{"title":"Routine GI Endoscopy","authors":"","doi":"10.1111/jgh.16708","DOIUrl":null,"url":null,"abstract":"<p><b>8</b></p><p><b>A rare lesion of the oesophagus: oesophageal submucosal gland duct adenoma</b></p><p><b>Gary Zhang</b><sup>1,2</sup>, Spiro Raftopoulos<sup>1,2,3</sup> and Priyanthi Kumarasinghe<sup>1,2,3</sup></p><p><sup>1</sup><i>Sir Charles Gairdner Osborne Park Health Care Group, Perth, Australia;</i> <sup>2</sup><i>The University of Western Australia, Perth, Australia;</i> <sup>3</sup><i>Curtin University, Bentley, Australia</i></p><p><b><i>Introduction:</i></b> Oesophageal submucosal gland duct adenomas (ESGDA) are a rare oesophageal lesion usually diagnosed in males 50-80 years of age presenting with abdominal pain or incidentally. Less than 20 cases of ESGDA have been reported in the literature, with two cases reporting incidental accompanying oesophageal squamous cell carcinoma and gastric adenocarcinoma, respectively.</p><p><b><i>Case report:</i></b> A 68-year-old Caucasian man without other significant medical history presented with mild reflux symptoms. There were no associated alarm symptoms. He was a non-smoker and consumed up to 2 standard drinks of alcohol a day. Initial upper gastrointestinal endoscopy demonstrated a 10mm subepithelial lesion (SEL) at the gastroesophageal junction with normal overlying squamous mucosa and no evidence of reflux changes (figure 1). Pinch biopsies were acquired and reported as an inflammatory polyp with no evidence of dysplasia. The patient was referred for consideration of endoscopic removal following 8 weeks of high dose twice daily proton pump inhibitor therapy. On subsequent endoscopy, the SEL remained despite high dose PPI and therefore a decision was made for endoscopic removal via local excision using a band and ligation technique (figure 1A-C). The lesion was completely resected, retrieved, pinned and sent for pathological assessment. Histopathological assessment of the SEL demonstrated a predominantly submucosal lesion featuring localised hyperplastic and proliferated oesophageal glands and ducts without malignancy (figure 1D). With histochemical stains, the glandular epithelial cells showed diffuse cytoplasmic positivity with epithelial membrane antigen and CK7. Some basal cells showed a positive reaction with p63 and p40. There was no aberrant p53 over-expression or heightened ki-67 proliferation index. The lesion was consistent with an ESGDA. Endoscopic appearances at follow-up demonstrated a smooth, contracted scar (figure 1E).</p><p><b>17</b></p><p><b>Colonoscopy in octogenarians and older patients with 1L polyethylene glycol plus ascorbic acid bowel preparation in the real-world setting</b></p><p>Elena Perez-Arellano<sup>1</sup>, Salvador Machlab<sup>2</sup>, Miguel A Pantaleón<sup>3</sup>, Ricardo Gorjão<sup>4</sup>, Cátia Arieira<sup>5</sup>, Jose Cotter<sup>5</sup>, Vicente Lorenzo-Zúñiga<sup>6</sup>, Sarbelio Rodriguez Muñoz<sup>7</sup>, David Carral-Martínez<sup>8</sup>, Carmen Turbi<sup>9</sup>, Fatma Akriche<sup>10</sup>, José M Esteban<sup>11</sup> and <b>Katherine Davies</b><sup>12</sup></p><p><sup>1</sup><i>Hospital La Zarzuela, Madrid, Spain;</i> <sup>2</sup><i>Hospital Parc Taulí de Sabadell, Sabadell, Spain;</i> <sup>3</sup><i>Hospital del Mar, Barcelona, Spain;</i> <sup>4</sup><i>Hospital C UF Descobertas, Lisbon, Portugal;</i> <sup>5</sup><i>Hospital Senhora da Oliveira, Guimarães,, Portugal;</i> <sup>6</sup><i>Hospital HM Sant Jordi, Barcelona, Spain;</i> <sup>7</sup><i>Hospital Ruber Juan Bravo, Madrid, Spain;</i> <sup>8</sup><i>Hospital San Rafael, A Coruña, Spain;</i> <sup>9</sup><i>Norgine Medical Department, Spain;</i> <sup>10</sup><i>Norgine Medical Affairs, Harefield, United Kingdom;</i> <sup>11</sup><i>Hospital Clinico Universitario San Carlos, Madrid, Spain;</i> <sup>12</sup><i>Norgine, Sydney, Australia</i></p><p><b><i>Background and Aim:</i></b> Colonoscopy for colorectal cancer (CRC) detection in octogenarians is technically challenging due to bowel preparation difficulties in this population. While moderate or poor preparation quality were reported in 25% patients using large volume PEG [1], there is no published literature in octogenarians using validated cleansing scales. The aim of this study was to evaluate the colon cleansing effectiveness and safety of a contemporary bowel preparation, the 1L polyethylene glycol plus ascorbic acid (1L PEG+ASC) in octogenarians and older patients.</p><p><b><i>Methods:</i></b> Post-hoc analysis of an observational, multicentre, retrospective real-world study. Outpatients aged ≥ 80 years, who received 1L PEG + ASC before undergoing colonoscopy in 8 centres in Spain and Portugal between July 2019 and September 2021 [2]. Cleansing quality was evaluated using the Boston Bowel Preparation Scale (BBPS). Adequate quality was defined as a BBPS score ≥6 with all segmental scores ≥2. High-quality cleansing was defined overall as a BBPS score ≥8, and segmentally as a BBPS score of 3. Caecal intubation rate (CIR), withdrawal time (WT) and polyp detection rate (PDR) were also assessed. Safety was assessed from recorded adverse events (AEs).</p><p><b><i>Results:</i></b> A total of 423/13,169 patients (3.2%), 49.2% male were included. Mean age 83.5 years (range 80 to 95 years). Indication for colonoscopy was screening for CRC (14.4%), diagnostic (56.7%), follow-up (25.5%), or other (3.3%). The bowel preparation method was either as a split-dose (40.9%) or a same-day dose (59.1%) regimen. In total, 94.1% of patients completed the colonoscopy. Incomplete colonoscopy was reported in 5.9% of patients, including 1% due to poor preparation, 1.4% due to stenosing cancer, 1.2% due to technical difficulties, and 2.3% for other reasons. The CIR was 94.9%, the mean WT was 8.4 minutes, and the overall PDR was 45.6%. Cleansing outcomes are shown in Figure 1. The incidence of AEs was 4.5%, with dehydration (2.8%) and nausea (1.2%) being the most reported AEs. No severe AEs were reported.</p><p><b>References</b></p><p>\n 1. <span>Chatrenet, P</span>, <span>Friocourt, P</span>, <span>Ramain, JP</span>, et al. <span>Colonoscopy in the elderly: A study of 200 cases</span>. <i>Eur J Med</i> <span>1993</span>; <span>2</span>: <span>411</span>–<span>3</span>.</p><p>\n 2. <span>López-Jamar, JME</span>, et al. <span>Bowel cleansing effectiveness and safety of 1L PEG + Asc in the real-world setting: Observational, retrospective, multicenter study of over 13000 patients</span>. <i>Endosc Int Open</i> <span>2023</span>; <span>11</span>(<span>08</span>): <span>E785</span>-<span>E793</span>.</p><p><b>24</b></p><p><b>Endoscopists’ knowledge, perceptions and attitudes towards the use of artificial intelligence in endoscopy: A systematic review</b></p><p><b>Nicholas Wan</b><sup>1,2</sup>, Celine Chan<sup>1</sup>, Jin Lin Tan<sup>1,2</sup>, Mohamed Asif Chinnaratha<sup>1,2</sup> and Rajvinder Singh<sup>1,2</sup></p><p><sup>1</sup><i>Gastroenterology Department, Lyell McEwin Hospital, Adelaide, Australia;</i> <sup>2</sup><i>Adelaide Medical School, University of Adelaide, Adelaide, Australia</i></p><p><b><i>Background and Aim:</i></b> Artificial Intelligence (AI) is rapidly evolving in the field of gastrointestinal endoscopy. However, the prevailing perceptions and attitudes of endoscopists towards AI remain poorly understood. This review aims to provide a summary on the current views and perspectives covering the incorporation of AI into endoscopy, as well as to identify any obstacles hindering its adoption.</p><p><b><i>Methods:</i></b> Electronic databases including MEDLINE, PubMed, and Scopus were searched from inception to 25th March 2024 to identify qualitative studies, such as questionnaires or surveys, conducted on endoscopists regarding the use of AI in endoscopy. The Joanna Briggs Institute critical appraisal checklist was used to assess study quality. Qualitative synthesis of included studies was conducted by employing thematic analysis classified into the following five domains: 1) Knowledge, and attitudes towards AI, 2) Perception on AI’s ability to improve accuracy and quality of endoscopy, 3) Impact of AI on endoscopists, 4) Impact of AI on patients and 5) Barriers towards the implementation of AI.</p><p><b><i>Results:</i></b> Ten studies were included in this systematic review comprising of 1587 endoscopists across Europe (32.6%), North America (42.8%), and Asia (24.6%). Domain 1: Most endoscopists (69–100%) reported having basic knowledge of AI. Furthermore, the majority (79.5–87.5%) expressed interest and optimism regarding AI in endoscopy. Domain 2: Most respondents (62.5–97%) supported the notion that AI would positively impact endoscopic performance and quality. Domain 3: There were mixed perceptions regarding the extent of operator dependence on AI (6.2–62.8% agreement), and whether AI would prolong procedural time (21–81.3% in agreement). Most endoscopists (71–100%) disagreed that AI would replace them at work. Domain 4: A substantial proportion of respondents (81.3%) felt that AI would lead to an increase in the quality of patient care. Only a minority of endoscopists (6.2–24%) felt that AI could improve the patient-physician relationship and provide empathetic care. Domain 5: A significant proportion of endoscopists (75.2–91%) identified costs as potential barriers to the implementation of AI in endoscopy. Opinions on ethical concerns and the lack of regulation varied (12.5–100% and 35–88%, respectively), with many endoscopists feeling that there was need for clear guidelines and regulations when integrating AI into clinical practice.</p><p><b>31</b></p><p><b>Development of hepatic portal venous gas following percutaneous endoscopic gastrostomy – an ominous radiological sign?</b></p><p><b>Joel Thio</b></p><p><i>Department of Gastroenterology and Hepatology, Logan Hospital, Meadowbrook, Australia</i></p><p><b><i>Introduction:</i></b> Percutaneous endoscopic gastrostomy (PEG) feeding is widely used to overcome barriers to nutrition in patients with impaired swallowing. Like any intervention, this procedure carries risks of complications. Hepatic portal venous gas (HPVG), a rare radiological entity usually seen as an ominous sign, has only been reported in five case reports to date following PEG insertion. The aim of this case report is to raise awareness of this rare complication following PEG insertion.</p><p><b><i>Conclusion:</i></b> HPVG is a rare entity following PEG procedures, with only five case reports in the literature to date – two cases were managed conservatively with antibiotics with good outcomes, one case was managed conservatively without antibiotics with a good outcome, and two cases unfortunately died soon after from septic shock. If we include our case of death from likely intra-abdominal sepsis, this brings the mortality rate associated with findings of HPVG post-PEG insertion to 50%. This supports the increasing need for more data and vigilance of this radiological finding of HPVG following PEG procedures to help guide the course of care in these patients.</p><p><b>40</b></p><p><b>Over-the-scope clipping of a bleeding duodenal Dieulafoy lesion: a case report</b></p><p><b>Carl Cosgrave</b><sup>1</sup>, Zacchary Tamsett<sup>1,2</sup>, <b>Eliza Flanagan</b><sup>1,3</sup> and Neel Heerasing<sup>1,2</sup></p><p><sup>1</sup><i>Barwon Health, Geelong, Australia;</i> <sup>2</sup><i>Deakin University, Geelong, Australia;</i> <sup>3</sup><i>Monash University, Melbourne, Australia</i></p><p><b><i>Introduction:</i></b> Dieulafoy lesions (DL) are enlarged submucosal blood vessels that bleed in the absence of abnormality such as ulcers or erosions<sup>1</sup>. They are a rare cause for obscure upper gastrointestinal bleeding (UGIB), accounting for 6% of non-variceal bleeding and 1-2% of all UGIB<sup>2</sup>. DL can occur at any age but most commonly present clinically in the sixth or seventh decade of life<sup>3</sup>. Approximately 70% are found in the proximal stomach, with 15% found in the duodenum<sup>2</sup>. We present a case of a large DL at the second-third (D2/D3) aspect of the duodenum, which made treatment with traditional measures of adrenaline and clipping particularly challenging. Over-the-scope clips have been demonstrated to be an effective means of managing patients with non-variceal UGIB<sup>4</sup>. Whilst using a colonic over-the-scope (OVESCO<sup>TM</sup>) clip in the duodenum is uncommon, the procedure was successful with no adverse outcomes.