Several factors that predict the outcome of large B-cell lymphoma patients who relapse/progress after chimeric antigen receptor (CAR) T-cell therapy can be identified before cell administration
Alice Sýkorová, František Folber, Kamila Polgárová, Heidi Móciková, Juraj Ďuraš, Kateřina Steinerová, Aleš Obr, Adriana Heindorfer, Miriam Ladická, Ľubica Lukáčová, Erika Čellárová, Ivana Plameňová, David Belada, Andrea Janíková, Marek Trněný, Tereza Jančárková, Vít Procházka, Andrej Vranovský, Margaréta Králiková, Jan Vydra, Lukáš Smolej, Ľuboš Drgoňa, Martin Sedmina, Eva Čermáková, Robert Pytlík
{"title":"Several factors that predict the outcome of large B-cell lymphoma patients who relapse/progress after chimeric antigen receptor (CAR) T-cell therapy can be identified before cell administration","authors":"Alice Sýkorová, František Folber, Kamila Polgárová, Heidi Móciková, Juraj Ďuraš, Kateřina Steinerová, Aleš Obr, Adriana Heindorfer, Miriam Ladická, Ľubica Lukáčová, Erika Čellárová, Ivana Plameňová, David Belada, Andrea Janíková, Marek Trněný, Tereza Jančárková, Vít Procházka, Andrej Vranovský, Margaréta Králiková, Jan Vydra, Lukáš Smolej, Ľuboš Drgoňa, Martin Sedmina, Eva Čermáková, Robert Pytlík","doi":"10.1002/cam4.70138","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Aim</h3>\n \n <p>The aim of this study was to analyse the outcomes of patients with large B-cell lymphoma (LBCL) treated with chimeric antigen receptor T-cell therapy (CAR-Tx), with a focus on outcomes after CAR T-cell failure, and to define the risk factors for rapid progression and further treatment.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>We analysed 107 patients with LBCL from the Czech Republic and Slovakia who were treated in ≥3rd-line with tisagenlecleucel or axicabtagene ciloleucel between 2019 and 2022.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>The overall response rate (ORR) was 60%, with a 50% complete response (CR) rate. The median progression-free survival (PFS) and overall survival (OS) were 4.3 and 26.4 months, respectively. Sixty-three patients (59%) were refractory or relapsed after CAR-Tx. Of these patients, 39 received radiotherapy or systemic therapy, with an ORR of 22% (CR 8%). The median follow-up of surviving patients in whom treatment failed was 10.6 months. Several factors predicting further treatment administration and outcomes were present even before CAR-Tx. Risk factors for not receiving further therapy after CAR-Tx failure were high lactate dehydrogenase (LDH) levels before apheresis, extranodal involvement (EN), high ferritin levels before lymphodepletion (LD) and ECOG PS >1 at R/P. The median OS-2 (from R/P after CAR-Tx) was 6.7 months (6-month 57.9%) for treated patients and 0.4 months (6-month 4.2%) for untreated patients (<i>p</i> < 0.001). The median PFS-2 (from R/P after CAR-Tx) was 3.2 months (6-month 28.5%) for treated patients. The risk factors for a shorter PFS-2 (<i>n</i> = 39) included: CRP > limit of the normal range (LNR) before LD, albumin < LNR and ECOG PS > 1 at R/P. All these factors, together with LDH > LNR before LD and EN involvement at R/P, predicted OS-2 for treated patients.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Our findings allow better stratification of CAR-Tx candidates and stress the need for a proactive approach (earlier restaging, intervention after partial remission achievement).</p>\n </section>\n </div>","PeriodicalId":139,"journal":{"name":"Cancer Medicine","volume":"13 17","pages":""},"PeriodicalIF":3.1000,"publicationDate":"2024-09-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cam4.70138","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cam4.70138","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Aim
The aim of this study was to analyse the outcomes of patients with large B-cell lymphoma (LBCL) treated with chimeric antigen receptor T-cell therapy (CAR-Tx), with a focus on outcomes after CAR T-cell failure, and to define the risk factors for rapid progression and further treatment.
Methods
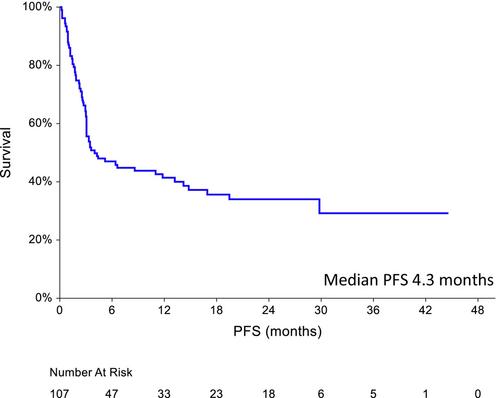
We analysed 107 patients with LBCL from the Czech Republic and Slovakia who were treated in ≥3rd-line with tisagenlecleucel or axicabtagene ciloleucel between 2019 and 2022.
Results
The overall response rate (ORR) was 60%, with a 50% complete response (CR) rate. The median progression-free survival (PFS) and overall survival (OS) were 4.3 and 26.4 months, respectively. Sixty-three patients (59%) were refractory or relapsed after CAR-Tx. Of these patients, 39 received radiotherapy or systemic therapy, with an ORR of 22% (CR 8%). The median follow-up of surviving patients in whom treatment failed was 10.6 months. Several factors predicting further treatment administration and outcomes were present even before CAR-Tx. Risk factors for not receiving further therapy after CAR-Tx failure were high lactate dehydrogenase (LDH) levels before apheresis, extranodal involvement (EN), high ferritin levels before lymphodepletion (LD) and ECOG PS >1 at R/P. The median OS-2 (from R/P after CAR-Tx) was 6.7 months (6-month 57.9%) for treated patients and 0.4 months (6-month 4.2%) for untreated patients (p < 0.001). The median PFS-2 (from R/P after CAR-Tx) was 3.2 months (6-month 28.5%) for treated patients. The risk factors for a shorter PFS-2 (n = 39) included: CRP > limit of the normal range (LNR) before LD, albumin < LNR and ECOG PS > 1 at R/P. All these factors, together with LDH > LNR before LD and EN involvement at R/P, predicted OS-2 for treated patients.
Conclusion
Our findings allow better stratification of CAR-Tx candidates and stress the need for a proactive approach (earlier restaging, intervention after partial remission achievement).
期刊介绍:
Cancer Medicine is a peer-reviewed, open access, interdisciplinary journal providing rapid publication of research from global biomedical researchers across the cancer sciences. The journal will consider submissions from all oncologic specialties, including, but not limited to, the following areas:
Clinical Cancer Research
Translational research ∙ clinical trials ∙ chemotherapy ∙ radiation therapy ∙ surgical therapy ∙ clinical observations ∙ clinical guidelines ∙ genetic consultation ∙ ethical considerations
Cancer Biology:
Molecular biology ∙ cellular biology ∙ molecular genetics ∙ genomics ∙ immunology ∙ epigenetics ∙ metabolic studies ∙ proteomics ∙ cytopathology ∙ carcinogenesis ∙ drug discovery and delivery.
Cancer Prevention:
Behavioral science ∙ psychosocial studies ∙ screening ∙ nutrition ∙ epidemiology and prevention ∙ community outreach.
Bioinformatics:
Gene expressions profiles ∙ gene regulation networks ∙ genome bioinformatics ∙ pathwayanalysis ∙ prognostic biomarkers.
Cancer Medicine publishes original research articles, systematic reviews, meta-analyses, and research methods papers, along with invited editorials and commentaries. Original research papers must report well-conducted research with conclusions supported by the data presented in the paper.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
