they are maintained on the same MMF dose and only reduced if they develop an adverse event. We hypothesized that a preemptive MMF dosing strategy after the first year of transplantation is associated with decreased infections without increasing alloimmune complications.</p><p><strong>Methods: </strong>We conducted a retrospective cohort study of all KTRs receiving MMF from January 1, 2015, to December 31, 2020. The primary outcome was the incidence of infections requiring hospitalization.</p><p><strong>Results: </strong>One hundred forty-two KTRs met the inclusion criteria, of whom 44 (31%) were in the preemptive group and 98 (69%) were in the reactive group. The median follow-up was 4 y (interquartile range, 3.8-4.0). Multivariable analysis showed that a preemptive MMF dose reduction strategy was associated with a lower risk of infections requiring hospitalization (adjusted hazard ratio = 0.39; 95% confidence interval, 0.16-0.92). There was no difference in graft loss, rejection, or estimated glomerular filtration rate slope.</p><p><strong>Conclusions: </strong>Preemptive MMF dose reduction in KTRs may be an effective strategy to prevent infections without increasing the risk of allograft rejection. Randomized clinical trials are needed to confirm these findings.</p>","PeriodicalId":23225,"journal":{"name":"Transplantation Direct","volume":"10 9","pages":"e1697"},"PeriodicalIF":1.9000,"publicationDate":"2024-08-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11365660/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplantation Direct","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/TXD.0000000000001697","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"TRANSPLANTATION","Score":null,"Total":0}
引用次数: 0
Abstract
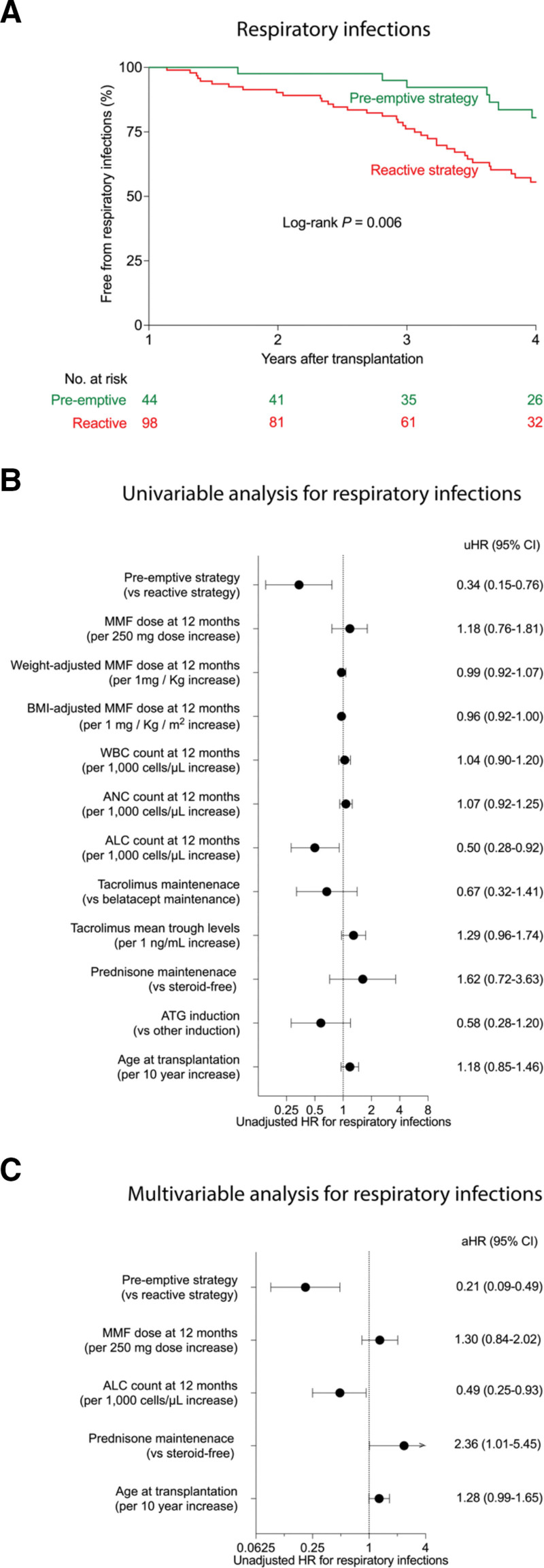
Background: There are no high-quality data to guide long-term mycophenolate mofetil (MMF) dosing in kidney transplant recipients (KTRs) to balance the long-term risks of allograft rejection with that of infections and malignancy. At our center, KTRs are managed with either a "preemptive" dose reduction strategy, where the MMF dose is reduced after the first year before the development of adverse events, or with a "reactive" dosing strategy, where they are maintained on the same MMF dose and only reduced if they develop an adverse event. We hypothesized that a preemptive MMF dosing strategy after the first year of transplantation is associated with decreased infections without increasing alloimmune complications.