</p><p><b><i>Case report:</i></b> An 89-year-old man underwent a gastroscopy to investigate recurrent melaena and profound iron deficiency anaemia. His medical history includes recurrent UGIB due to a suspected DL (previously managed with through-the scope clipping), atrial fibrillation (not on anticoagulation), ischemic heart disease and a transcatheter aortic valve implantation. His medications included pantoprazole, amlodipine, and furosemide. Urgent gastroscopy revealed an enlarged 7mm submucosal lesion on the medial floor of the D2/D3 with intermittent active arterial bleeding (Figure 1). Initial attempts with adrenaline injection and resolution<sup>TM</sup> clips failed to achieve haemostasis. Due to the location of the lesion, the endoscope was switched to a paediatric colonoscope. The decision was made to proceed with over-the-scope clipping due to ongoing bleeding and a large underlying arterial pulsation. A 14mm colonic over-the-scope clip was used as a smaller size (11/12mm) over-the-scope clip was not readily available. The clip was placed over the bleeding point capturing the entire lesion (Figures 2 & 3). The lesion was observed for 5 minutes post-therapy with no further ooze noted. The patient's haemoglobin remained stable over the coming days with resolved melaena and he was discharged home.</p><p><b>References</b></p><p>1. \n <span>Malik, T</span>, <span>Anjum, F</span>. <span>Dieulafoy Lesions Causing Gastrointestinal Bleeding</span>. StatPearls, <span>2017</span>.</p><p>2. \n <span>Nojkov, B</span>, <span>Cappell, M</span>. <span>Gastrointestinal bleeding from Dieulafoy’s lesion: clinical presentation, endoscopic findings, and endoscopic therapy</span>. <i>World J Gastrointest Endosc</i>, <span>2015</span>; <span>7</span>(<span>4</span>): <span>295</span>–<span>307</span>.</p><p>3. \n <span>Baxter, M</span>, <span>Aly, EH</span>: <span>Dieulafoy’s lesion: current trends in diagnosis and management</span>. <i>Ann R Coll Surg Engl</i> <span>2010</span>; <span>92</span>(<span>7</span>): <span>548</span>–<span>554</span>.</p><p>4. \n <span>Qiu, J</span> et al. <span>Over-the-Scope Clip Applications as First Line Therapy in the Treatment of Upper Non-variceal Gastrointestinal Bleeding</span>, Perforations and Fistulas. <i>Front Med (Lausanne)</i> <span>2022</span>; <span>9</span>:753956.</p><p><b>72</b></p><p><b>Penetrating injury and retained toothpick fragment causing bleeding from oesophageal varix</b></p><p><b>Elaine Koh</b><sup>1</sup>, Vikram Rao<sup>1</sup>, Kim Hay Be<sup>1,2</sup> and Leonardo Zorron Cheng Tao Pu<sup>1,2,3</sup></p><p><sup>1</sup><i>Department of Gastroenterology, Peninsula Health, Australia;</i> <sup>2</sup><i>Department of Gastroenterology, Austin Health, Australia;</i> <sup>3</sup><i>Department of Surgery, University of Melbourne, Melbourne, Australia</i></p><p><b><i>Introduction:</i></b> A foreign body (FB) lodged within the gastrointestinal tract is a frequent presenting complaint amongst patients presenting to the emergency department. Despite the common nature of this presentation, there are no descriptions of cases where a FB has become embedded within an oesophageal varix. In this case report, we describe a cirrhotic patient presenting with haematemesis, with the eventual diagnosis of a toothpick fragment lodged within an oesophageal varix.</p><p><b><i>Case report:</i></b> A 50-year-old man with alcohol-related Child-Pugh C liver cirrhosis presented with a 1-day history of epigastric pain and two episodes of haematemesis. This was in the setting of recently banded grade II oesophageal varices and a pre-emptive transjugular intrahepatic portosystemic shunt (TIPS) insertion a month prior. His haemoglobin was 101g/L on presentation, with no associated urea rise. An abdominopelvic CT scan demonstrated a patent TIPS. Given the patient’s risk factors and concerning history, an urgent gastroscopy was performed. Grade I varices were found in the lower third of the oesophagus, with an area of yellow discoloration noted (Figure 1A). On closer inspection, this appeared to be a solid FB embedded within an oesophageal varix. A single band was applied to the culprit varix, causing the FB to protrude into the lumen (Figure 1B). Given haemostasis had been achieved, the FB was not removed due to the risk of precipitating further bleeding. On further assessment of this patient’s history, this FB was deemed likely to be a fragment of a toothpick accidentally swallowed by the patient while intoxicated. The patient remained stable overnight and was discharged the following day. Though he had a subsequent alcohol-related presentation to our centre, he has yet to attend a follow-up gastroscopy or outpatient clinic appointments despite multiple attempts.</p><p><b>78</b></p><p><b>Stuck in transit: Food retention in ERCP for liver transplant patients</b></p><p><b>Vicki McGarrigle</b>, Marios Efthymiou, Rhys Vaughan and Sujievvan Chandran</p><p><i>Austin Health, Melbourne, Australia</i></p><p><b><i>Introduction:</i></b> Food retention during Endoscopic Retrograde Cholangiopancreatography (ERCP) poses significant risks such as aspiration and can lead to procedure delays. Food retention following fasting over four hours is associated with gastroparesis. Liver transplant patients have increased rates of diabetes, which can lead to gastroparesis. Solid organ transplant recipients are known to have higher rates of gastroparesis.</p><p><b><i>Methods:</i></b> A retrospective analysis was performed on patients who underwent ERCP between 2022 and 2024. Data from 525 procedures were collected to date, including variables such as food retention, liver transplant, diabetes, and gastric surgery.</p><p><b><i>Results:</i></b> A total of 525 ERCPs were analysed (mean age 62 years). Food was present in 3% of total procedures. Thirty-one percent of ERCPs were in liver transplant patients. Twenty-four percent of procedures were in diabetic patients. A significant association was observed between food retention and liver transplant recipients using Pearson’s Chi-squared test (p=0.03). However, there was no association using logistic regression analysis. Age was inversely associated with food retention.</p><p><b><i>Discussion:</i></b> The results indicate a higher likelihood of food retention in liver transplant patients during ERCP, although this association was not held with logistic regression analysis. Understanding the factors that cause food retention during ERCP is crucial in determining the need for pre-procedure prokinetics in high-risk groups. To achieve this, we plan to collect further data and increase our sample size to better identify the factors leading to food retention. This data is essential for optimal patient preparation, reducing procedure delays, and improving patient outcomes.</p><p><b>81</b></p><p><b>Safety of endoscopist directed procedural sedation in patients with severe obesity</b></p><p><b>Raymond Lewandowski</b>, Montri Gururatsakul, Keith Brick and Peter Boyd</p><p><i>Cairns Base Hospital, Cairns, Australia</i></p><p><b><i>Background and Aim:</i></b> According to Australian Institute of Health and Welfare data, 33% of men and 30% of women are living with obesity and 12% are living with severe obesity, which is defined as having a BMI of 35 or more. Presentations for endoscopic procedures in this population will increase as well. Endoscopist directed sedation has been demonstrated to be safe in low-risk populations. The aim of this review is to determine whether this safety expectation can be expanded to this high-risk group.</p><p><b><i>Methods:</i></b> An audit was conducted of patients presenting to our unit for endoscopic procedures between January 2022 and April 2023. Outcomes were evaluated based on model of sedation, BMI and ASA category and complications related to sedation.</p><p><b><i>Results:</i></b> 904 endoscopic procedures were performed in our unit on patients with a BMI ≥35 during the time covered by this review including 57 patients with BMI ≥50. 805 (89%) received endoscopist directed sedation, the remaining 99 had sedation provided by an anaesthetic team. The majority of patients in the endoscopist directed group received propofol and midazolam for sedation. There were a total of 4 complications related to sedation in the endoscopist directed group representing 0.49% of patients. Complications included two episodes of bradycardia, one laryngospasm and one transient hypoxic episode. Only one complication, laryngospasm, led to the discontinuation of the procedure.</p><p><b><i>Conclusion:</i></b> Endoscopist directed sedation is a safe model for sedation in endoscopic procedures performed in patients with BMI ≥35.</p><p>\n \n </p><p><b>89</b></p><p><b>Iron deficiency without anaemia: to scope or not to scope?</b></p><p><b>Zainul Azhar</b> and Rozemary Karamatic</p><p><i>Townsville University Hospital, Townsville, Australia</i></p><p><b><i>Background and Aim:</i></b> Iron deficiency is a common indication for endoscopic assessment, with endoscopy guidelines available to guide the decision to refer. Commonly, patients will have iron deficiency without anaemia. There remains a paucity of evidence for proceeding to endoscopy in iron deficient patients without anaemia. The research aims to explore endoscopic yield of non-anaemic iron deficient (NAID) patients, comparing their counterparts with iron deficiency anaemia (IDA)</p><p><b><i>Methods:</i></b> We conducted a retrospective study of 421 patients with iron deficiency referred for endoscopic assessment to a regional tertiary hospital in Queensland from 2022 to 2023. Inclusion criteria is patients ≥ 15 years old and iron deficiency defined as respective laboratory parameters at time of referral. Outcome measures include age, premenopausal status, use of prior iron supplementation, presence and nature of clinically significant lesions causing iron deficiency, malignancy rate, use of antiplatelet and anticoagulants. Multiple logistic regression was used to determine predictors of malignancy.</p><p><b><i>Results:</i></b> There were significantly lower rates of malignancy in the NAID arm compared to IDA arm (7.61%, 2.68%, p 0.02). In subgroup analyses, non-anaemia females (NAF) had lower malignancy rates than the anaemia group, among pre-menopausal (PRMF) (1.25% vs 2.94%, p 0.53) and post-menopausal (POMF) group (1.56% vs 7.02%, p = 0.13) respectively. Among non-anaemic females, malignancy rate showed no difference between PRMF and POMF (1.56% vs 1.25%, p 0.87). Significant predictors of malignancy were anaemia (OR 2.97, p 0.03) and presence of overt bleeding (OR 2.91, p 0.03). There were also significantly lower rates of non-neoplastic causes in NAID arm compared to IDA arm (56.70% vs 72.08%, p < 0.01). The most common finding in esophagogastroduodenoscopy in NAID group is <i>Helicobacter</i> pylori gastritis (8.48%) while gastric or duodenal erosions is the most common in the IDA group (7.61%). For colonoscopy, the most common findings in the NAID and IDA group is haemorrhoids (4.91%) and colonic angioectasias (4.59%) respectively.</p><p><b><i>Conclusion:</i></b> Our evidence demonstrates that non-anaemic iron deficiency confers a lower risk of gastrointestinal malignancy and detection of non-neoplastic pathology compared to iron deficiency anaemia. Further studies with larger sample sizes are needed to show statistical significance. The decision to proceed or not to proceed to endoscopic assessment among low-risk individuals and rationalize the use of a limited resource can be informed by these results.</p><p><b>91</b></p><p><b>Use of artificial intelligence improves colonoscopy performance in adenoma detection: A systematic review and meta-analysis</b></p><p><b>Jonathan Makar</b><sup>1</sup>, Jonathan Abdelmalak<sup>2,3,4</sup>, Danny Con<sup>1,2</sup>, Bilal Hafeez<sup>1</sup> and Mayur Garg<sup>1,5</sup></p><p><sup>1</sup><i>The University of Melbourne, Melbourne, Australia;</i> <sup>2</sup><i>Department of Gastroenterology, Austin Hospital, Melbourne, Australia;</i> <sup>3</sup><i>Department of Gastroenterology, Alfred Hospital, Melbourne, Australia;</i> <sup>4</sup><i>Central Clinical School, Monash University, Melbourne, Australia;</i> <sup>5</sup><i>Department of Gastroenterology, Northern Health, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> Artificial intelligence (AI) is increasingly used to improve adenoma detection during colonoscopy. This meta-analysis aimed to provide an updated evaluation of computer-aided detection (CADe) systems and their impact on key colonoscopy quality indicators.</p><p><b><i>Methods:</i></b> We searched the Embase, PubMed and MEDLINE databases from inception until February 15, 2024, for randomised control trials (RCTs) comparing the performance CADe systems with routine unassisted colonoscopy in the detection of colorectal adenomas.