Blood pressure (BP) measured by 24-h ambulatory blood pressure monitoring (ABPM) is a better predictor of hypertension (HTN)-related end-organ damage than office BP; however, it is not always available nor tolerated by patients. Community pharmacy-measured blood pressure (CPBP) could serve as a potential alternative, although it is unknown whether CPBP is equivalent to BP measured using ABPM.
The primary objective of this pilot study was to explore the equivalency of CPBP compared with awake ABPM.
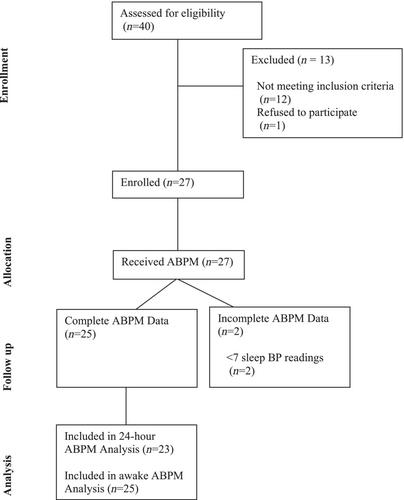
This was a pilot, single-arm, equivalency study of adults ≥21 years with HTN, taking ≥1 antihypertensive with no changes in the prior 2 weeks. Exclusion criteria included night shift workers, sleep apnoea, arrhythmia, on dialysis, pregnancy or an arm circumference > 50 cm. Three unattended seated BP measurements were obtained in both arms at a community pharmacy and followed by 24-h ABPM. At the return visit, seated BP measurements were repeated; the mean across both visits served as the CPBP. The primary outcome was the equivalency of systolic BP measured at the community pharmacy to awake BP measured using ABPM. The continuous outcome (BP) was modelled against a binary fixed effect for the measurement device (CPBP vs. ABPM) and a subject-level random effect to account for the multiple BP readings arising from the same individuals.
The 25 participants had a mean (standard deviation [SD]) age of 65 (15) years, 80% were female, and 36% identified as Black or Latino. The mean (SD) systolic BP was 128.0 (20.2) and 129.1 (15.8) mmHg for CPBP and awake ABPM, respectively (p = 0.8409). No significant differences were found between the mean diastolic BP or heart rate for CPBP vs. 24-h ABPM or CPBP vs. daytime ABPM.
The difference between CPBP and ABPM was not statistically significant; however, we cannot claim equivalence between the two approaches.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
