{"title":"Factors Associated With Sacubitril/Valsartan Continuation and the Methods of Combining Heart Failure Medications in Patients With Heart Failure.","authors":"Erika Iwasaki, Noriko Kohyama, Mayumi Inamoto, Michiru Nagao, Tomiko Sunaga, Hiroshi Suzuki, Mio Ebato, Mari Kogo","doi":"10.1177/10600280241277354","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Sacubitril/valsartan (SV) is recommended for patients with heart failure (HF). In addition, a combination of 4 HF medications, including SV, is recommended in patients with HF with reduced ejection fraction (HFrEF). However, evidence on the characteristics of patients who could continue SV and its initiation methods is limited.</p><p><strong>Objective: </strong>To investigate the factors associated with SV continuation and methods of combining HF medications.</p><p><strong>Methods: </strong>This retrospective cohort study included HF patients who initiated with SV at our institution. The endpoint was SV continuation for 6 months after its initiation. Multivariate analysis was used to extract factors associated with SV continuation. The relationship between the methods of combining HF medications (renin-angiotensin system inhibitors, beta-blockers, mineralocorticoid receptor antagonists, or sodium-glucose cotransporter 2 inhibitors), including the number of HF medications, their combination patterns, and the timing of their initiation, and SV continuation was examined in patients with HFrEF.</p><p><strong>Results: </strong>Of 186 eligible patients, 68.8% had HFrEF, and 79.0% continued SV for 6 months. Significant factors associated with SV continuation were albumin ≥ 3.5 g/dL (odds ratio, 4.81; 95% confidence interval, 2.19-10.59), body mass index (BMI) ≥ 18.5 kg/m<sup>2</sup> (4.17; 1.10-15.85), and systolic blood pressure (SBP) ≥ 110 mmHg (2.66; 1.12-6.28). In patients with HFrEF, the proportion of HF medications not initiated simultaneously with SV was significantly higher in the continuation group than in the discontinuation group (67.3% vs 33.3%, <i>P</i> = 0.002). The number of HF medications and their combination patterns were not significantly associated with SV continuation.</p><p><strong>Conclusion and relevance: </strong>Albumin, BMI, and SBP are useful indicators for selecting patients who are likely to continue SV. In addition, initiating only SV without simultaneously initiating other HF medications in patients with HFrEF may lead to SV continuation.</p>","PeriodicalId":7933,"journal":{"name":"Annals of Pharmacotherapy","volume":" ","pages":"301-310"},"PeriodicalIF":2.3000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11874506/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Pharmacotherapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/10600280241277354","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/4 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Sacubitril/valsartan (SV) is recommended for patients with heart failure (HF). In addition, a combination of 4 HF medications, including SV, is recommended in patients with HF with reduced ejection fraction (HFrEF). However, evidence on the characteristics of patients who could continue SV and its initiation methods is limited.
Objective: To investigate the factors associated with SV continuation and methods of combining HF medications.
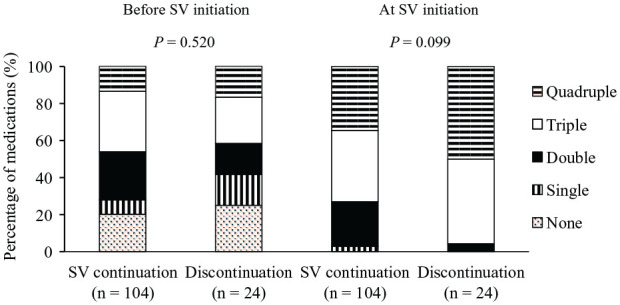
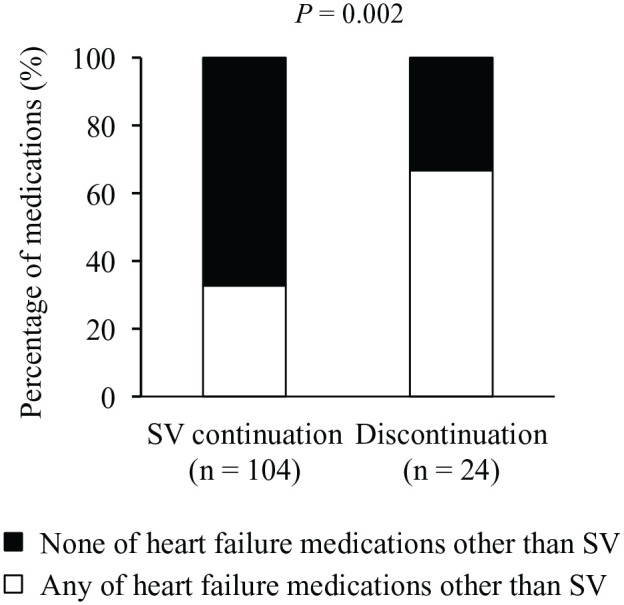
Methods: This retrospective cohort study included HF patients who initiated with SV at our institution. The endpoint was SV continuation for 6 months after its initiation. Multivariate analysis was used to extract factors associated with SV continuation. The relationship between the methods of combining HF medications (renin-angiotensin system inhibitors, beta-blockers, mineralocorticoid receptor antagonists, or sodium-glucose cotransporter 2 inhibitors), including the number of HF medications, their combination patterns, and the timing of their initiation, and SV continuation was examined in patients with HFrEF.
Results: Of 186 eligible patients, 68.8% had HFrEF, and 79.0% continued SV for 6 months. Significant factors associated with SV continuation were albumin ≥ 3.5 g/dL (odds ratio, 4.81; 95% confidence interval, 2.19-10.59), body mass index (BMI) ≥ 18.5 kg/m2 (4.17; 1.10-15.85), and systolic blood pressure (SBP) ≥ 110 mmHg (2.66; 1.12-6.28). In patients with HFrEF, the proportion of HF medications not initiated simultaneously with SV was significantly higher in the continuation group than in the discontinuation group (67.3% vs 33.3%, P = 0.002). The number of HF medications and their combination patterns were not significantly associated with SV continuation.
Conclusion and relevance: Albumin, BMI, and SBP are useful indicators for selecting patients who are likely to continue SV. In addition, initiating only SV without simultaneously initiating other HF medications in patients with HFrEF may lead to SV continuation.
期刊介绍:
Annals of Pharmacotherapy (AOP) is a peer-reviewed journal that advances pharmacotherapy throughout the world by publishing high-quality research and review articles to achieve the most desired health outcomes.The articles provide cutting-edge information about the most efficient, safe and cost-effective pharmacotherapy for the treatment and prevention of various illnesses. This journal is a member of the Committee on Publication Ethics (COPE). Average time from submission to first decision: 14 days



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