</p><p><b><i>Results:</i></b> 28 RCTs were selected for inclusion comprising 23861 participants. Random-effects meta-analysis demonstrated a significant 20% increase in adenoma detection rate (ADR, RR 1.20, 95% CI 1.14-1.27, p < 0.01) and 55% decrease in adenoma miss rate (AMR, RR 0.45, 95% CI 0.37-0.54, p < 0.01) with AI-assisted colonoscopy. Subgroup analyses revealed CADe-associated benefits for ADR persisted when considering only expert endoscopists (RR 1.19, 95% CI 1.11-1.27, p < 0.001) and remained for all investigated CADe systems and in both hospital and day-procedure settings. CADe use also significantly increased adenomas per colonoscopy (weighted mean difference 0.21, 95% CI 0.14-0.29, p < 0.01). Subgroup analysis of 8 studies reporting total adenomas categorised by size showed a significant benefit with regards to diminutive lesion detection (IRR 1.46, 95% CI 1.19-1.80, p< 0·001) for the CADe supported study arms, with a non-significant trend towards improved detection associated with small (IRR 1.11, 95% CI 0.94-1.31, p = 0.20) and large polyps (IRR 1.24, 95% CI 0.94-1.62, p = 0.12). Sessile serrated lesion detection (RR 1.10, 95% CI 0.93-1.30, p = 0.27) or miss rates (RR 0.44, 95% CI 0.16-1.19, p = 0.11) were not improved when all CADe systems were combined. There was an average 0.15 minute prolongation of withdrawal time with AI-assisted colonoscopy (weighted mean difference 0.15, 95% CI 0.04-0.25, p = 0.01).</p><p><b>95</b></p><p><b>Small intestinal bacterial overgrowth as assessed by breath testing: a prospective evaluation to the gold standard aspirate</b></p><p><b>Ayesha Shah</b><sup>1,2</sup>, <b>Teressa Hansen</b><sup>1</sup>, Thomas Fairlie<sup>1,2</sup>, Natasha Koloski<sup>1,2,3</sup>, Mike Jones<sup>4</sup> and Gerald Holtmann<sup>1,2</sup></p><p><sup>1</sup><i>Princess Alexandra Hospital, Metro South Health, Brisbane, Australia;</i> <sup>2</sup><i>The University of Queensland, Brisbane, Australia;</i> <sup>3</sup><i>The University of Newcastle, Newcastle, Australia;</i> <sup>4</sup><i>Macquarie University, Sydney, Australia</i></p><p><b><i>Background:</i></b> Small intestinal bacterial overgrowth (SIBO) is defined as the presence of excessive and abnormal types of bacteria in the small intestine. SIBO has been linked to several gastrointestinal and extraintestinal diseases. While small bowel aspiration and culture is the accepted gold standard for diagnosis, glucose breath testing (GBT) is widely used in the routine clinical setting. We aimed to prospectively compare in the routine clinical setting results of the GBT with duodenal aspirate and culture for diagnosing SIBO.</p><p><b><i>Methods:</i></b> We prospectively recruited patients between 2019-2023 with clinical suspicion of SIBO who underwent GBT as well as a gastroscopy and aspirate collected from the third part of the duodenum and cultured utilizing previously published methods (1). We calculated the sensitivity, specificity, positive and negative predictive value for the GBT against the duodenal aspirate and culture.</p><p><b><i>Results:</i></b> The final dataset included 131 patients with suspected SIBO who underwent GBT and had duodenal aspirate collected. The cohort had an average age of 43.2 ±15.6 years, with 73% female. Based upon duodenal aspirates and culture, 51 (38.9%, 95% CI 30.5-47.8) patients were positive for SIBO, at a cut off threshold of ≥10<sup>3</sup> colony forming units of bacteria/ml (Table 1). In contrast based upon the GBT, 13/131 (9.9%, 95% CI 5.4-16.4) tested positive for SIBO. Compared with the reference standard of small bowel aspirate and culture, GBT had accuracy of 55.7% (sensitivity 5.9%, specificity 87.5%).</p><p>\n \n </p><p><b><i>Conclusion:</i></b> The results of this large prospective single centre study shows that GBT has poor sensitivity but good specificity when compared to duodenal aspirate and culture for diagnosing SIBO. However, there is lack of universal acceptance and validation of small bowel aspirate and culture as the gold standard for diagnosing SIBO. This highlights the urgent need to develop better validated diagnostic tests for SIBO in routine clinical settings.</p><p><b>Reference</b></p><p>\n 1. <span>Shah, A</span>, <span>Talley, NJ</span>, <span>Koloski, N</span>, <span>Macdonald, GA</span>, <span>Kendall, BJ</span>, <span>Shanahan, ER</span>, et al. <span>Duodenal bacterial load as determined by quantitative polymerase chain reaction in asymptomatic controls, functional gastrointestinal disorders and inflammatory bowel disease</span>. <i>Alimentary pharmacology & therapeutics.</i> <span>2020</span>; <span>52</span>(<span>1</span>): <span>155</span>-<span>67</span>.</p><p><b>104</b></p><p><b>The effect of computer aided detection system availability on polyp detection during colonoscopy in a real-life scenario</b></p><p><b>Vikram Rao</b><sup>1</sup>, <b>Gordon Chen</b><sup>1</sup>, Elaine Koh<sup>1</sup>, Sheng Wei Lo<sup>1</sup>, Ibrahim Al Ansari<sup>2</sup>, Josephine Wanandi<sup>1</sup>, Brian Chow<sup>1</sup>, Marcus Robertson<sup>1</sup>, Leonardo Zorron Cheng Tao Pu<sup>1,3,4</sup> and Kim Hay Be<sup>1</sup></p><p><sup>1</sup><i>Department of Gastroenterology, Peninsula Health, Melbourne, Australia;</i> <sup>2</sup><i>Department of Medicine, Monash University, Melbourne, Australia;</i> <sup>3</sup><i>Department of Gastroenterology, Austin Health, Melbourne, Australia;</i> <sup>4</sup><i>Department of Surgery, University of Melbourne, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> One of colonoscopy's primary aims is to detect and remove precancerous polyps. Several studies have demonstrated that the use of computer aided detection (CADe) technology improves metrics such as the adenoma detection rate (ADR). Implementation of CADe is not yet standard practice across endoscopy centres, and even when available, uptake is variable amongst endoscopists. This makes it questionable if the results from controlled studies can be extrapolated to the real-world scenario. This study assessed the real-world effect of CADe availability on ADR.</p><p><b><i>Methods:</i></b> A single-centre retrospective observational study was performed at a metropolitan tertiary centre following the introduction of the Olympus Endo-AID module in July 2023. All colonoscopy reports generated through the network’s reporting software (Endobase) were examined 7-months prior to, and 7-months after the introduction of CADe. Inclusion criteria were: i) patients aged ≥ 40 years, and ii) colonoscopies performed for screening or surveillance. Endoscopists who did not perform eligible colonoscopies in both periods of the study were excluded. Emergency colonoscopies (e.g. for acute colitis, foreign body extraction or suspected active bleeding) were excluded. The frequency of use of CADe by each endoscopist was assessed as: i) Uses CADe for 100% procedures; ii) uses CADe for ≥ 50% procedures; iii) uses CADe for < 50% of the time; or iv) 0% CADe use. The primary outcome was the comparison of ADR before and after introduction of CADe.</p><p><b><i>Results:</i></b> Seven endoscopists performed a total of 636 eligible pre-CADe and 386 post-CADe colonoscopies during the study period. No statistically significant differences in baseline pre- and post-CADe procedure data were identified regarding age, gender, procedure indication, bowel preparation score or the endoscopist’s specialty. ADR was significantly improved for endoscopists with a baseline pre-CADe ADR between 25-50%, regardless of whether it was used for every procedure. This effect was not seen for endoscopists with an ADR >50% at baseline pre-CADe, even though for this group CADe use was 100%. Only one endoscopist with a baseline ADR of less than 25% did not show improvement, despite CADe use for more than 75% of the time. However, this endoscopist had only 10% of all their colonoscopies for the study period done after introduction of CAD.</p><p>\n \n </p><p><b><i>Conclusion:</i></b> Availability of CADe significantly improved ADR for endoscopists with baseline ADR 25-50%, even if not being used consistently for all procedures. The single endoscopist in this group that did not show improvement is likely due to the low numbers of post-CADe eligible colonoscopies within the study period. The observed effect was not seen in those with a baseline ADR pre-CADe > 50%. These results support the introduction of CADe even if it is not used for every colonoscopy by all endoscopists.</p><p><b>118</b></p><p><b>EPIC: A novel scoring system to identify patients likely to benefit from extended bowel preparation at index colonoscopy</b></p><p><b>Matthew Smale</b> and <b>Lok Lee</b> and Jeremy Humphris</p><p><i>Wollongong Hospital, Wollongong, Australia</i></p><p><b><i>Background:</i></b> Despite concerted intervention, bowel preparation remains inadequate in 18-35% of colonoscopies, resulting in reduced caecal intubation rate and adenoma detection rate, and increased procedure time and adverse events.<sup>1</sup> For the patient, this increases the risk of delayed diagnosis and disease progression. For the healthcare system, it increases the need for repeat colonoscopy.<sup>2</sup> Several studies have identified risk factors for inadequate bowel preparation. Four demonstrate predictive models for identifying patients at risk of inadequate bowel preparation, including Dik et al (2015).<sup>3</sup> No predictive model, however, can be generalised to patients at their index colonoscopy, where the benefit is arguably greatest.</p><p><b><i>Aim:</i></b> We designed and validated a novel scoring system,”EPIC”, that identifies patients at risk of inadequate bowel preparation using established patient risk factors at their index colonoscopy.</p><p><b><i>Methods:</i></b> Risk factors for EPIC were taken from a systematic review and meta-analysis by Mahmood et al (2018)<sup>1</sup>, which reviewed 24 studies and therein the outcomes of 49,868 colonoscopies. Risk factors and associated odds ratios (ORs) were cirrhosis (OR 0.49), stroke (OR 0.51), tricyclic antidepressant use (OR 0.51), diabetes mellitus (OR 0.58), hypertension (OR 0.58), narcotic use (OR 0.59), history of constipation (OR 0.61) and male gender (OR 0.85). We assigned points based on their ORs in a similar fashion to Dik et al (2015). Three points were assigned to cirrhosis, stroke and TCA use; two points to diabetes mellitus, hypertension, narcotic use and history of constipation; one point to male gender. To validate the system, we collected retrospective data for 500 index colonoscopies from our hospital’s endoscopy database. This included patient age, gender, BBPS and the aforementioned risk factors. ASA score and history of previous abdominal surgery were also collected to allow comparison of the EPIC scoring system with Dik et al (2015).</p><p><b><i>Results:</i></b> The median age was 60 years (253 patients male, 247 female). 13.4% had inadequate bowel preparation (total BBPS < 6 or individual segment of 1). Using EPIC, a score of 3 or more was the optimal threshold for predicting inadequate bowel preparation (sensitivity 58%, specificity 71%, PPV 0.24, NPV 0.92). Comparatively, using the Dik et al system, a score of 2 or more was the optimal threshold (sensitivity 36%, specificity 88%, PPV 0.32, NPV 0.90). A ROC analysis found a similar area under the ROC curve of 0.67 (p<0.002, standard error = .04) for each system (Figure 1). However, higher NPV and sensitivity using EPIC renders it a stronger performing scoring system in this population for screening. A binary logistical regression suggested a score of 3 or more was associated with 3.54 times greater odds of inadequate bowel preparation compared to a score of 2 or less, p < 0.001. A Mann-Whitney U test suggested a score of 3 or more was associated with a mean BBPS 2.17 points (out of 9) lower compared to a score of 2 or less (p=.03).</p><p><b>References</b></p><p><b>134</b></p><p><b>Comparison of artificial intelligence enhanced versus conventional reading in small bowel capsule endoscopy: a multi-centre australia based study</b></p><p><b>Phillip Leaver</b><sup>1,2</sup>, Fiona Tudehope<sup>1</sup>, Kevin Choi<sup>3</sup>, Sneha John<sup>4</sup>, Aman Yadav<sup>4</sup>, Arthur J Kaffes<sup>3</sup> and Robert B Feller<sup>1,2</sup></p><p><sup>1</sup><i>Department of Gastroenterology & Hepatology, St Vincent’s Hospital, Sydney, Australia;</i> <sup>2</sup><i>St Vincent’s Clinical School, The University of New South Wales, Sydney, Australia;</i> <sup>3</sup><i>AW Morrow Gastroenterology and Liver Centre, Royal Prince Alfred Hospital, Sydney, Australia;</i> <sup>4</sup><i>Department of Gastroenterology, Gold Coast University Hospital, Gold Coast, Australia</i></p><p><b><i>Background and Aim:</i></b> Capsule endoscopy is a proven, useful, minimally invasive tool for the investigation of small bowel pathology, particularly suspected small bowel bleeding. Important practical limitations include physician reading times and the risk of reader fatigue. The advent of artificial intelligence (AI) assisted reading software has the potential to significantly reduce reading time without compromising efficacy. Our aim was to compare conventional and AI assisted reading modes with respect to reading times and findings, from studies performed at a number of Tertiary Australian sites.