Patricia Gina Lu, Zhi Ven Fong, Patrick T Hangge, Yu-Hui Chang, Elisabeth S Lim, Nabil Wasif, Patricia A Cronin, Chee-Chee Stucky
{"title":"Differential utilization of thyroid lobectomy after the 2015 American Thyroid Association guideline update.","authors":"Patricia Gina Lu, Zhi Ven Fong, Patrick T Hangge, Yu-Hui Chang, Elisabeth S Lim, Nabil Wasif, Patricia A Cronin, Chee-Chee Stucky","doi":"10.1530/EO-24-0010","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The 2015 American Thyroid Association (ATA) guidelines added thyroid lobectomy (TL) as the appropriate treatment for low-risk differentiated thyroid cancer (DTC). We aimed to investigate the population-level factors that influence the utilization of TL.</p><p><strong>Methods: </strong>The Surveillance, Epidemiology and End Results (SEER) database was queried for all DTC patients fitting low-risk criteria as defined by the ATA. Trends in total thyroidectomy (TT) and TL were identified using a Cochrane-Armitage test. Multivariable logistic regression identified patient and socioeconomic characteristics associated with TL, and difference-in-difference analysis was used to control for secular trends over time.</p><p><strong>Results: </strong>A total of 43,526 patients with low-risk DTC were identified in the SEER database; 39,411 pre-2015 and 4115 post-2015. After 2015, TT continued to outnumber TL (76.2% vs 23.8%), although the rate of TL increased significantly (11.6% to 23.8%, <i>P</i> < 0.001). However, difference-in-difference analysis found that age > 55 (OR 1.11, 95% CI 1.01-1.19, <i>P</i> < 0.001) and rurality (OR 1.16, 95% CI 1.05-1.28, <i>P</i> < 0.001) were independently associated with TT. TL was associated with T1 disease (OR 1.11, 95% CI 1.04-1.19, <i>P</i> = 0.001).</p><p><strong>Conclusion: </strong>Although the 2015 ATA guideline update led to an increase in TL for low-risk DTC, most patients still underwent TT. Age and neighborhood significantly impact the odds of receiving guideline-appropriate TL for low-risk DTC, especially for T2 disease.</p>","PeriodicalId":72907,"journal":{"name":"Endocrine oncology (Bristol, England)","volume":"4 1","pages":"e240010"},"PeriodicalIF":0.0000,"publicationDate":"2024-09-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11378144/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Endocrine oncology (Bristol, England)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1530/EO-24-0010","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The 2015 American Thyroid Association (ATA) guidelines added thyroid lobectomy (TL) as the appropriate treatment for low-risk differentiated thyroid cancer (DTC). We aimed to investigate the population-level factors that influence the utilization of TL.
Methods: The Surveillance, Epidemiology and End Results (SEER) database was queried for all DTC patients fitting low-risk criteria as defined by the ATA. Trends in total thyroidectomy (TT) and TL were identified using a Cochrane-Armitage test. Multivariable logistic regression identified patient and socioeconomic characteristics associated with TL, and difference-in-difference analysis was used to control for secular trends over time.
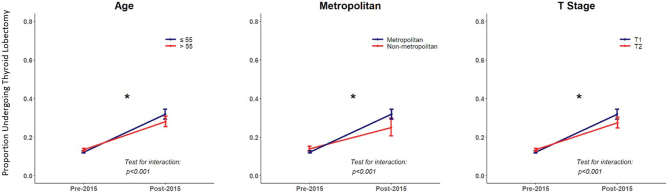
Results: A total of 43,526 patients with low-risk DTC were identified in the SEER database; 39,411 pre-2015 and 4115 post-2015. After 2015, TT continued to outnumber TL (76.2% vs 23.8%), although the rate of TL increased significantly (11.6% to 23.8%, P < 0.001). However, difference-in-difference analysis found that age > 55 (OR 1.11, 95% CI 1.01-1.19, P < 0.001) and rurality (OR 1.16, 95% CI 1.05-1.28, P < 0.001) were independently associated with TT. TL was associated with T1 disease (OR 1.11, 95% CI 1.04-1.19, P = 0.001).
Conclusion: Although the 2015 ATA guideline update led to an increase in TL for low-risk DTC, most patients still underwent TT. Age and neighborhood significantly impact the odds of receiving guideline-appropriate TL for low-risk DTC, especially for T2 disease.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