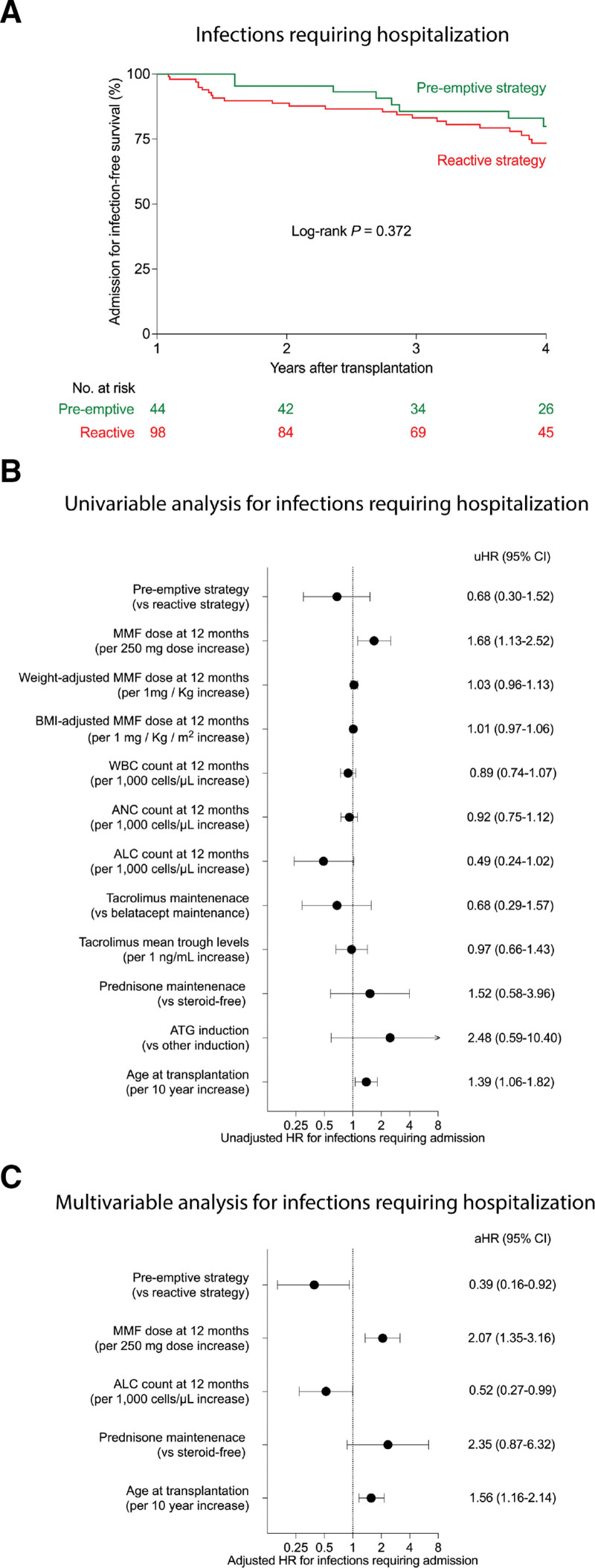
Methods: We conducted a retrospective cohort study of all KTRs receiving MMF from January 1, 2015, to December 31, 2020. The primary outcome was the incidence of infections requiring hospitalization.
Results: One hundred forty-two KTRs met the inclusion criteria, of whom 44 (31%) were in the preemptive group and 98 (69%) were in the reactive group. The median follow-up was 4 y (interquartile range, 3.8-4.0). Multivariable analysis showed that a preemptive MMF dose reduction strategy was associated with a lower risk of infections requiring hospitalization (adjusted hazard ratio = 0.39; 95% confidence interval, 0.16-0.92). There was no difference in graft loss, rejection, or estimated glomerular filtration rate slope.
Conclusions: Preemptive MMF dose reduction in KTRs may be an effective strategy to prevent infections without increasing the risk of allograft rejection. Randomized clinical trials are needed to confirm these findings.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