</p><p><b><i>Methods:</i></b> 30 patients who underwent routine capsule endoscopy with the OMOM<i>®</i> capsule for investigation of obscure gastrointestinal bleeding were retrospectively analysed across three tertiary Australian hospitals. Included patients were over 18-years-old, had suspected overt or occult small bowel bleeding and no known small bowel strictures or Peutz-Jegher syndrome. OMOM<i>®</i> capsule ingestion and post-ingestion protocol were as per standard method. A conventional read (CR) at a frame rate of 12 frames per second was conducted by an experienced capsule endoscopist. The AI enhanced mode (Smart scan-assisted read- SSAR®) was then used for a second read. Comparison was made between the two in the following domains: reading time, reporting time, total number of findings, number of significant findings (using the Sarin classification: P0 insignificant, P1 uncertain, P2 definite). Statistical significance was assessed using the Student t-test.</p><p><b><i>Results:</i></b> All thirty patients were included in data analysis. Mean reading time by CR was 29.26 minutes vs 2.96 minutes by SSAR (p<.001). Mean reporting time showed no significant difference (p= 0.654). Comparison of capsule findings across all patients – P2 lesions: CR 57 vs 63 by SSAR (p=0.264), P1 lesions: CR identified 109 vs 70 by SSAR (p=0.032), P0 lesions: CR identified 32 vs 22 by SSAR (p=0.057). The most frequent P2 lesions were angioectasias (n=35/42) followed by ulcers (n=22/20), blood (n=13/13) and tumours (n=4/6). The most common P1 lesions were red spots (n=83/45).</p><p><b>143</b></p><p><b>Quality improvement using an electronic referral pathway for endoscopic procedures</b></p><p><b>Brigid Pinnuck</b><sup>1</sup>, Kirri Riley<sup>2</sup>, Sharon Gillespie<sup>3</sup>, Sharon Killin<sup>3</sup>, Nicola Mullaney<sup>3</sup>, Sarah Mendoza<sup>4</sup>, Amy Schafer<sup>2</sup> and Jane Andrews<sup>3,5</sup></p><p><sup>1</sup><i>Department of Gastroenterology and Hepatology, Royal Adelaide Hospital, Adelaide, Australia;</i> <sup>2</sup><i>Surgery Program, Central Adelaide Local Health Network, Adelaide, Australia;</i> <sup>3</sup><i>Central Adelaide Local Health Network, Adelaide, Australia;</i> <sup>4</sup><i>Gastrointestinal Investigation Unit, Royal Adelaide Hospital, Adelaide, Australia;</i> <sup>5</sup><i>Faculty of Health Sciences, University of Adelaide, Adelaide, Australia</i></p><p><b><i>Background:</i></b> Electronic referrals (e-referrals) for endoscopic procedures are becoming the standard of care. However, many healthcare organisations have more than one entry point for referrals, and this leads to unwarranted variation in triage and waiting times for those referred. Accurate triage against accepted indications is fundamental to delivering a quality, safe endoscopic service. Processing and managing large volumes of referrals also presents an administrative challenge, which digital platforms can support by ensuring no loss of referrals, booking in turn (by clinical urgency) and visibility along with audit.</p><p><b><i>Methods:</i></b> A consultation and co-design process was run over 18 months examining routine ambulatory endoscopic referrals across 2 sites in one health network. We identified referral entry points and necessary processes. A new agreed process was designed to harmonise practices across sites and reduce processing steps. To manage this new process, a digital platform (Novari ATC™was used. The new dual site, single pathway went live in October 2023. Data pre and post implementation were reviewed.</p><p><b><i>Results:</i></b> Since October 2023, 6,911 internal and external referrals were received, of which 5,799 were new referrals (n=558 staged). Of new referrals, colonoscopy (52.4%, n=3,036) was the most commonly referred procedure, followed by endoscopy (24.1%, n=1,399), colonoscopy and endoscopy (18.4%, n=1,066), flexible sigmoidoscopy (4.9%, n= 287) and endoscopy and flexible sigmoidoscopy (0.2%, n=11). To date, 3,609 of the new referrals have exited the pathway; 999 without a procedure, 2,488 were treated/scoped and 122 were diverted to outpatient department (OPD). Since going live, compared to May to October 2023, the number of weekly OPD additions for both colorectal and gastroenterology units decreased (colorectal by 45.9%, gastroenterology by 43.2%, and combined overall by 44.2%).</p><p><b><i>Conclusion:</i></b> Creating a single point for receipt, triage, assessment and scheduling of routine ambulatory endoscopic referrals in a digital platform has proved possible across 2 acute care sites. It has enabled us to better see and plan our work and to report on processes and outcomes transparently. It allows for these procedures to be delivered more consistently and reliably and to ensure that each person is verified to receive evidence-based guidelines at pathway exit, which will reduce the future number of inappropriate referrals via consumer and GP education. Significant savings in additions to OPD bookings have also been demonstrated, meaning that, people requiring OPD will have less waiting time and those where a procedure is clearly indicated can progress more rapidly without waiting for OPD.</p><p><b>Average weekly OPD additions before and after the e-referral pathway went live</b>\n \n </p><p><b>171</b></p><p><b>Dual snare endoscopic extraction of a gastric foreign body using a dual-channel endoscope: case report</b></p><p><b>Amitjeet Singh</b>, Edward Young and Rajvinder Singh</p><p><i>Department of Gastroenterology, Lyell McEwin Hospital, Adelaide, Australia</i></p><p><b><i>Introduction:</i></b> Foreign body ingestions are rare but can pose serious risks. Most pass naturally, but 10-20% require endoscopic removal, and 1% need surgery. Ingested foreign bodies can include organic material, such as food boluses, or non-organic objects, such as coins, toys, magnets or batteries. Foreign bodies are commonly removed endoscopically using forceps, snares, baskets and nets. The physical characteristics of ingested objects greatly influence the available techniques for safe and atraumatic endoscopic retrieval. Long and pointed foreign objects in the stomach are challenging to remove endoscopically and can cause complications such as tears or even perforation. The removal of long and sharp foreign objects has previously been described using a dual-snare technique using two endoscopes either simultaneously or successively. We present a novel case highlighting the use of dual snares with a dual-channel endoscope to safely manoeuvre a gastric foreign body using a push-pull technique.</p><p><b><i>Case report:</i></b> A 16-year-old female with a history of anxiety and depression had purposefully ingested a cigarette lighter three weeks prior to presentation. She presented to the hospital due to ongoing abdominal pain over two days duration. There were no significant findings on clinical examination, and laboratory investigations were unremarkable. An X-ray of the patient's abdomen showed a radiopaque foreign body in the left upper quadrant of the abdomen, likely within the gastric body. At endoscopy, a single cigarette lighter was in the gastric body with the metal cap removed, exposing a sharp plastic edge. Initially, grasping forceps were used but these would not capture the lighter adequately to traverse the lower oesophageal sphincter. A single snare was used, but this positioned the lighter perpendicular to the oesophageal lumen when the snare was tightened, which would have made retrieval dangerous. An attempt with an overtube was not attempted as the diameter of the object was too large and using a Roth Net was not attempted as it would not allow for appropriate orientation and could have led to difficulties in releasing the lighter. A dual-channel gastroscope was then used, facilitating the careful positioning of the lighter using two snares. One snare was placed over the rounded edge of the lighter, which was positioned cranially, while the second snare captured the sharp edge of the lighter and was positioned caudally using a push-pull technique (figure). The lighter could then be gradually pulled through the gastroesophageal junction and out of the mouth without complication. After removing the lighter, the scope was re-advanced, and there was no significant trauma.</p><p><b><i>Discussion:</i></b> This case demonstrates the use of dual snares through a dual-channel endoscope to successfully remove a long and sharp object from the stomach using a push-pull technique. Procedural challenges to removing such an object involve positioning the blunt end proximally to prevent perforation or impaction during extraction, orienting the object's long axis in the extraction line and applying traction to the foreign body without losing traction. The use of a push-pull technique has previously been described with other endoscopic accessories (balloons and snares); however, to our knowledge, it has not previously been described using dual snares with a dual-channel endoscope.</p><p><b>192</b></p><p><b>Changing aetiology and demographics of patients presenting with upper gastrointestinal bleeding at a tertiary hospital over a decade</b></p><p><b>Aparna Morgan</b>, Deniz Tuncer, Nirosha Pragash, Tharusha Dadallage, Angana Bajracharya, Leonardo Zorron Cheng Tao Pu and Richard La Nauze</p><p><i>Peninsula Health, Frankston, Australia</i></p><p><b><i>Background and Aim:</i></b> Upper gastrointestinal bleeding (UGIB) is a common and potentially life-threatening condition presenting to emergency departments worldwide. Anecdotally, the incidence of UGIB seems to have remained stable over the years, however the aetiology and demographics of patients have thought to have changed. In addition, over the last 10 years, novel endoscopic interventions have been developed to manage UGIB and presumably these have decreased rebleed and mortality rates. There are no recent studies validating these observations, especially in the Australian population. The aim of this retrospective audit is to compare the aetiology, demographics, management and outcomes of patients presenting with UGIB in the year 2012 compared to 2022. Being able to understand these changes can improve patient outcomes by informing clinical decision making and optimising healthcare resources.</p><p><b><i>Methods:</i></b> This study is a retrospective cohort study using electronic medical records to identify adult patients who presented with UGIB to a large tertiary hospital from 1/1/2012 to 31/12/2012 and the same period in 2022. Patients were identified using ICD-10 codes. Patients found to have a lower gastrointestinal bleed as the cause of the presentation during inpatient investigations, and patients that were discharged without having a gastroscopy, were excluded.</p><p><b><i>Results:</i></b> There were coincidentally exactly 161 patients who presented with UGIB in both 2012 and 2022. The average age of patients presenting with UGIB in 2012 was 69 years-old compared to 73 years-old in 2022, p=0.03. In 2012, 45% of patients had one or more comorbidities (liver disease, heart failure, ischaemic heart disease, chronic kidney disease or malignancy); this increased to 57% patients in 2022, p=0.03. There was also an increase in anticoagulation use in 2022 compared to 2012, (50 vs 17 patients, p <0.001). This was driven by an increase in direct-acting oral anticoagulation (DOAC) use, (39 vs 4 patients, p<0.0001) while Warfarin use remained the same (13 vs 9 patients, p=0.39). There was no difference in gender or rates of cancer. The rate of peptic ulcer disease as the primary aetiology and NSAID/Aspirin/PPI use, as well as incidence of H. Pylori, were similar. However, there was an increase in variceal bleeding in 2022 compared to 2012 (17 vs 4 patients, p<0.01). Endoscopic intervention also increased in 2022 compared to 2012. 21 patients underwent endoscopic intervention for UGI bleed in 2012 compared to 44 patients in 2022, p<0.001. There was no difference between rates of rebleeding, mortality or length of hospital stay.</p><p><b><i>Conclusion:</i></b> At our institution<b>,</b> aetiology and intervention for UGIB patients has changed between 2012 and 2022, now with increasing age, more comorbidities and anticoagulation use. Rates of peptic ulcer bleeds have remained the same but variceal bleeding has increased. Despite the increase in endoscopic intervention options, the rates of rebleed, mortality and length of hospital stay have remained the same. Further multi-centre studies are needed to validate these findings.</p><p><b>194</b></p><p><b>Effect of artificial intelligence on adenoma and polyp detection rate in a real-world, non-randomized setting</b></p><p><b>Jihan Harki</b><sup>1,2,3</sup>, Timothy O'Sullivan<sup>2,3</sup>, Kimberley Ryan<sup>2</sup>, Mehul Lamba<sup>2,3</sup>, <b>Paris Hoey</b><sup>2</sup>, Florian Grimpen<sup>2</sup>, Enoka Gonsalkorala<sup>2,3</sup>, Stacey Llewellyn<sup>4</sup>, Katherine Hanigan<sup>2,3</sup> and Mark Appleyard<sup>2,3</sup></p><p><sup>1</sup><i>Haga Ziekenhuis, The Hague, The Netherlands;</i> <sup>2</sup><i>Royal Brisbane and Women's Hospital, Brisbane, Australia;</i> <sup>3</sup><i>Surgical, Treatment and Rehabilitation Service, Brisbane, Australia;</i> <sup>4</sup><i>QIMR Berghofer Medical Research Institute, Brisbane, Australia</i></p><p><b><i>Background and Aim:</i></b> The benefit of computer-assisted detection systems (CADe) has been evaluated in several randomized controlled trials (RCTs) showing improved adenoma detection rate (ADR) (1-3). However, the generalizability of these studies is questioned as these studies are performed in highly controlled setting and thus not represent a real-world clinical setting (4). It is also believed that the increase in ADR is mainly observed in lower detector endoscopists (5, 6). We aimed to evaluate the effect of CADe-assisted colonoscopy on ADR in an actual clinical setting in a high-volume, non-tertiary endoscopy centre with high detector endoscopists.