Helena J Teede, Karen Best, Frank H Bloomfield, Alan Cass, Paul Cohen, Sue Crengle, Tiffany Harris-Brown, Stephen Jan, David W Johnson, Samantha Keogh, Anne McKenzie, Philippa Middleton, Sandra Peake, Hashim Periyalil, Paul A Scuffham, Angela Scheppokat, Greg R Sharplin, Steve Webb
{"title":"Implementability and impact in clinical research and the role of clinical trial networks","authors":"Helena J Teede, Karen Best, Frank H Bloomfield, Alan Cass, Paul Cohen, Sue Crengle, Tiffany Harris-Brown, Stephen Jan, David W Johnson, Samantha Keogh, Anne McKenzie, Philippa Middleton, Sandra Peake, Hashim Periyalil, Paul A Scuffham, Angela Scheppokat, Greg R Sharplin, Steve Webb","doi":"10.5694/mja2.52444","DOIUrl":null,"url":null,"abstract":"<p>The Australian Clinical Trials Alliance (ACTA) impact and implementation reference group has published guidance on clinical trial planning, design, conduct and reporting, to optimise the impact of late-phase trials.<span><sup>1</sup></span> It is critical that clinical trials are designed, executed and reported on so that the generated evidence can be implemented and applied to improve practice, health systems and policy (defined as <i>implementability</i>).<span><sup>1</sup></span> This is particularly important for late-phase trials as results from these trials guide stakeholder decisions on adoption or removal of candidate interventions from practice and policy. The results can also be used to guide implementation, potentially supplemented by other study types. In some cases, decisions on candidate interventions may be based on a single trial, although more commonly, they are based on the synthesis of evidence from multiple trials. If the results of positive late-phase trials are not put into effect, the community benefit, impact and return on investment are lost. Therefore, to reduce wastage and optimise value to the community, who is both the funder and beneficiary of research, we need to maximise the impact of trials. This impact includes health and economic benefits and requires trials to be designed for implementability.<span><sup>2-4</sup></span></p><p>Implementability is key to trial design and delivery, independent of the results of the trial. Impact is dependent on intervention efficacy and implementability. Late-phase trials should incorporate implementability and be designed to be useful to their diverse end users (including organisations, governments, clinicians and consumers).</p><p>Characteristics that contribute to implementability include concepts around trials that are embedded in clinical care and are pragmatic, focused on informing clinical practice and policy and considering real-world investigators, recruitment, participants, intervention, delivery and outcomes. The PRECIS-2 framework (PRagmatic Explanatory Continuum Indicator Summary framework) indicates where a trial sits on the spectrum between the explanatory “Can this intervention work under ideal conditions?” to the pragmatic “Does this intervention work under usual conditions?”. This framework highlights the vital need to identify, involve and co-design or tailor trial design to the needs of end users.<span><sup>5</sup></span> The Consolidated Framework for Implementation Research (CFIR) and similar tools are also useful to guide design and evaluation of implementation research.<span><sup>6, 7</sup></span> In implementability, key trial design considerations include eligibility and exclusion criteria, setting, requirement for a skilled workforce or specialised equipment and extent of data collection. Similarly, trial design contributes to both embedding and implementability; with the need to recognise potential differences between strategies to promote trial efficiency, and those to promote implementability of trial findings.</p><p>The important steps for progressing interventions through to implementation into practice, health services and policy are shown in the Box.</p><p>These steps align with the Australian Academy of Health and Medical Sciences report<span><sup>8</sup></span> emphasising the importance of embedding research into health care, and the vital role of workforce and infrastructure in achieving this vision. The report also highlights the important role of National Health and Medical Research Council accredited research translation centres (RTCs) in implementation. The RTCs encompass most research, education and hospital services nationally and are well positioned to support clinical trial networks and enable implementation.<span><sup>9</sup></span></p><p>Trials should be co-designed with end users, including consumers, who have experience and understanding of current practice.<span><sup>10</sup></span> It is acknowledged that in some circumstances opportunities for co-design may be limited, such as in industry-sponsored trials. Pre-trial work with end users can establish relevance and the priority of research questions and appropriate outcome measures. Formal processes can be useful<span><sup>11</sup></span> such as Delphi and nominal group techniques, although these need to be appropriate to the local context.</p><p>End points must be carefully chosen, including those of value to end users, and the minimum clinically important differences in end points considered. In addition, the minimum public health significant difference, which defines the relationship between a meaningful effect size and the public health disease burden, should be taken into account. For example, a major effect size (such as a cure for an inborn error of metabolism) in a rare disease may be just as important as minor effect sizes in common diseases (as this might cure a baby at birth and avoid lifetime costs and gain a lifetime of productivity).