Adding Evidence to an Evidence-Based Classification for Recurrent Weight Gain after Bariatric and Metabolic Surgery from a Norwegian National Registry.
Rutger J Franken, Hannu S Lyyjynen, Simon W Nienhuijs, Villy Våge, Arnold W van de Laar
{"title":"Adding Evidence to an Evidence-Based Classification for Recurrent Weight Gain after Bariatric and Metabolic Surgery from a Norwegian National Registry.","authors":"Rutger J Franken, Hannu S Lyyjynen, Simon W Nienhuijs, Villy Våge, Arnold W van de Laar","doi":"10.1007/s11695-024-07476-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In 2023, the first evidence-based classification for recurrent weight gain (RWG) after metabolic and bariatric surgery was introduced. It uses early and late follow-up weight loss benchmarks based on standard deviations (SD) of percentage total weight loss(%TWL) results from the large Dutch Audit for Treatment of Obesity (DATO) registry (n > 18,000). We aimed to validate this classification and confirm its clinical relevance with an external cohort.</p><p><strong>Methods: </strong>The DATO-based classification defines all RWG as grade 1, as long as weight-loss does not drop below DATO's late-follow-up minus one SD benchmark (20%TWL). Grade 3 represents clear outliers whose RWG evolves below DATO's late follow-up minus two SD benchmark (10%TWL), with grade 2 in-between. Grades 2a/3a represent initial suboptimal clinical response, with nadir %TWL never exceeding DATO's early-follow-up minus one SD benchmark (25%TWL). Grades 2b/3b represent late clinical deterioration from nadir weight loss ≥ 25%TWL. We compared baseline characteristics, SD based benchmarks, RWG and comorbidities from the Scandinavian Obesity Surgery Registry Norway (SOReg-N) with these DATO-derived grades.</p><p><strong>Results: </strong>The SOReg-N population (n = 3064) was comparable at baseline, with more sleeve gastrectomies (54% versus DATO 22.5%). The SD benchmarks were at early follow-up minus one SD 25.8%TWL, at 5 years minus one SD/minus two-SD 17.2%TWL/7.0%TWL (DATO 25%TWL/20%TWL/10%TWL). Percentage of patients and amount of RWG were similar to DATO. In line with DATO, comorbidities were predominant in grades 2a/3a, with least improvement in grade 3a. Also, grade 3b showed more favorable characteristics at baseline.</p><p><strong>Conclusion: </strong>The SOReg-N cohort confirmed the weight-loss benchmarks defining the DATO-derived grades, the distribution of patients and their RWG across the grades, and correlations between grades and comorbidities. Male gender, older age and comorbidities were predominant among patients with initial suboptimal clinical response (RWG grades 2a/3a), but not for late clinical deterioration (RWG grades 2b/3b). This classification can be used for populations with diverse weight loss trajectories and offers an evidence-based guide for clinical decision-making and standardization.</p>","PeriodicalId":19460,"journal":{"name":"Obesity Surgery","volume":" ","pages":"3833-3839"},"PeriodicalIF":3.1000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Obesity Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s11695-024-07476-y","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/9 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: In 2023, the first evidence-based classification for recurrent weight gain (RWG) after metabolic and bariatric surgery was introduced. It uses early and late follow-up weight loss benchmarks based on standard deviations (SD) of percentage total weight loss(%TWL) results from the large Dutch Audit for Treatment of Obesity (DATO) registry (n > 18,000). We aimed to validate this classification and confirm its clinical relevance with an external cohort.
Methods: The DATO-based classification defines all RWG as grade 1, as long as weight-loss does not drop below DATO's late-follow-up minus one SD benchmark (20%TWL). Grade 3 represents clear outliers whose RWG evolves below DATO's late follow-up minus two SD benchmark (10%TWL), with grade 2 in-between. Grades 2a/3a represent initial suboptimal clinical response, with nadir %TWL never exceeding DATO's early-follow-up minus one SD benchmark (25%TWL). Grades 2b/3b represent late clinical deterioration from nadir weight loss ≥ 25%TWL. We compared baseline characteristics, SD based benchmarks, RWG and comorbidities from the Scandinavian Obesity Surgery Registry Norway (SOReg-N) with these DATO-derived grades.
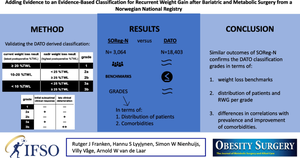
Results: The SOReg-N population (n = 3064) was comparable at baseline, with more sleeve gastrectomies (54% versus DATO 22.5%). The SD benchmarks were at early follow-up minus one SD 25.8%TWL, at 5 years minus one SD/minus two-SD 17.2%TWL/7.0%TWL (DATO 25%TWL/20%TWL/10%TWL). Percentage of patients and amount of RWG were similar to DATO. In line with DATO, comorbidities were predominant in grades 2a/3a, with least improvement in grade 3a. Also, grade 3b showed more favorable characteristics at baseline.
Conclusion: The SOReg-N cohort confirmed the weight-loss benchmarks defining the DATO-derived grades, the distribution of patients and their RWG across the grades, and correlations between grades and comorbidities. Male gender, older age and comorbidities were predominant among patients with initial suboptimal clinical response (RWG grades 2a/3a), but not for late clinical deterioration (RWG grades 2b/3b). This classification can be used for populations with diverse weight loss trajectories and offers an evidence-based guide for clinical decision-making and standardization.
期刊介绍:
Obesity Surgery is the official journal of the International Federation for the Surgery of Obesity and metabolic disorders (IFSO). A journal for bariatric/metabolic surgeons, Obesity Surgery provides an international, interdisciplinary forum for communicating the latest research, surgical and laparoscopic techniques, for treatment of massive obesity and metabolic disorders. Topics covered include original research, clinical reports, current status, guidelines, historical notes, invited commentaries, letters to the editor, medicolegal issues, meeting abstracts, modern surgery/technical innovations, new concepts, reviews, scholarly presentations and opinions.
Obesity Surgery benefits surgeons performing obesity/metabolic surgery, general surgeons and surgical residents, endoscopists, anesthetists, support staff, nurses, dietitians, psychiatrists, psychologists, plastic surgeons, internists including endocrinologists and diabetologists, nutritional scientists, and those dealing with eating disorders.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