</p><p><b><i>Methods:</i></b> A single-centre, observational study was conducted on all patients undergoing colonoscopy due to symptoms of colorectal cancer (CRC), screening colonoscopies for CRC, post-polypectomy surveillance, or colonoscopy due to positive results from a fecal immunochemical test between March 2023 to October 2023. Colonoscopies were performed by 19 experienced endoscopists using the validated CADe system that allows for real-time image analysis. Historical procedural data regarding colonoscopies were obtained up to 10 months before the start of the study and were compared to the CADe-assisted colonoscopies in a 2:1 fashion. The primary outcome was the ADR. The secondary outcomes were polyp detection rate (PDR), advanced adenoma detection rate (AADR), serrated polyp detection rate (SDR) and mean number of polyps and adenomas per colonoscopy. Data were analyzed using logistic mixed effects models expressed as Odds ratio (OR) or Incidence rate ratio (IRR) with a 95% confidence interval (CI).</p><p><b><i>Results:</i></b> A total of 7444 colonoscopies were performed. ADR was significantly higher in the CADe-assisted colonoscopy group (50.7%) than in the control group (45.0%) (OR 1.26; 95% CI 1.13-1.41; p<0.001). The PDR was also significantly higher (67.3% vs 62.2%, OR 1.25; 95% CI 1.12-1.41; p<0.001) as was the advanced adenoma detection rate (AADR) (8.0% vs 6.5%, OR 1.26; 95% CI 1.07-1.49; p=0.007). The mean number of polyps per colonoscopy was significantly higher in the CADe group than in the standard group (1.78 vs 1.59, IRR 1.12, 95% CI 1.07-1.17; p<0.001) as was the mean number of adenomas per colonoscopy (0.82 vs 0.68, IRR 1.19; 95% CI 1.1.12-1.27; p<0.001).</p><p><b>215</b></p><p><b>Enhancing access to gastrointestinal endoscopy: a mixed methods evaluation of the endoscopist directed nurse-administered propofol sedation (EDNAPS) model</b></p><p>Ameya Godambe<sup>1</sup>, Elizabeth Watson<sup>1</sup>, Rhian Jones<sup>2</sup>, Angela Carberry<sup>2</sup> and <b>James O'Beirne</b><sup>1</sup></p><p><sup>1</sup><i>Sunshine Coast University Hospital, Birtinya, Australia;</i> <sup>2</sup><i>Sunshine Coast Health Institute, Birtinya, Australia</i></p><p><b><i>Background and Aim:</i></b> Many hospital and health services are experiencing increasing demand for diagnostic procedures such as colonoscopy. Increasing demand for services coincides with a national health workforce shortage felt most acutely in non-metropolitan areas, potentially leading to inequity of access to diagnostic tests needed to exclude serious conditions like cancer. Current delivery of endoscopy services is heavily reliant on sedation delivered by Anaesthetists. Expansion of access to endoscopy by flexible models of endoscopy delivery without reliance on anaesthetists have been proven to be safe and effective nationally and internationally. One such model is Endoscopist Directed Nurse-Administered Propofol Sedation (EDNAPS). We have implemented the EDNAPS model at our health service and through a comprehensive evaluation methodology, including patient data analysis, consumer surveys, and clinician feedback, the project sought to determine the value and benefits of the EDNAPS model for low-risk gastrointestinal endoscopy procedures.</p><p><b><i>Methods:</i></b> A mixed-method evaluation approach was adopted, incorporating both quantitative and qualitative data. Procedural data was collected from hospital electronic medical records and surveys were disseminated to collect patient and clinician experience measures.</p><p><b><i>Results:</i></b> A total of 120 EDNAPS procedures (all colonoscopy) have been performed to date. Analysis of post-anaesthesia care unit (PACU) recovery times revealed a statistically significant reduction for EDNAPS patients (median = 18 minutes) when compared to matched control patients (median = 24 minutes, p<0.001). Mean withdrawal time (13 minutes vs 16 minutes) and mean total procedure time (22 minutes vs 23 minutes) were not significantly different between EDNAPS patients and controls. There were no significant differences in adenoma detection rate (50% vs 49%) or sessile lesion detection rate (18% vs 27%) between EDNAPS procedures and controls. The patient experience surveys resulted in 22 EDNAPS and 26 control responses, being 19% and 22% respective recruitment rates. Most respondents from both groups (EDNAPS 77%, Controls 85%) rated the care that they had received as “very good”. Overall, patients felt that they were involved in decisions about their care and treatment (EDNAPS, 95%; Controls, 96%), had their procedure as soon as necessary (EDNAPS, 77%; Controls, 73%), were provided with materials that prepared them for their procedure (EDNAPS, 86%; Controls, 73%), and had an opportunity to ask the healthcare professional questions about the procedure (EDNAPS, 95%; Controls, 69%). No adverse patient outcomes, including hospital admissions following procedure, emergency department presentations within 72 hours, or mortality, were reported among EDNAPS patients. This indicates the safety and effectiveness of the EDNAPS model for eligible patients. The staff experiences survey had a total of eight responses (62% recruitment rate), covering a range of staff members from different professional streams, including nursing, medical and administration. Staff involved in EDNAPS procedures reported increased confidence and competence, attributing this to translational simulation exercises. These exercises facilitated a smooth implementation process and contributed to the successful adoption of the new model of care.</p><p><b><i>Conclusion:</i></b> The EDNAPS model has demonstrated its potential as a safe and efficient alternative for low-risk gastrointestinal endoscopic procedures at our health service. Reduced recovery times and high patient satisfaction indicate its efficacy in improving service delivery. Further optimization of training and procedural logistics is recommended to address clinician concerns and enhance the model’s sustainability. The findings support the broader adoption of EDNAPS within the public health sector.</p><p><b>218</b></p><p><b>Consumer acceptability of a novel point-of-care faecal immunochemical test</b></p><p><b>Alicia Dallisson</b><sup>1</sup>, Ms Geraldine Laven-law<sup>1</sup>, Robert Le Blanc<sup>2</sup>, Graeme Young<sup>1</sup>, Charles Cock<sup>1,3</sup> and Erin Symonds<sup>1,3</sup></p><p><sup>1</sup><i>Flinders University, College of Medicine and Public Health, Flinders Health and Medical Research Institute, Adelaide, Australia;</i> <sup>2</sup><i>Health First Systems Ltd, Harrow, United Kingdom;</i> <sup>3</sup><i>Department of Gastroenterology and Hepatology, Flinders Medical Centre, Southern Adelaide Local Health Network, Adelaide, Australia</i></p><p><b><i>Background and Aim:</i></b> Colorectal cancer (CRC) screening with the faecal immunochemical test (FIT) has proven effectiveness at reducing CRC incidence and mortality. While most CRC screening programs use FITs, fewer than 50% of people participate. Common non-participation reasons include a lack of familiarity with the test and aversion to faecal sampling. Therefore, a user-friendly approach is needed to increase screening participation. We assessed the acceptability of a novel FIT that samples toilet bowl water containing faeces and provides point-of-care (POC) results using a rapid antigen lateral-flow test, then compared acceptability between consumers with and without prior CRC screening experience.</p><p><b><i>Methods:</i></b> This pilot study provided South Australians (18-74 years) with the POC FIT, instructions, and a survey. A broad demographic was approached to ensure that consumers without prior CRC screening experience were also included. Consumers were asked to collect a sample of toilet bowl water after a bowel motion and apply this water to the rapid antigen test. Consumers interpreted their result according to instructions and completed a survey assessing their demographics, user experience, and preference of POC FIT versus other CRC screening tests. Survey responses between those with and without prior CRC screening experience were compared using Chi-squared tests. A p-value <0.05 was considered statistically significant.</p><p><b><i>Results:</i></b> A total of 47 out of 52 (90.4%) invitees completed the POC FIT, with 53.2% (25/47) aged over 50 years and 59.6% (28/47) female. 80.9% (38/47) of participants had previously completed a CRC screening test. Most consumers (97.9%; 46/47) were confident they completed the test and read the results correctly, 97.8% (44/45) of consumers were satisfied to obtain an immediate result, and 97.8% (45/46) indicated they would feel comfortable reporting a positive result to their doctor. Useability responses were not significantly different between consumers with and without prior CRC screening experience (p>0.05, Table). Most participants who had previously completed a CRC screening test (64.9%, 24/37) preferred the POC FIT to other CRC screening tests commenting that it was easier, cleaner and quicker. Just two consumers (5.4%, 2/37) preferred other CRC screening tests with 29.7% (11/37) not having a preference between testing types.</p><p><b><i>Conclusion:</i></b> The novel POC FIT was well-received and may provide a simple and familiar way of testing to enhance CRC screening participation. Larger studies assessing the user preference and diagnostic accuracy of the POC FIT are warranted.</p><p><b>Table.</b> Comparison of user experience of POC FIT based on CRC screening experience\n\n </p><p><b>235</b></p><p><b>Clinical outcomes following incomplete surveillance colonoscopies in patients at increased risk of colorectal cancer</b></p><p><b>Syme Aftab</b><sup>1</sup>, Michelle Coats<sup>2</sup>, Kalindra Simpson<sup>2</sup>, Charles Cock<sup>2</sup> and Erin Symonds<sup>2,3</sup></p><p><sup>1</sup><i>Department of Medicine, Flinders University, Adelaide, Australia;</i> <sup>2</sup><i>Department of Gastroenterology and Hepatology, Flinders Medical Centre, Adelaide, Australia;</i> <sup>3</sup><i>Flinders Health and Medical Research Institute, Flinders University, Adelaide, Australia</i></p><p><b><i>Background and Aim:</i></b> Optical colonoscopy is the gold standard for colonic surveillance. Following incomplete colonoscopies (i.e., intubation fails to reach the caecum/terminal ileum), computerised tomography colonography (CTC) is recommended to complete colonic evaluation. However, the role of CTC following incomplete colonoscopies in the increased risk surveillance population is unknown. The aim of this study was to review the reason for incomplete colonoscopies in a surveillance population, and to assess the potential role of CTC in completing evaluation.</p><p><b><i>Methods:</i></b> Incomplete surveillance colonoscopies in a public hospital setting (Jan 2017-Dec 2022) were audited. Procedures were excluded if the intended intubation site was distal to the caecum/terminal ileum. Data extracted from clinical reports included patient demographics, reasons for incomplete procedures, follow-up CTC results, and prevalence of advanced neoplasia at the next complete colonoscopy, by colonic site. Advanced neoplasia was defined as CRC or advanced pre-cancerous lesions (including adenomas ≥10mm, high-grade dysplasia; villosity, sessile serrated lesions ≥10mm or with dysplasia, traditional serrated adenomas, or ≥5 small tubular adenomas).</p><p><b><i>Results:</i></b> Among 153 eligible incomplete colonoscopies (median patient age: 64.7 years, SD 12.3 years; 44.4% (n=68) male), the leading reasons for incompletion were anatomy-related: significant looping, tortuous colon, angulation, or restricted colonic mobility (58.2%, n=89), followed by inadequate bowel preparation (34.6%, n=53) and patient discomfort (20.9%, n=32). More than one reason was reported in 34% of cases (n=52). For follow-up, 20.9% (n=32/153) underwent a CTC, 53.6% (n=82) underwent a colonoscopy, and 25.5% (n=39) had no documented complete investigation to date. Among the CTC group (median 8.5 days (IQR 0.0-65.5) after the incomplete procedure), 30 CTCs detected no polyps. When 11 of these cases had subsequent colonoscopies (25.6 months (IQR 9.8-30.9) after the incomplete colonoscopy), advanced neoplasia was detected in 27.3% (n=3) of individuals, including CRC (n=1). Among patients who had a repeat colonoscopy as their first follow-up procedure (3.6 months (IQR 1.1-11.1) after the incomplete procedure), 88% (n=72) had complete intubation. Advanced adenoma was detected in 29.2% (n=21/72) of cases, with 81.0% (n=17) of these adenomas in a site not reached by the previous incomplete colonoscopy.