</p><p>The feasibility of intervention delivery should be established before a late-phase trial. This can be assessed via a systematic review of existing evidence (which may establish the merit for implementation of a particular approach to treating a health problem), as well as pilot studies. Regulatory approvals or burden should also be considered for implementation of drug or device interventions, alongside required skills and resources.</p><p>To optimise generalisability, consideration should be given to the population to which the results of the trial apply. The selected population should be as broad as possible, and entry criteria should be easily interpreted, using easily accessible information available to clinicians in routine practice, and participants in community-based trials. If the candidate intervention is targeted to a clinical setting, trial sites should be broadly representative of the centres that provide care to the key population groups in which the intervention would be implemented post-trial. For population-based studies, community-based recruitment and decentralised trial designs should be considered. If implementation will be beyond tertiary or quaternary hospitals, then the trial should be conducted to include this setting.</p><p>Inclusion criteria should be broad and exclusion criteria as limited as possible. Research burden and complexity from additional factors such as research-only or largely unavailable biomarkers should be limited. The selected population should be diverse and representative of the population that the matter in question affects. Importantly, populations who experience inequities should be appropriately included through a range of strategies, including engaging with representatives from priority populations.</p><p>Interventions should be delivered in ways similar to current or future use in routine clinical practice. If interventions are designed to align with routine clinical practice, an intervention will likely be easier to embed and adopted more quickly. If an intervention has efficacy in a trial that has considered implementability, it is likely to be broadly effective when implemented into practice. For example, trialists should optimise opportunities for clinical staff (and not researchers) to deliver interventions. As reach and penetration are key to broader effectiveness, trials that can only recruit a small proportion of a target population are not recommended. Comparators, or the current standard of care (ie, an active control) where the investigator treats control participants as they would normally, should be included in trial protocols, as this offers the opportunity to provide a definitive end of trial recommendation.</p><p>End user consultation and strategies, such as run-in periods, can assess challenges in adherence with the intervention. Protocols should include adjustments or titration that may be necessary to achieve efficacy or avoid adverse events and these should align with application in routine care. Ultimately, including diverse end users can inform embedding and pragmatic aspects related to implementability.</p><p>Other design considerations are concomitant care; strategies to increase reach (such as limited exclusion and inclusion criteria); analysis (intention-to-treat principles are recommended<span><sup>12</sup></span>); limiting trial burden to optimise and sustain participation (eg, by considering type of consent, requirements of participant follow-up, and use of streamlined case report forms); embedding trials in a registry;<span><sup>13</sup></span> considering and capturing factors that influence reach, adoption, fidelity, maintenance and process evaluation;<span><sup>14</sup></span> and inclusion of health economic end points. A well designed, prospective health economic analysis may be critical to optimise implementation and will inform decision makers regarding investment.<span><sup>15-17</sup></span> Economic analysis should also focus on cost-effectiveness of interventions across different modelled scenarios, such as for specific population subgroups. This allows for the consideration of equity and provides policy makers with more nuanced investment options than simply offering “all or nothing” choices.</p><p>Historically, a large proportion of studies go unpublished, or reporting lacks sufficient detail.<span><sup>18</sup></span> This selective reporting increases the risk of publication bias and must be rectified. All trials must be reported in a timely manner, preferably within 12 months of their completion, and those reports must be readily accessible.<span><sup>19</sup></span> This is vital if the trial has insufficient recruitment or is unable to deliver the intervention as it will still generate new knowledge on process, challenges and implementability, relevant to the trial and to implementation into practice. Detailed reporting on factors that affect implementation is important and consideration of an implementation protocol can optimise generated data and assist end users with implementing trial findings into practice. Interventions should be described in detail to enable replication, using tools such as the Template for Intervention Description and Replication (TIDieR) checklist.