Neoadjuvant gemcitabine–cisplatin plus tislelizumab in persons with resectable muscle-invasive bladder cancer: a multicenter, single-arm, phase 2 trial
Kaiwen Li, Wenlong Zhong, Jinhai Fan, Shaogang Wang, Dexin Yu, Tao Xu, Jiaju Lyu, Shaoxu Wu, Tao Qin, Zhuo Wu, Longhao Xu, Kaijie Wu, Zheng Liu, Zhiquan Hu, Fan Li, Jinyou Wang, Qi Wang, Jie Min, Zhiqiang Zhang, Luping Yu, Sentai Ding, Longfei Huang, Tingting Zhao, Jian Huang, Tianxin Lin
{"title":"Neoadjuvant gemcitabine–cisplatin plus tislelizumab in persons with resectable muscle-invasive bladder cancer: a multicenter, single-arm, phase 2 trial","authors":"Kaiwen Li, Wenlong Zhong, Jinhai Fan, Shaogang Wang, Dexin Yu, Tao Xu, Jiaju Lyu, Shaoxu Wu, Tao Qin, Zhuo Wu, Longhao Xu, Kaijie Wu, Zheng Liu, Zhiquan Hu, Fan Li, Jinyou Wang, Qi Wang, Jie Min, Zhiqiang Zhang, Luping Yu, Sentai Ding, Longfei Huang, Tingting Zhao, Jian Huang, Tianxin Lin","doi":"10.1038/s43018-024-00822-0","DOIUrl":null,"url":null,"abstract":"Programmed death 1 blockade (tislelizumab) has been approved for metastatic urothelial carcinoma but not as part of neoadjuvant therapy for muscle-invasive bladder cancer (MIBC). In this multicenter single-arm trial (ChiCTR2000037670), 65 participants with cT2-4aN0M0 MIBC received neoadjuvant gemcitabine–cisplatin plus tislelizumab; 57 of them underwent radical cystectomy (RC). The primary endpoint of pathologic complete response (pCR) rate was 50.9% (29/57, 95% confidence interval (CI) 37.3–64.4%) and the pathologic downstaging (secondary endpoint) rate was 75.4% (43/57, 95% CI 62.2–85.9%) in participants undergoing RC. Genomic and transcriptomic analyses revealed three MIBC molecular subtypes (S): S1 (immune-desert) with activated cell-cycle pathway, S2 (immune-excluded) with activated transforming growth factor-β pathway and S3 (immune-inflamed) with upregulated interferon-α and interferon-γ response. Post hoc analysis showed pCR rates of 16% (3/19, S1), 77% (10/13, S2) and 80% (12/15, S3) (P = 0.006). In conclusion, neoadjuvant gemcitabine–cisplatin plus tislelizumab for MIBC was compatible with an enhanced pCR rate. Li et al. perform a phase 2 single-arm clinical trial of neoadjuvant chemotherapy plus checkpoint blockade in participants with resectable muscle-invasive bladder cancer and conduct genomic and transcriptomic profiling to describe molecular subtypes.","PeriodicalId":18885,"journal":{"name":"Nature cancer","volume":"5 10","pages":"1465-1478"},"PeriodicalIF":28.5000,"publicationDate":"2024-09-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Nature cancer","FirstCategoryId":"3","ListUrlMain":"https://www.nature.com/articles/s43018-024-00822-0","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
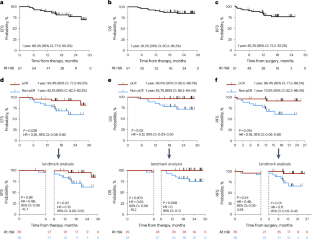
Programmed death 1 blockade (tislelizumab) has been approved for metastatic urothelial carcinoma but not as part of neoadjuvant therapy for muscle-invasive bladder cancer (MIBC). In this multicenter single-arm trial (ChiCTR2000037670), 65 participants with cT2-4aN0M0 MIBC received neoadjuvant gemcitabine–cisplatin plus tislelizumab; 57 of them underwent radical cystectomy (RC). The primary endpoint of pathologic complete response (pCR) rate was 50.9% (29/57, 95% confidence interval (CI) 37.3–64.4%) and the pathologic downstaging (secondary endpoint) rate was 75.4% (43/57, 95% CI 62.2–85.9%) in participants undergoing RC. Genomic and transcriptomic analyses revealed three MIBC molecular subtypes (S): S1 (immune-desert) with activated cell-cycle pathway, S2 (immune-excluded) with activated transforming growth factor-β pathway and S3 (immune-inflamed) with upregulated interferon-α and interferon-γ response. Post hoc analysis showed pCR rates of 16% (3/19, S1), 77% (10/13, S2) and 80% (12/15, S3) (P = 0.006). In conclusion, neoadjuvant gemcitabine–cisplatin plus tislelizumab for MIBC was compatible with an enhanced pCR rate. Li et al. perform a phase 2 single-arm clinical trial of neoadjuvant chemotherapy plus checkpoint blockade in participants with resectable muscle-invasive bladder cancer and conduct genomic and transcriptomic profiling to describe molecular subtypes.
期刊介绍:
Cancer is a devastating disease responsible for millions of deaths worldwide. However, many of these deaths could be prevented with improved prevention and treatment strategies. To achieve this, it is crucial to focus on accurate diagnosis, effective treatment methods, and understanding the socioeconomic factors that influence cancer rates.
Nature Cancer aims to serve as a unique platform for sharing the latest advancements in cancer research across various scientific fields, encompassing life sciences, physical sciences, applied sciences, and social sciences. The journal is particularly interested in fundamental research that enhances our understanding of tumor development and progression, as well as research that translates this knowledge into clinical applications through innovative diagnostic and therapeutic approaches. Additionally, Nature Cancer welcomes clinical studies that inform cancer diagnosis, treatment, and prevention, along with contributions exploring the societal impact of cancer on a global scale.
In addition to publishing original research, Nature Cancer will feature Comments, Reviews, News & Views, Features, and Correspondence that hold significant value for the diverse field of cancer research.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