</p><p><b><i>Conclusion:</i></b> Abnormal anatomy, inadequate bowel preparation and patient discomfort were leading causes of incomplete surveillance colonoscopies. Follow-up colonoscopies revealed a significant rate of advanced neoplasia. With the focus in the increased risk surveillance population being detection and removal of advanced neoplasia, we conclude that CTC has a limited role following incomplete colonoscopy, and repeat colonoscopy should be the preferred approach.</p><p><b>258</b></p><p><b>A bruised TOE in the throat</b></p><p><b>Moshe Loebenstein</b>, Bowen Xia and Sam Hui</p><p><i>Monash Health, Melbourne, Australia</i></p><p><b><i>Introduction:</i></b> Oesophageal injury is a rare but important complication of transoesophageal echocardiography (TOE). We present a case of an extensive oesophageal haematoma presenting as odynophagia and dysphagia as a result of a TOE performed during a percutaneous mitral valve (MV) repair for severe mitral regurgitation.</p><p><b><i>Case report:</i></b> An 80 year old male with a history of cardiomyopathy, pulmonary hypertension, AF and CKD underwent a MV repair with a Halfmoon prosthesis. 12000IU of heparin were administered intraoperatively as per protocol. A TOE probe was placed for the duration of the procedure. Towards the end of the procedure, blood was noted in the oropharynx and nares. His haemoglobin dropped from 119g/L to 85g/L with a concurrent drop in blood pressure requiring vasopressor support and a blood transfusion. The patient was extubated one day after the procedure and commenced on warfarin. He reported severe throat and retrosternal pain with minimal oral intake. On nasoendoscopy there was a small bruise over the right palate with an otherwise normal exam. A contrast CT was recommended however the patient’s renal function (eGFR 25ml/min) precluded this. The patient commenced total parenteral nutrition (TPN) and an urgent gastroenterology opinion was requested. Endoscopic assessment was delayed due to supratherapeutic warfarinisation (INR 9.4) which was treated with intravenous Vitamin K. A gastroscopy was performed 6 days post the initial procedure which demonstrated an extensive linear submucosal haematoma (Figure 1a). The gastroscope was not progressed beyond the distal end of the haematoma due to risk of perforation. The patient was managed conservatively with cautious upgrading of his diet. 12 days after the initial injury parenteral nutrition was ceased. He was anticoagulated first with subcutaneous enoxaparin and then with warfarin. A CT chest with oral contrast performed 2 weeks after the procedure demonstrated residual oesophageal wall thickening but no perforation (Figure 1b).</p><p><b>292</b></p><p><b>Evaluation of demographics and outcomes of patients undergoing endoscopy after-hours</b></p><p><b>Zainab Abdul-Rahman</b>, Rohita Reji and Abhey Singh</p><p><i>Fiona Stanley Hospital, Perth, Australia</i></p><p><b><i>Background and Aim:</i></b> After-hours emergency endoscopic procedures are indicated in various settings and utilize significant healthcare resources. Current guidelines recommend performing an endoscopy within 24-hours of upper gastrointestinal bleeding (UGIB) presentation <sup>(1)</sup>. Studies have shown no difference in clinical outcomes in UGIB patients undergoing endoscopy in <6 hours compared to 6-24 hours after hospital presentation <sup>(1, 2)</sup>. We aimed to assess demographics and outcomes of patients undergoing endoscopy after-hours.</p><p><b><i>Methods:</i></b> We conducted a single-center retrospective cohort study of adult patients who underwent endoscopy afterhours (1700-0800) from Jan 2023-Jan 2024 at a major tertiary hospital in Western Australia. Information was collected from electronic medical records and analyzed using Graphpad Prism 10.2.3. Patients were categorized based on the timing of endoscopy: urgent (<6 hours) or early (6-24 hours) from presentation. Primary outcome assessed was 30-day all-cause mortality. Secondary outcomes included 30-day rebleeding rate, 30-day ICU admission and length of hospital stay (LOS).</p><p><b><i>Results:</i></b> The study included 126 patients, with a mean age of 63 years. 63% (79/126) of cases had afterhours endoscopy for UGIB and 37% (47/126) for non-UGIB. 79% (100/126) of patients required a therapeutic endoscopic intervention. Among UGIB patients, 30% (24/79) were variceal and 70% (55/79) were non-variceal. 56% (44/79) of UGIB patients had endoscopy within 6 hours and 44% (35/79) within 6-24 hours. 30-day all-cause mortality was 9.5% (12/126) among the whole cohort and 11.4% (9/79) among patients with UGIB (9.1% in non-variceal bleeding group vs 17% in variceal UGIB). The mean age of death was 67.6 years. In the non-variceal UGIB group, 4/5 deaths were from complications of ongoing bleeding and 1 was due to underlying cancer. In the variceal UGIB group, all 4 deaths were from complications of chronic liver disease. There was no significant difference in the 30-day all-cause mortality between the urgent (13.6%, 6/44) and early (8.6%, 3/35) groups (p = >0.99, NS). Secondary outcomes of 30-day rebleeding rate and 30-day ICU admission were not significantly different between the two groups. However, the LOS was lower at 8 days in the urgent group vs 17 days in the early group (p = 0.039).</p><p><b><i>Conclusion:</i></b> Our study revealed a significant 30-day all-cause mortality of 9.5% among patients undergoing afterhours endoscopy, with most deaths occurring in patients with UGIB. There was no significant difference in 30-day all-cause mortality, 30-day rebleeding rate or ICU admissions of UGIB patients undergoing urgent (<6 hours) versus early endoscopy (6-24 hours). However, urgent endoscopy resulted in a significantly reduced LOS compared to early endoscopy. These findings align with previous observational studies and emphasize the importance of medical optimization before endoscopy. The high mortality rate among UGIB patients highlight the need for enhanced care of these patients such as by utilizing specialized UGIB units with strict protocols.</p><p>\n \n </p><p><b>References</b></p><p>1. \n <span>Lau, J.</span>, <span>Yu, Y.</span>, <span>Tang, R.</span>, et al. <span>Timing of Endoscopy for Acute Upper Gastrointestinal Bleeding</span>. <i>N Engl J Med</i> <span>2020</span>; <span>382</span>: <span>1299</span>-<span>1308</span>.</p><p>2. \n <span>Merola, E.</span>, <span>Michielan, A.</span> & <span>Pretis, G.</span> <span>Optimal timing of endoscopy for acute upper gastrointestinal bleeding: a systematic review and meta-analysis</span>. <i>Intern Emerg Med</i> <span>16</span>, <span>1331</span>–<span>1340</span> (<span>2021</span>). https://doi.org/10.1007/s11739-020-02563-1</p><p><b>297</b></p><p><b>A rare case of metastatic renal cell carcinoma to the stomach presenting as upper gastrointestinal bleeding</b></p><p><b>Gurtej Singh</b><sup>1</sup>, Nicholas Mingos<sup>1</sup>, Maeve Slevin<sup>2</sup> and Ashok Raj<sup>1</sup></p><p><sup>1</sup><i>Department of Gastroenterology, The Royal Melbourne Hospital, Melbourne, Australia;</i> <sup>2</sup><i>Department of Anatomical Pathology, The Royal Melbourne Hospital, Parkville, Australia</i></p><p><b><i>Background:</i></b> Renal cell carcinoma (RCC) accounts for 2.8% of cancer diagnoses in Australia. 25-30% of patients present with distant metastases at diagnosis with the commonest sites including the lungs, lymph nodes, bone and liver, and portending a poorer prognosis. Gastric metastases are exceedingly rare with few cases reported and an incidence of <1%. We report a unique case of a patient with metastatic RCC to the stomach presenting with upper gastrointestinal bleeding.</p><p><b><i>Case report:</i></b> A 73-year-old lady with a history of multiple sclerosis, previous bowel resection for diverticulitis presented with haematemesis and melaena. She reported a one year history of progressive fatigue, 20kg unintentional weight loss, and a one month history of dull right-sided abdominal pain. Laboratory studies revealed anaemia, leukocytosis and hypercalcaemia. Oesophagogastroduodenoscopy (OGD) revealed three 10-20mm sessile fundic gland polyps with stigmata of recent bleeding. All three polyps were injected with adrenaline, hot snared whilst haemostasis was achieved with soft coagulation and endo-clips. A contrast-enhanced computed tomography (CT) scan revealed a large 7cm heterogeneous mass in the right kidney with extrarenal extension into the perinephric space and extensive metastases to the liver and lungs. Histology of the gastric polyps showed high grade malignant spindle cells with smooth muscle differentiation consistent with sarcomatoid renal cell carcinoma. Further tissue biopsy was deemed unnecessary given the histology seen from polypectomy. The patient’s gastrointestinal bleeding resolved following OGD and polypectomy. Unfortunately, they had a liver metastases rupture three weeks after presentation and a palliative approach was taken.</p><p><b>301</b></p><p><b>Influence of endoscopic biopsy forceps characteristics on tissue specimens</b></p><p><b>Lulu Zhang</b><sup>1</sup>, Mark Bettington<sup>2</sup>, Mike Jones<sup>3</sup> and Nicholas Tutticci<sup>1</sup></p><p><sup>1</sup><i>QEII Jubilee Hospital, Brisbane, Australia;</i> <sup>2</sup><i>Envoi Specialist Pathologists, Brisbane, Australia;</i> <sup>3</sup><i>Macquarie University, Sydney, Australia</i></p><p><b><i>Background and Aim:</i></b> Tissue acquisition with biopsy forceps is routine during diagnostic endoscopic procedures. Currently a large variety of forceps are available characterised by differences in jaw size and shape, cup contour (“toothed/alligator cup” vs smooth) or a needle. Pathologic interpretation of biopsy specimens may be impacted by submucosal inclusion, orientation, and crush artifact. Historical studies consistently show jaw size is associated with larger samples. Studies comparing currently available forceps however are lacking, and there is heterogeneity in the preference for biopsy forceps among Endoscopists, as well as in their availability in Endoscopy units. Hence the aim our study was to assess the difference in tissue specimen quality between commonly used biopsy forceps.</p><p><b><i>Methods:</i></b> A retrospective pathologist-blinded cohort study was performed. Three biopsy forceps without needle (jaw toothed 2.4mm, smooth cup “toothless” 2.3mm, and jaw toothed 2.2mm) were trialled in an Endoscopy unit to gauge Endoscopist acceptability and inform procurement decisions. From this period, a blinded expert gastrointestinal Pathologist re-reviewed each tissue specimen obtained with these biopsy forceps during routine diagnostic endoscopy and/or colonoscopy. Specimens were assessed for size, orientation, crush artefact and the presence of submucosa. Statistical analysis comprised nonparametric Kruskal-Wallis test for null hypothesis of equality between forceps and three unique pairwise contrasts with Mann-Whitney test.</p><p><b><i>Results:</i></b> During the study period, 538 tissue specimens were collected (table 1). The largest forceps returned significantly larger mean specimen size compared to the smaller forceps (p<0.001). Most biopsy specimens did not contain submucosa (87%) however submucosa was more frequently identified in with the larger forceps (p=0.003). Smooth cup 2.3mm forceps had a higher proportion of poorly oriented specimens, while again, larger 2.4mm forceps had the least with poor orientation (p=0.04). All forceps, regardless of jaw contour, exhibited no crushing of tissue (100% intact). Further specific paired comparison between the smooth cup 2.3mm and toothed 2.2mm demonstrated no significant differences. No clinically significant adverse events were recorded in study patients and haemostatic techniques were not required for any biopsy sites.</p><p><b>309</b></p><p><b>Rare case of doxycycline-induced gastric mucosal injury</b></p><p><b>Christopher James Shephard</b> and Rozemary Karamatic</p><p><i>Department of Gastroenterology and Hepatology, Townsville University Hospital, Townsville, Australia</i></p><p><b><i>Introduction:</i></b> Doxycycline, a commonly prescribed tetracycline antibiotic, is a well-known cause of drug-induced oesophagitis and ulceration. In contrast, doxycycline-induced gastric mucosal injury (DGMI) is rarely encountered, with small bowel injury even less frequent. Patients may be asymptomatic or exhibit dysphagia, epigastric pain or anaemia due to gastrointestinal (GI) bleeding following a variable lead time (five days to three years). Gastric lesions are characterised by inflamed mucosa with overlying white-yellow plaque and/or ulceration. Histologically, drug-specific injury is depicted by eosinophilic degeneration of superficial capillaries and microthrombi formation with overlying mucosal necrosis. Additionally, reactive foveolar epithelial change, prominent lamina propria neutrophilic infiltrate and erosion/ulceration may be present. We report a case of DGMI to improve awareness regarding this infrequent adverse outcome of doxycycline use.