<span><sup>20</sup></span> If the comparator was protocolised, details of the comparator and delivery methods should be clear. Open access publication should be prioritised to optimise reach to end users. Affordable open access options are needed to ensure equity and access.<span><sup>21</sup></span> Additional dissemination tools, channels and strategies (such as implementation guides, evidence synthesis, guidelines, policy summaries, round tables, health professional and consumer tools) are key to implementation and should be co-designed with end users. Authors should declare and maintain a record of real or perceived conflicts of interest and provide access to data where possible.</p><p>Many, but not all, clinical trials are completed by a network, with most members holding dual roles as researchers and clinicians. Many networks also include consumers, representative of end users. Consumer and community involvement (CCI) is fundamental, recommended or required by funders and considered good practice. This can include both formal or informal processes, across planning, design, conduct and reporting of trials. Early and embedded CCI in a structured, meaningful way within the network also enables appropriate implementation of trial outcomes. Networks can support quality CCI, as consumer engagement from the outset is prioritised by the NHMRC CCI statement. Tokenistic engagement with consumers should be avoided. ACTA, NHMRC and RTCs provide tools and resources to build capacity and support genuine CCI.<span><sup>22-24</sup></span></p><p>Networks can provide access to representative trial sites aligned to clinical sites and populations where results are applicable. Some networks, potentially with an associated registry, are ideally positioned to monitor implementation (Box). Lastly, networks can facilitate the next steps in dedicated implementation research involving the systematic study of methods, strategies and pathways that support the application of trial findings into policy and practice. It is acknowledged that implementation science requires different but overlapping skills and expertise to that of clinical trials and that capacity building is warranted in both implementability and implementation science.</p><p>To deliver on the investment and potential benefit of late-phase clinical trials, it is important that end user-informed implementability considerations are widely adopted and applied. Further information on best practice for the design, conduct and reporting of studies with a view to implementation can be found on ACTA's website (www.clinicaltrialsalliance.org.au/resource/6258/).</p><p>Open access publishing facilitated by Monash University, as part of the Wiley - Monash University agreement via the Council of Australian University Librarians.</p><p>Samantha Keogh reports monies received by her employer Queensland University of Technology from BD Medical and ITL Biomedical for educational consultancies not related to this study. Paul Cohen reports speaker's honoraria from Seqirus and AstraZeneca, stock and advisory board participation in Clinic IQ. David Johnson has received consultancy fees, research grants, speaker's honoraria and travel sponsorships from Baxter Healthcare and Fresenius Medical Care, consultancy fees from Astra Zeneca, Bayer, and AWAK, speaker's honoraria from ONO and Boehringer Ingelheim and Lilly, and travel sponsorships from ONO and Amgen. All other authors declare no relevant disclosures.</p><p>Not commissioned; externally peer reviewed.</p>","PeriodicalId":18214,"journal":{"name":"Medical Journal of Australia","volume":"221 8","pages":"410-413"},"PeriodicalIF":8.5000,"publicationDate":"2024-09-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.5694/mja2.52444","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medical Journal of Australia","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.5694/mja2.52444","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
The Australian Clinical Trials Alliance (ACTA) impact and implementation reference group has published guidance on clinical trial planning, design, conduct and reporting, to optimise the impact of late-phase trials.1 It is critical that clinical trials are designed, executed and reported on so that the generated evidence can be implemented and applied to improve practice, health systems and policy (defined as implementability).1 This is particularly important for late-phase trials as results from these trials guide stakeholder decisions on adoption or removal of candidate interventions from practice and policy. The results can also be used to guide implementation, potentially supplemented by other study types. In some cases, decisions on candidate interventions may be based on a single trial, although more commonly, they are based on the synthesis of evidence from multiple trials. If the results of positive late-phase trials are not put into effect, the community benefit, impact and return on investment are lost. Therefore, to reduce wastage and optimise value to the community, who is both the funder and beneficiary of research, we need to maximise the impact of trials. This impact includes health and economic benefits and requires trials to be designed for implementability.2-4
Implementability is key to trial design and delivery, independent of the results of the trial. Impact is dependent on intervention efficacy and implementability. Late-phase trials should incorporate implementability and be designed to be useful to their diverse end users (including organisations, governments, clinicians and consumers).
