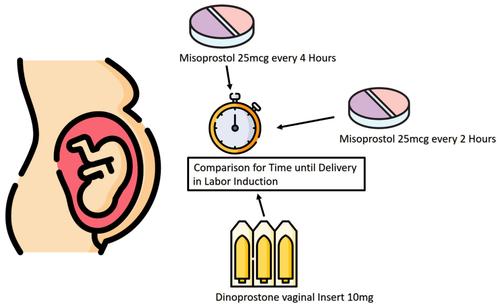
Labor induction exhibits considerable variations in protocols and medication regimens. Limited studies compare vaginal dinoprostone inserts with different oral misoprostol dosages, considering parity influence. This study explores the distinctions among 10 mg vaginal dinoprostone inserts and oral misoprostol 25 μg every 2 and every 4 h for labor induction, stratified by parity.
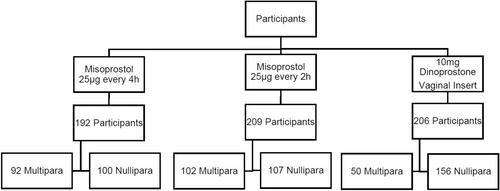
This retrospective cohort study involved 607 participants across two hospitals. The primary outcome, time from induction to delivery, and secondary outcomes, including mode of delivery and maternal and fetal safety, were assessed.
Patient characteristics revealed differences in indication for labor induction, with the dinoprostone cohort having fewer post-term and premature rupture of membranes cases but more intrauterine growth restriction/small-for-gestational age. Both oral misoprostol regimens showed a shorter time to delivery interval compared to the dinoprostone cohort (median: 1380 min [IQR 1381.0] and 1127.0 min [IQR 1214.0] vs 1631.5 [IQR 1736.2], p < 0.001 and p = 0.014). Only the difference between oral misoprostol q2h and vaginal dinoprostone remained significant for nulliparous but not multiparous women, losing significance over all the population after adjusting for confounding factors. The proportion of women giving birth within 24 h did not significantly differ between misoprostol q2h and dinoprostone after adjusting for confounders. When comparing misoprostol q4h with dinoprostone after confounder adjustment, an increased time to delivery interval for misoprostol q4h was found (p = 0.001). Both oral misoprostol regimens exhibited fewer meconium-stained liquor (miso q4h: OR 0.44, miso q2h: OR 0.34) and cesarean sections (miso q4h: OR 0.48, miso q2h: OR 0.53) compared to dinoprostone, even after adjustment for confounders.
Our study suggests that oral misoprostol 25 μg q4h is less effective than 10 mg vaginal dinoprostone for labor induction if parity and indication for induction are adjusted for, particularly in multiparous women. In terms of side effects, oral misoprostol regimens seem superior to vaginal dinoprostone. Our data support the individualized use of different agents for labor induction according to parity, indication for induction, bishop score, and women's preference.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