</p><p><b><i>Case report:</i></b> A 78-year-old gentleman with diabetes, hypertension, ischaemic heart disease with coronary stenting, chronic kidney disease and chronic back pain was admitted with dyspnoea in the setting of pulmonary oedema due to non-ST segment elevation myocardial infarction and acute normocytic anaemia (haemoglobin 77g/L versus 122g/L from 13 days prior) with melaena concerning for upper GI bleeding. Eleven days earlier he commenced a 2-week course of doxycycline 100mg twice daily following evaluation for pyrexia of unknown origin. Relevant co-medications included aspirin and clopidogrel but no recent anti-inflammatory drug use. Platelet count and international normalised ratio were within normal limits. He was initially managed with temporary antiplatelet interruption, two units of packed red blood cells and high-dose intravenous pantoprazole. Oesophagogastroduodenoscopy revealed widespread gastritis involving the cardia, fundus, and gastric body with isolated white plaque-like lesions (figure 1) but no ulceration, and three small non-bleeding ulcers in the second portion of the duodenum. Gastric biopsy exhibited surface erosion with neutrophilic infiltration and reactive epithelial changes. Multiple superficial mucosal capillaries demonstrated degenerative change with eosinophilic necrosis and microthrombi formation, highly consistent with DGMI (figure 2). There was no evidence of <i>Helicobacter pylori,</i> viral cytopathic changes or dysplasia/neoplasia. Doxycycline was ceased and antiplatelet therapy was resumed under high-dose oral pantoprazole cover without re-bleeding. Without supportive biopsy, it remains unclear whether doxycycline also instigated duodenal ulceration in this case.</p><p><b>314</b></p><p><b>A serious case of post-colonoscopy colitis</b></p><p><b>Irene Lu</b>, Eliza Flanagan, Carl Cosgrave, Jack Shembrey and Damian Dowling</p><p><i>Barwon Health, University Hospital Geelong, Geelong, Australia</i></p><p><b><i>Introduction:</i></b> Immediate complications post-colonoscopy includes bleeding and perforation. Colitis as a complication of colonoscopy is incredibly rare. It has only been described in a few case reports (1,2) and often in patients with underlying medical conditions such as connective tissue disorders or vascular risk factors for ischaemia (3,4). There has been reports of chemical colitis from historical use of glutaraldehyde to clean colonoscopy equipment (5) and unexpected reports of ischaemic colitis with aggressive bowel preparation in constipated patients over the age of 75 (6). We report an unusual case of severe colitis post-colonoscopy without clear aetiology.</p><p><b><i>Case report:</i></b> A 70-year-old female with obesity and type-2 diabetes underwent routine endoscopy for investigation of iron deficiency anaemia and altered bowel habits. Colonoscopy revealed uncomplicated left-sided diverticular disease and a 5mm splenic flexure polyp removed via cold snare. Random colonic biopsies were taken. The day following colonoscopy she developed abdominal pain, profuse diarrhoea and vomiting. On day two post-colonoscopy, she presented to hospital due to worsening pain despite spontaneous resolution of her diarrhoea. On physical examination, she was found to have diffuse abdominal tenderness with profound hypotension. Her admission CRP was 416 mg/L with normal white-cell count. She was managed with vasopressor support, intravenous fluids and antibiotics, and subsequently continuous renal replacement therapy (CRRT) for anuric renal failure. Computer tomography (CT) revealed diffuse bowel wall thickening of the hepatic flexure, proximal and mid-transverse colon with adjacent fat stranding, without evidence of pneumoperitoneum or intra-abdominal collection. The patient did not open her bowels again until 4 days following presentation, whereby stool testing was negative for infection. Her renal function recovered but her admission was complicated by persistent abdominal pain and nausea limiting oral intake and necessitating total parenteral nutrition. Serial imaging revealed persistent and progressive inflammation of the hepatic flexure without radiological evidence of perforation or pneumoperitoneum. Exploratory laparotomy on day 19 revealed gross inflammation of the distal ascending and proximal transverse colon with multiple mesocolon abscesses and a contained abscess at the hepatic flexure. The patient underwent a right hemicolectomy with stoma formation. Histopathology of the bowel showed non-specific acute on chronic inflammation contained within the submucosal layer. The patient recovered on the ward and was discharged home 20 days post her operation.</p><p><b><i>Conclusion:</i></b> The aetiology of colitis in this post-colonoscopy case remains undifferentiated and has resulted in significant morbidity and prolonged hospitalisation. Whilst infective colitis resulting in bacterial septic shock remains a leading differential given the significantly raised inflammatory markers, the lack of positive faecal stool sampling and positive blood or urine culture remains contradictory. As a well-accepted complication, perforation remains possible, but this would typically present with localised radiological findings and would not proceed in this clinical course with organ dysfunction and subsequent histological findings of diffuse inflammation. Some case reports have demonstrated surprising diagnoses of ischaemic colitis after histopathological review, but our patient has a negative arterial phase CT and histological results are non-specific. Endoscopist should be aware of serious colitis as a potential, albeit rare, complication of diagnostic colonoscopy.</p><p><b>References</b></p><p>1. \n <span>Shah, Parin</span>; <span>Aggarwal, Aakash</span>; <span>Vaziri, Haleh</span>. <span>A Rare Case of Post Colonoscopy Colitis: 1351</span>. <i>American Journal of Gastroenterology</i> <span>111</span>:p <span>S607</span>, October 2016.</p><p>2. \n <span>Mathew, Madhu</span>; <span>Elkhouly, Mohamed A.</span>; <span>Mbachi, Chimezie U</span>. \n <span>et al</span>. <span>An Unusual Case of Post Colonoscopy Colitis - A Pathological Surprise: 1485</span>. <i>American Journal of Gastroenterology</i> <span>113</span>:p <span>S852</span>-<span>S853</span>, October 2018.</p><p>3. \n <span>Wheeldon, NM</span>, <span>Grundman, MJ</span>. <span>Ischaemic colitis as a complication of colonoscopy</span>. <i>BMJ</i> <span>1990</span>; <span>301</span>(<span>6760</span>): <span>1080</span>–<span>1081</span>.</p><p>4. \n <span>Versaci, A</span>, <span>Macrì, A</span>, <span>Scuderi, G</span>, <span>Bartolone, S</span>, <span>Familiari, L</span>, <span>Lupattelli, T</span>, et al. <span>Ischemic colitis following colonoscopy in a systemic lupus erythematosus patient: report of a case</span>. <i>Dis Colon Rectum</i> <span>2005</span>; <span>48</span> (<span>4</span>): <span>866</span>–<span>9</span>.</p><p>5. \n <span>Ahishali, E</span>. <span>Uygur-Bayramiçli, O</span>. <span>Dolapçioğlu, C</span>. <span>Dabak, R</span>. <span>Mengi, A</span>. <span>Işik, A</span>.et al. <span>Chemical colitis due to glutaraldehyde: case series and review of the literature</span> <i>Dig Dis Sci</i> Dec 23 <span>2008</span> e-pub ahead of print).</p><p>6. \n <span>Kawamura, T</span>, <span>Sakiyama, N</span>, <span>Tanaka, K</span>, <span>Yokota, I</span>, <span>Uno, K</span>, <span>Yasuda, K</span>. <span>Ischemic Colitis Caused by Bowel Preparation for Colonoscopy</span>. <i>Gastroenterology Res</i>. <span>2021</span> Oct; <span>14</span>(<span>5</span>): <span>296</span>-<span>303</span>. doi: https://doi.org/10.14740/gr1461. Epub 2021 Oct 14. PMID: 34804274; PMCID: PMC8577598</p><p><b>324</b></p><p><b>Endoscopic retrieval of a partially deflated intragastric balloon: a case report</b></p><p><b>Denis Rubtsov</b><sup>1</sup> and Nicholas Tutticci<sup>2</sup></p><p><sup>1</sup><i>The Prince Charles Hospital, Brisbane, Australia;</i> <sup>2</sup><i>Royal Brisbane and Women's Hospital, Brisbane, Australia</i></p><p><b><i>Introduction:</i></b> Fluid-filled intragastric balloon (IGB) is a widely utilised non-surgical weight loss modality. Advantages of reversibility and lower cost than bariatric surgery are offset by potential adverse events including balloon rupture, migration and bowel obstruction. There is no consensus on the optimal endoscopic technique for removal of a malfunctioning balloon. We report a case of a successful endoscopic removal of a ruptured and partially deflated IGB with long dwell time.</p><p><b><i>Case report:</i></b> A 51-year-old woman presented with a mild epigastric pain and blue-coloured urine. She underwent a placement of an Orbera® IGB (Apollo Endosurgery, Austin, Tex, USA) 18 months prior and elective removal of the balloon at 6 months was delayed in the context of a therapeutic relationship breakdown with the treating practitioner. She was haemodynamically stable on admission, reported no nausea, vomiting or other symptoms of bowel obstruction. However, a CT scan demonstrated a collapsed gastric balloon at the fundus extending through the pylorus into the duodenal bulb (Figure 1). Considering the impending risk of small bowel obstruction, the decision was made to retrieve the IGB emergently in an after-hours setting. Endoscopy was performed under general anaesthesia with endotracheal tube placement. The near completely deflated leaking IGB was found in the stomach. The manufacturer’s recommended draining equipment and balloon retractors were not readily available. Presumably due to the long dwell time of the balloon the material was stiff and inelastic. Attempted removal with a large polypectomy snare failed to grasp the convex balloon end. Attempted removal with a Rescue® Rat Tooth Grasping Forceps (Boston Scientific, Marlborough, MA, USA) failed due to residual fluid in the dependent component limiting passage beyond the lower oesophageal sphincter. The perishing balloon tore under tension. The forceps was then used to intentionally create a 15mm defect in the balloon which permitted complete drainage of IGB fluid with the gastroscope partially inserted into the balloon remnant. Secondly the defect permitted a polypectomy snare purchase of the end of the balloon where it previously slipped repeatedly due to the convex configuration. Atraumatic retrieval through the mouth was then uneventful.</p><p><b><i>Conclusion:</i></b> This case demonstrates endoscopic technique of a partially deflated IGB removal, utilising the equipment that is readily accessible to all endoscopists. This approach can be considered for balloons after a long dwell time where other techniques fail as it appears to be effective and safe.</p><p><b>338</b></p><p><b>Gastrointestinal stromal tumor presenting with life threatening haematemesis - a rare cause of upper gastrointestinal bleeding highlighting the importance of a multidisciplinary approach</b></p><p><b>Robert O'Neill</b><sup>1,2</sup>, Phillip Leaver<sup>1,2</sup>, Connor Ryan<sup>1,2</sup> and Ian Lockart<sup>1,2</sup></p><p><sup>1</sup><i>St Vincent's Hospital Sydney, Sydney, Australia;</i> <sup>2</sup><i>The University of New South Wales, Sydney, Australia</i></p><p><b><i>Introduction:</i></b> Gastrointestinal stromal tumours (GIST) are the most common type of mesenchymal tumor of the gastrointestinal tract. Clinical presentation is variable and is dependent on the tumor's location and size. Approximately 25% of GISTs manifest with recurrent gastrointestinal bleeding, however acute haematemesis with haemodynamic instability and shock is relatively uncommon. We present the case of a patient who presented to our institution with an acute episode of haematemesis secondary to an ulcerated gastric GIST.