Characteristics that contribute to implementability include concepts around trials that are embedded in clinical care and are pragmatic, focused on informing clinical practice and policy and considering real-world investigators, recruitment, participants, intervention, delivery and outcomes. The PRECIS-2 framework (PRagmatic Explanatory Continuum Indicator Summary framework) indicates where a trial sits on the spectrum between the explanatory “Can this intervention work under ideal conditions?” to the pragmatic “Does this intervention work under usual conditions?”. This framework highlights the vital need to identify, involve and co-design or tailor trial design to the needs of end users.5 The Consolidated Framework for Implementation Research (CFIR) and similar tools are also useful to guide design and evaluation of implementation research.6, 7 In implementability, key trial design considerations include eligibility and exclusion criteria, setting, requirement for a skilled workforce or specialised equipment and extent of data collection. Similarly, trial design contributes to both embedding and implementability; with the need to recognise potential differences between strategies to promote trial efficiency, and those to promote implementability of trial findings.
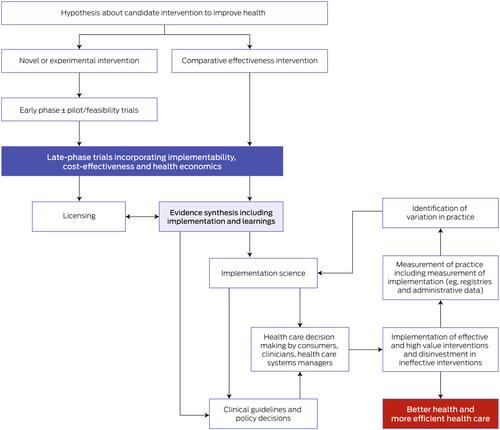
The important steps for progressing interventions through to implementation into practice, health services and policy are shown in the Box.
These steps align with the Australian Academy of Health and Medical Sciences report8 emphasising the importance of embedding research into health care, and the vital role of workforce and infrastructure in achieving this vision. The report also highlights the important role of National Health and Medical Research Council accredited research translation centres (RTCs) in implementation. The RTCs encompass most research, education and hospital services nationally and are well positioned to support clinical trial networks and enable implementation.9
Trials should be co-designed with end users, including consumers, who have experience and understanding of current practice.10 It is acknowledged that in some circumstances opportunities for co-design may be limited, such as in industry-sponsored trials. Pre-trial work with end users can establish relevance and the priority of research questions and appropriate outcome measures. Formal processes can be useful11 such as Delphi and nominal group techniques, although these need to be appropriate to the local context.
End points must be carefully chosen, including those of value to end users, and the minimum clinically important differences in end points considered. In addition, the minimum public health significant difference, which defines the relationship between a meaningful effect size and the public health disease burden, should be taken into account. For example, a major effect size (such as a cure for an inborn error of metabolism) in a rare disease may be just as important as minor effect sizes in common diseases (as this might cure a baby at birth and avoid lifetime costs and gain a lifetime of productivity).
The feasibility of intervention delivery should be established before a late-phase trial. This can be assessed via a systematic review of existing evidence (which may establish the merit for implementation of a particular approach to treating a health problem), as well as pilot studies. Regulatory approvals or burden should also be considered for implementation of drug or device interventions, alongside required skills and resources.
