Early Antibiotic De-escalation in Patients With Severe Infections Due to Bloodstream Infection by Enterobacterales: A Post Hoc Analysis of a Prospective Multicentre Cohort
Francesc Escrihuela-Vidal , Zaira R. Palacios-Baena , Josune Goikoetxea Agirre , María Teresa Pérez-Rodríguez , José María Reguera Iglesias , Jordi Cuquet Pedragosa , Leticia Sánchez Gómez , Lucía Boix-Palop , Alberto Bahamonde Carrasco , Clara Natera-Kindelán , Jonathan Fernández-Suárez , Alfredo Jover-Sáenz , Alejandro Smithson Amat , Alfonso del Arco Jiménez , Juan Manuel Sánchez Calvo , Andrés Martín-Aspas , Pedro María Martínez Pérez-Crespo , Inmaculada López-Hernández , Jesús Rodríguez-Baño , Luis Eduardo López-Cortés , Isabel Reche
{"title":"Early Antibiotic De-escalation in Patients With Severe Infections Due to Bloodstream Infection by Enterobacterales: A Post Hoc Analysis of a Prospective Multicentre Cohort","authors":"Francesc Escrihuela-Vidal , Zaira R. Palacios-Baena , Josune Goikoetxea Agirre , María Teresa Pérez-Rodríguez , José María Reguera Iglesias , Jordi Cuquet Pedragosa , Leticia Sánchez Gómez , Lucía Boix-Palop , Alberto Bahamonde Carrasco , Clara Natera-Kindelán , Jonathan Fernández-Suárez , Alfredo Jover-Sáenz , Alejandro Smithson Amat , Alfonso del Arco Jiménez , Juan Manuel Sánchez Calvo , Andrés Martín-Aspas , Pedro María Martínez Pérez-Crespo , Inmaculada López-Hernández , Jesús Rodríguez-Baño , Luis Eduardo López-Cortés , Isabel Reche","doi":"10.1016/j.ijantimicag.2024.107317","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><div>Data about antibiotic de-escalation in sepsis associated with the bloodstream and caused by Enterobacterales are scarce. The objectives of this study are to identify factors associated with early de-escalation and to analyse the impact of de-escalation on mortality in patients with Enterobacterales bloodstream infection (BSI) with a Sequential Organ Failure Assessment (SOFA) score ≥ 2.</div></div><div><h3>Methods</h3><div>A prospective, multicentre cohort study was performed including episodes of BSI due to Enterobacterales and a SOFA score ≥ 2 who were receiving an active antipseudomonal β-lactam; the isolate should be susceptible to at least 1 narrower-spectrum antibiotic. Variables associated with de-escalation were identified using logistic binary regression. The association of de-escalation with 30-day mortality was investigated. Confounding was controlled by calculating a propensity score used as covariate, as matching variable, and for inverse probability treatment weighting.</div></div><div><h3>Results</h3><div>Of the 582 patients included, de-escalation was performed in 311 (53.4%). Neutropenia (adjusted odds ratio [aOR] = 0.37; 95% confidence interval [95% CI] = 0.18–0.75), central venous catheter (aOR = 0.52; 95% CI = 0.32–0.83), and extended-spectrum β-lactamase (ESBL)–producing isolate (aOR = 0.28; 95% CI = 0.17–0.48) were negatively associated with de-escalation, and urinary tract source was positively associated (aOR = 2.27; 95% CI = 1.56–3.33). The 30-day mortality was 6.8% (21 patients) in de-escalated patients and 14.4% (39) in not de-escalated patients (relative risk, 0.63; 95% CI = 0.44–0.89). In multivariate analysis including the propensity score, de-escalation was not associated with mortality (AOR = 0.98; 95% CI = 0.39–2.47) and was protective in the case of urinary or biliary tract source (AOR = 0.31, 95% CI = 0.09–1.06). Matched and inverse probability treatment weighting analysis showed similar results.</div></div><div><h3>Conclusions</h3><div>These results suggest that early de-escalation from antipseudomonal β-lactams is safe in patients with Enterobacterales bacteremia and SOFA ≥ 2.</div></div>","PeriodicalId":13818,"journal":{"name":"International Journal of Antimicrobial Agents","volume":"64 5","pages":"Article 107317"},"PeriodicalIF":4.6000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Antimicrobial Agents","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0924857924002334","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/2 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
Background
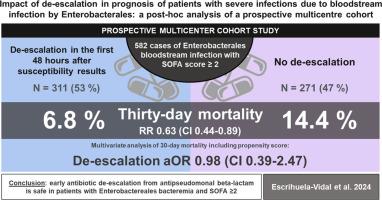
Data about antibiotic de-escalation in sepsis associated with the bloodstream and caused by Enterobacterales are scarce. The objectives of this study are to identify factors associated with early de-escalation and to analyse the impact of de-escalation on mortality in patients with Enterobacterales bloodstream infection (BSI) with a Sequential Organ Failure Assessment (SOFA) score ≥ 2.
Methods
A prospective, multicentre cohort study was performed including episodes of BSI due to Enterobacterales and a SOFA score ≥ 2 who were receiving an active antipseudomonal β-lactam; the isolate should be susceptible to at least 1 narrower-spectrum antibiotic. Variables associated with de-escalation were identified using logistic binary regression. The association of de-escalation with 30-day mortality was investigated. Confounding was controlled by calculating a propensity score used as covariate, as matching variable, and for inverse probability treatment weighting.
Results
Of the 582 patients included, de-escalation was performed in 311 (53.4%). Neutropenia (adjusted odds ratio [aOR] = 0.37; 95% confidence interval [95% CI] = 0.18–0.75), central venous catheter (aOR = 0.52; 95% CI = 0.32–0.83), and extended-spectrum β-lactamase (ESBL)–producing isolate (aOR = 0.28; 95% CI = 0.17–0.48) were negatively associated with de-escalation, and urinary tract source was positively associated (aOR = 2.27; 95% CI = 1.56–3.33). The 30-day mortality was 6.8% (21 patients) in de-escalated patients and 14.4% (39) in not de-escalated patients (relative risk, 0.63; 95% CI = 0.44–0.89). In multivariate analysis including the propensity score, de-escalation was not associated with mortality (AOR = 0.98; 95% CI = 0.39–2.47) and was protective in the case of urinary or biliary tract source (AOR = 0.31, 95% CI = 0.09–1.06). Matched and inverse probability treatment weighting analysis showed similar results.
Conclusions
These results suggest that early de-escalation from antipseudomonal β-lactams is safe in patients with Enterobacterales bacteremia and SOFA ≥ 2.
期刊介绍:
The International Journal of Antimicrobial Agents is a peer-reviewed publication offering comprehensive and current reference information on the physical, pharmacological, in vitro, and clinical properties of individual antimicrobial agents, covering antiviral, antiparasitic, antibacterial, and antifungal agents. The journal not only communicates new trends and developments through authoritative review articles but also addresses the critical issue of antimicrobial resistance, both in hospital and community settings. Published content includes solicited reviews by leading experts and high-quality original research papers in the specified fields.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