To optimise generalisability, consideration should be given to the population to which the results of the trial apply. The selected population should be as broad as possible, and entry criteria should be easily interpreted, using easily accessible information available to clinicians in routine practice, and participants in community-based trials. If the candidate intervention is targeted to a clinical setting, trial sites should be broadly representative of the centres that provide care to the key population groups in which the intervention would be implemented post-trial. For population-based studies, community-based recruitment and decentralised trial designs should be considered. If implementation will be beyond tertiary or quaternary hospitals, then the trial should be conducted to include this setting.
Inclusion criteria should be broad and exclusion criteria as limited as possible. Research burden and complexity from additional factors such as research-only or largely unavailable biomarkers should be limited. The selected population should be diverse and representative of the population that the matter in question affects. Importantly, populations who experience inequities should be appropriately included through a range of strategies, including engaging with representatives from priority populations.
Interventions should be delivered in ways similar to current or future use in routine clinical practice. If interventions are designed to align with routine clinical practice, an intervention will likely be easier to embed and adopted more quickly. If an intervention has efficacy in a trial that has considered implementability, it is likely to be broadly effective when implemented into practice. For example, trialists should optimise opportunities for clinical staff (and not researchers) to deliver interventions. As reach and penetration are key to broader effectiveness, trials that can only recruit a small proportion of a target population are not recommended. Comparators, or the current standard of care (ie, an active control) where the investigator treats control participants as they would normally, should be included in trial protocols, as this offers the opportunity to provide a definitive end of trial recommendation.
End user consultation and strategies, such as run-in periods, can assess challenges in adherence with the intervention. Protocols should include adjustments or titration that may be necessary to achieve efficacy or avoid adverse events and these should align with application in routine care. Ultimately, including diverse end users can inform embedding and pragmatic aspects related to implementability.
Other design considerations are concomitant care; strategies to increase reach (such as limited exclusion and inclusion criteria); analysis (intention-to-treat principles are recommended12); limiting trial burden to optimise and sustain participation (eg, by considering type of consent, requirements of participant follow-up, and use of streamlined case report forms); embedding trials in a registry;13 considering and capturing factors that influence reach, adoption, fidelity, maintenance and process evaluation;14 and inclusion of health economic end points. A well designed, prospective health economic analysis may be critical to optimise implementation and will inform decision makers regarding investment.15-17 Economic analysis should also focus on cost-effectiveness of interventions across different modelled scenarios, such as for specific population subgroups. This allows for the consideration of equity and provides policy makers with more nuanced investment options than simply offering “all or nothing” choices.
Historically, a large proportion of studies go unpublished, or reporting lacks sufficient detail.18 This selective reporting increases the risk of publication bias and must be rectified. All trials must be reported in a timely manner, preferably within 12 months of their completion, and those reports must be readily accessible.19 This is vital if the trial has insufficient recruitment or is unable to deliver the intervention as it will still generate new knowledge on process, challenges and implementability, relevant to the trial and to implementation into practice. Detailed reporting on factors that affect implementation is important and consideration of an implementation protocol can optimise generated data and assist end users with implementing trial findings into practice. Interventions should be described in detail to enable replication, using tools such as the Template for Intervention Description and Replication (TIDieR) checklist.20 If the comparator was protocolised, details of the comparator and delivery methods should be clear. Open access publication should be prioritised to optimise reach to end users. Affordable open access options are needed to ensure equity and access.21 Additional dissemination tools, channels and strategies (such as implementation guides, evidence synthesis, guidelines, policy summaries, round tables, health professional and consumer tools) are key to implementation and should be co-designed with end users. Authors should declare and maintain a record of real or perceived conflicts of interest and provide access to data where possible.
Many, but not all, clinical trials are completed by a network, with most members holding dual roles as researchers and clinicians. Many networks also include consumers, representative of end users. Consumer and community involvement (CCI) is fundamental, recommended or required by funders and considered good practice. This can include both formal or informal processes, across planning, design, conduct and reporting of trials. Early and embedded CCI in a structured, meaningful way within the network also enables appropriate implementation of trial outcomes. Networks can support quality CCI, as consumer engagement from the outset is prioritised by the NHMRC CCI statement. Tokenistic engagement with consumers should be avoided. ACTA, NHMRC and RTCs provide tools and resources to build capacity and support genuine CCI.22-24
Networks can provide access to representative trial sites aligned to clinical sites and populations where results are applicable. Some networks, potentially with an associated registry, are ideally positioned to monitor implementation (Box). Lastly, networks can facilitate the next steps in dedicated implementation research involving the systematic study of methods, strategies and pathways that support the application of trial findings into policy and practice. It is acknowledged that implementation science requires different but overlapping skills and expertise to that of clinical trials and that capacity building is warranted in both implementability and implementation science.
To deliver on the investment and potential benefit of late-phase clinical trials, it is important that end user-informed implementability considerations are widely adopted and applied. Further information on best practice for the design, conduct and reporting of studies with a view to implementation can be found on ACTA's website (www.clinicaltrialsalliance.org.au/resource/6258/).
Open access publishing facilitated by Monash University, as part of the Wiley - Monash University agreement via the Council of Australian University Librarians.
Samantha Keogh reports monies received by her employer Queensland University of Technology from BD Medical and ITL Biomedical for educational consultancies not related to this study. Paul Cohen reports speaker's honoraria from Seqirus and AstraZeneca, stock and advisory board participation in Clinic IQ. David Johnson has received consultancy fees, research grants, speaker's honoraria and travel sponsorships from Baxter Healthcare and Fresenius Medical Care, consultancy fees from Astra Zeneca, Bayer, and AWAK, speaker's honoraria from ONO and Boehringer Ingelheim and Lilly, and travel sponsorships from ONO and Amgen. All other authors declare no relevant disclosures.
这可以通过对现有证据的系统审查(这可能会确定实施特定方法治疗健康问题的价值)以及试点研究进行评估。在实施药物或器械干预时,还应考虑监管部门的批准或负担,以及所需的技能和资源。所选人群应尽可能广泛,入选标准应易于解释,使用日常实践中临床医生和社区试验参与者容易获得的信息。如果候选干预措施针对的是临床环境,试验地点应广泛代表为关键人群提供医疗服务的中心,干预措施将在试验后在这些中心实施。对于以人群为基础的研究,应考虑以社区为基础的招募和分散试验设计。如果实施范围超出三级或四级医院,则试验应包括这一环境。应限制仅用于研究或基本不可用的生物标记物等额外因素造成的研究负担和复杂性。所选人群应具有多样性,并能代表相关问题所影响的人群。重要的是,应通过一系列策略(包括与重点人群的代表接触)适当纳入遭受不公平待遇的人群。如果干预措施的设计与常规临床实践相一致,那么干预措施可能会更容易嵌入和更快被采用。如果一项干预措施在考虑了可实施性的试验中取得了疗效,那么在实践中实施时很可能会取得广泛的疗效。例如,试验人员应优化临床人员(而非研究人员)实施干预的机会。由于覆盖率和渗透率是取得广泛疗效的关键,因此不建议开展只能招募到一小部分目标人群的试验。试验方案中应包括对照组或目前的护理标准(即积极对照组),研究者对对照组参与者进行正常治疗,因为这为提供明确的试验结束建议提供了机会。试验方案应包括为达到疗效或避免不良事件而可能需要的调整或滴定,这些调整或滴定应与常规护理中的应用相一致。最终,让不同的最终用户参与进来可以为可实施性相关的嵌入和实用方面提供信息。其他设计考虑因素包括:伴随护理;扩大覆盖范围的策略(如有限的排除和纳入标准);分析(建议采用意向治疗原则12);限制试验负担以优化和维持参与(如考虑同意类型、参与者随访要求和使用简化的病例报告表);将试验嵌入登记册;13 考虑并捕捉影响覆盖范围、采用、忠诚度、维持和过程评估的因素;14 以及纳入卫生经济学终点。精心设计的前瞻性卫生经济分析可能是优化实施的关键,并将为决策者提供有关投资的信息15-17。经济分析还应关注不同模型情景下干预措施的成本效益,如针对特定人口亚群。与简单地提供 "要么全有,要么全无 "的选择相比,这样可以考虑公平性,并为决策者提供更细致的投资选择。所有试验都必须及时报告,最好是在试验完成后 12 个月内报告,而且这些报告必须易于获取。19 如果试验招募人数不足或无法实施干预措施,这一点至关重要,因为它仍会产生与试验和实践实施相关的过程、挑战和可实施性方面的新知识。详细报告影响实施的因素非常重要,考虑实施方案可以优化生成的数据,并帮助最终用户将试验结果应用到实践中。应使用干预措施描述与复制模板(TIDieR)清单等工具对干预措施进行详细描述,以便于复制。 20 如果比较对象是协议化的,则应清楚说明比较对象的细节和提供方法。应优先考虑公开获取出版物,以优化最终用户的接触。21 额外的传播工具、渠道和策略(如实施指南、证据综述、指南、政策摘要、圆桌会议、卫生专业人员和消费者工具)是实施的关键,应与最终用户共同设计。作者应声明并记录真实或感知的利益冲突,并在可能的情况下提供数据访问权限。许多临床试验由网络完成,但并非所有临床试验都是由网络完成的,大多数成员具有研究人员和临床医生的双重身份。许多网络还包括代表最终用户的消费者。消费者和社区参与(CCI)是资助者推荐或要求的基本做法,也被认为是良好实践。消费者和社区参与(CCI)是最基本的,是资助者推荐或要求的,也被认为是一种良好的做法。这可能包括正式或非正式的过程,涉及试验的规划、设计、实施和报告。在网络内以有组织、有意义的方式及早开展和巩固 CCI,也有助于适当落实试验成果。NHMRC CCI声明将消费者从一开始的参与列为优先事项,因此网络可以支持高质量的CCI。应避免只是象征性地让消费者参与。ACTA、NHMRC和RTC为能力建设和支持真正的CCI提供了工具和资源。22-24网络可提供与临床地点和结果适用人群相一致的代表性试验地点。一些网络(可能有相关的登记处)是监测实施情况的理想场所(方框)。最后,网络可以促进专门实施研究的下一步工作,包括系统研究方法、策略和途径,以支持将试验结果应用到政策和实践中。我们认识到,实施科学需要与临床试验不同但重叠的技能和专业知识,因此需要在可实施性和实施科学两方面进行能力建设。有关设计、开展和报告实施性研究的最佳实践的更多信息,请访问ACTA网站(www.clinicaltrialsalliance.org.au/resource/6258/)。莫纳什大学通过澳大利亚大学图书馆员理事会(Council of Australian University Librarians)促成了Wiley与莫纳什大学协议的一部分--开放存取出版。Samantha Keogh报告了其雇主昆士兰科技大学从BD Medical和ITL Biomedical获得的与本研究无关的教育咨询费。保罗-科恩(Paul Cohen)报告了从 Seqirus 公司和阿斯利康公司获得的演讲酬金,以及参与 Clinic IQ 公司股票和顾问委员会的情况。大卫-约翰逊(David Johnson)从百特医疗保健公司(Baxter Healthcare)和费森尤斯医疗保健公司(Fresenius Medical Care)获得顾问费、研究基金、演讲酬金和差旅赞助,从阿斯利康公司(Astra Zeneca)、拜耳公司(Bayer)和 AWAK 公司获得顾问费,从 ONO 公司、勃林格殷格翰公司(Boehringer Ingelheim)和礼来公司(Lilly)获得演讲酬金,从 ONO 公司和安进公司(Amgen)获得差旅赞助。所有其他作者声明没有相关披露。
期刊介绍:
The Medical Journal of Australia (MJA) stands as Australia's foremost general medical journal, leading the dissemination of high-quality research and commentary to shape health policy and influence medical practices within the country. Under the leadership of Professor Virginia Barbour, the expert editorial team at MJA is dedicated to providing authors with a constructive and collaborative peer-review and publication process. Established in 1914, the MJA has evolved into a modern journal that upholds its founding values, maintaining a commitment to supporting the medical profession by delivering high-quality and pertinent information essential to medical practice.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