</p><p><b><i>Case report:</i></b> A 61-year-old male was brought in by ambulance to our institution with five episodes of haematesis and pre-syncopal symptoms. He had a medical history notable for a previous lumbar spine laminectomy. He was on no regular medications. On initial examination he was hypotensive to 80/50 mmHg and tachycardic with a heart rate of 122 bpm. Frank haematemesis on initial assessment. The remainder of his examination was normal. Initial biochemical assessment revealed a haemoglobin of 115 g/L and urea of 11.4 mmol/L with preserved renal function. Serum lactate was 2.2 mmol/L. Intravenous fluid resuscitation was commenced along with a pantoprazole infusion. The patient underwent emergent upper gastrointestinal endoscopy which revealed a large gastric mass (5 cm in size) which was 4 cm distal to the gastroesophageal junction over the posterior wall and fundus of the stomach (Figure 1a). Macroscopically the mass appeared to be submucosal in origin with preservation of the overlying mucosal architecture. A large ulcer measuring 1 cm in diameter was present on the posterior surface of the mass with a visible vessel present at the base (Forest class 2a). Bleeding was provoked on minimal trauma (Figure 1b). Haemospray was applied for haemostasis. Computed tomography abdomen was performed which demonstrated a well-circumscribed hypoattenuating lesion within the fundus of the posterior wall of the stomach measuring 30 x49 mm. Surgical opinion was sought and the patient underwent partial gastrectomy. Histopathological analysis of the resected specimen revealed a 40 mm gastric fundus GIST with clear surgical margins (AJCC pT2). The patient had an uncomplicated postoperative period and was discharged home.</p><p><b><i>Conclusion:</i></b> GISTs are a relatively uncommon benign gastrointestinal neoplasm that can present with variable symptoms ranging from indolent to hyperacute. This case highlights an uncommon presentation of a GIST with an acute upper gastrointestinal haemorrhage and highlights the importance of multidisciplinary management and definitive surgical management given the limited scope of endoscopy.</p><p><b>344</b></p><p><b>Eosinophilic gastroenteritis with mucosal and serosal involvement: A rare cause of abdominal pain and ascites</b></p><p><b>Georgia Zeng</b><sup>1,2</sup>, <b>Robert O'Neill</b><sup>1</sup>, Phillip Leaver<sup>1,2</sup>, Connor Ryan<sup>1,2</sup>, Fiona Tudehope<sup>1,2</sup> and Santosh Sanagapalli<sup>1,2</sup></p><p><sup>1</sup><i>Department of Gastroenterology and Hepatology, St Vincent's Hospital, Sydney, Australia;</i> <sup>2</sup><i>St Vincent’s Clinical School, Faculty of Medicine, University of New South Wales, Sydney, Australia</i></p><p><b><i>Introduction:</i></b> Eosinophilic gastroenteritis is a rare immune-mediated condition defined by the presence of gastrointestinal symptoms alongside the histological demonstration of eosinophilic infiltration in the gastrointestinal tract or eosinophilic ascitic fluid. In this case report, we describe a patient who presented with gastrointestinal symptoms and marked peripheral eosinophilia, who was found to have eosinophilic gastroenteritis with both mucosal and serosal disease involvement<b>.</b></p><p><b><i>Case report:</i></b> A 35-year-old man presented to our institution with a 6-week history of abdominal pain with associated nausea, vomiting and anorexia. He described a history of intermittent episodes of abdominal pain for the past few years prior to presentation. Other past medical history was remarkable for hypertension. Clinical examination was notable for epigastric tenderness. His complete blood count was remarkable for an eosinophil count of 2.6. Computed tomography scan of his abdomen demonstrated features of partial gastric outlet obstruction, a cluster of small nodules about a distal small bowel loop in the upper pelvis and a moderate volume of ascites. Endoscopy demonstrated thickening and erythema of the pylorus with an element of gastric outlet obstruction (Figure 1A); the second part of the duodenum was boggy and thickened (Figure 1B), not allowing deeper passage of the paediatric colonoscope. Alternative causes of eosinophilia were excluded on serological assessment. Biopsies of the duodenal mucosa demonstrated an inflammatory infiltrate of predominantly eosinophils, without dysplasia or malignancy. Ascitic fluid, obtained via ultrasound-guided paracentesis, demonstrated a total white cell count of 1900 x 10<sup>6</sup> cells, of which 91% were eosinophils. Bone marrow aspirate demonstrated a mildly hypercellular aspirate with active trilineage haematopoiesis, with proliferation of left shifted eosinophils averaging 23% of total nucleated cells. There was no evidence of clonality or cytogenic abnormalities detected on this sample. The patient’s eosinophils rose to a peak of 5.2 six days into his admission. He was exquisitely sensitive to intravenous corticosteroids, with a drop of eosinophil count to 0.3 the following day. He was promptly stepped down to oral corticosteroids and discharged on a weaning regimen.</p><p><b><i>Conclusion:</i></b> This was a case of eosinophilic gastroenteritis with serosal and mucosal involvement that responded well to initial corticosteroid therapy. Idiopathic hypereosinophilic syndrome was considered as a differential diagnosis but ultimately ruled out given the absence of multi-system involvement. Long-term treatment options include dietary therapy, immunomodulators and biologics, and disease trajectory remains difficult to predict given the sparsity of cases.</p><p><b>349</b></p><p><b>A retrospect audit of inpatient upper endoscopy for dyspepsia evaluation: Single centre experience</b></p><p><b>Thant Zaw</b><sup>1,2</sup> and Montri Gururatsakul<sup>1,2</sup></p><p><sup>1</sup><i>Cairns Hospital, Cairns, Australia;</i> <sup>2</sup><i>James Cook University, Cairns, Australia</i></p><p><b><i>Background and Aim:</i></b> Dyspepsia is a collection of non-specific upper epigastric discomfort symptoms that often prompt further evaluation through upper endoscopy. However, the role of dyspepsia as an inpatient workup is both practical and can lead to increased hospital stays and inpatient costs. This study was conducted at a regional hospital to assess the outcomes of inpatient endoscopy for patients presenting with dyspepsia.</p><p><b><i>Methods:</i></b> We retrospectively analysed data from inpatients who underwent inpatient endoscopy for dyspepsia at the regional hospital from January 2014 to March 2024. Patient presentation history, endoscopy reports, and biopsy data were gathered from electronic medical records and the endoscopy documentation software (Provation). The primary objective was to determine the cause of dyspepsia, while the secondary goal was to assess the feasibility of conducting these evaluations in outpatient settings.</p><p><b><i>Results:</i></b> A total of 57 upper endoscopy procedures were performed over a 10-year and 2-month period. The patients' ages ranged from 15 to 85, with 54% of the subjects (n=31) being above 50 years old. Alarming features were identified during the analysis, with the most common being persistent vomiting in 20 patients and unintentional weight loss in 15 patients. The predominant findings included gastritis (54.4%), normal findings(15.9%), oesophagitis (8.7%), duodenal ulcer (7%), and gastric ulcer(7%). H. pylori was detected in 3 cases, but no cases revealed any urgent issues requiring immediate attention or malignancy.</p><p><b><i>Conclusion:</i></b> The results indicated that alarming features have a low predictive value for gastrointestinal malignancy. The findings of the audit suggest that endoscopy assessments for new-onset dyspepsia in elderly patients or those with alarming features can be safely conducted in outpatient settings. This approach has the potential to reduce hospital stays and overall hospitalization costs.</p><p><b>358</b></p><p><b>Patient sedation satisfaction for endoscopy procedures comparing anaesthetist assisted endoscopy sedation and endoscopist-directed nurse administered propofol sedation (EDNAPS)</b></p><p><b>Keith Brick</b> and Montri Gururatsakul and Shihaz Hussain and Raymond Lewandowski and Peter Boyd</p><p><i>Queensland Health, Cairns, Australia</i></p><p><b><i>Background and Aim:</i></b> Endoscopist-directed nurse administered propofol sedation (EDNAPS) has been demonstrated to be safe and effective in patients undergoing gastroscopy and colonoscopy procedures. Our regional endoscopy unit utilizes either EDNAPS or anaesthetist assisted endoscopy sedation for such procedures. We aim to investigate patient satisfaction of their sedation at our unit between the anaesthetist assisted endoscopy sedation and EDNAPS.</p><p><b><i>Methods:</i></b> In a single centre study, patients at a regional hospital who underwent simple endoscopic procedures (gastroscopy, colonoscopy, endoscopic dilatation) received sedation from either an anaesthetic team or EDNAPS. Over a three week period (with a plan to extend to 6 months) patients undergoing these procedures were phoned 1-2 weeks after their procedure. They were asked 3 questions related to their satisfaction of the sedation they received. The first two questions were graded on a 5 point Likert Scale: 1. Does the patient remember experiencing pain or discomfort during the procedure; 2. The patients overall satisfaction of sedation. The third question (yes or no) asked if the patient would be willing to have similar sedation for the same procedure in the future. Data collectors were blinded to which type of sedation patients received when contacting the patient. Patient co-morbidities, ASA classification, procedural complications, medication doses, procedural timings and discharge timings were all recorded on a data sheet.</p><p><b><i>Results:</i></b> A total of 98 patients underwent simple endoscopic procedures, and 70 of these patients were able to be contacted by phone regarding their endoscopic procedure (71% phone call response rate). There were 54 patients who received EDNAPS – of this group 9 were ASA 1, 35 were ASA 2 and 10 were ASA 3. In the anaesthetist assisted endoscopy sedation, there were 16 patients – 3 were ASA 2, 8 were ASA 3 and 5 were ASA 4. There were a total of 23 gastroscopies, 34 colonoscopies, 12 combined gastroscopy and colonoscopies, and 1 endoscopic dilatations. Of those who responded who underwent EDNAPS, 53/54 patients (98%) would be willing to have similar sedation for a repeat procedure and 52/54 patients (96%) had no pain with their procedure. In the anaesthetic group 16/16 patients (100%) experienced no pain and would have similar sedation for a repeat procedure. There were no complications reported in any of the procedures in both groups.</p><p><b><i>Conclusion:</i></b> In this audit, the preliminary results showed that patients undergoing simple endoscopic procedures are equally satisfied with EDNAPS compared to anaesthetist assisted endoscopy sedation and there was no difference in complications between the groups. This supports that EDNAPS is both safe and effective for patients given a very high satisfaction rate.</p><p><b>363</b></p><p><b>Bleeding mid-jejunal lesion accessible only with motorised spiral enteroscopy</b></p><p><b>Shane Selvanderan</b>, Robert Little, Catriona McLean, Mark Ward and Gregor Brown</p><p><i>The Alfred Hospital, Melbourne, Australia</i></p><p><b><i>Introduction:</i></b> Small bowel lymphangiomas are benign tumours characterised by dilated lymphatic spaces and account for <1% of all lymphangiomas. They are more common in children and may be complicated by gastrointestinal bleeding, torsion or intussusception.</p><p><b><i>Case report:</i></b> A 26-year-old man of Thai ethnicity presented in 2013 with symptomatic iron deficiency anaemia (IDA) - haemoglobin 51 g/L, ferritin 3 mcg/L and transferrin saturation 7%. Coeliac serology, haemolytic screens, stool microbial testing, esophagogastroduodenoscopy and ileocolonoscopy were unremarkable. Inconsistent clinic engagement precluded timely investigation over the subsequent nine years despite recurrent profound IDA requiring a total of 11 units of packed red blood cells and four iron infusions. Capsule endoscopy identified a mid-jejunal, erythematous, polypoid, plaque-like circumferential lesion. Given epidemiological exposure risk and positive schistosomiasis serology, the patient was treated with two courses of praziquantel and despite this the patient had recurrent iron deficiency anaemia requiring ongoing transfusions. Abdominal CT revealed intra-abdominal lymphadenopathy and differential diagnoses of tuberculosis and small bowel lymphoma were considered. Bidirectional double-balloon enteroscopy was unable to reach the lesion. Surgical referral was offered but the patient opted for a conservative approach with supportive transfusions. A follow-up surveillance capsule endoscopy identified progression of the mid small bowel lesion with fresh bleeding. Expertise and equipment for motorised spiral enteroscopy became available and the haemorrhagic lesion was reached for tissue biopsies via an antegrade approach (Figure 1). Three days post-procedure the patient experienced melaena, increasing abdominal pain, and eventually a complete small bowel obstruction, attributed to biopsy-related haemorrhage. He underwent an exploratory laparotomy with resection of a 65 x 60 mm firm, obstructing mass. Histopathology demonstrated acute haemorrhage and inflammation with deep ectatic vascular channels containing proteinaceous lymphatic material extending from the mucosa to muscularis propria, consistent with a small bowel lymphangioma.</p><p><b><i>Conclusion:</i></b> Mid-jejunal bleeding lesions can pose a diagnostic and therapeutic challenge. Video capsule endoscopy allows for lesion visualisation but not biopsy. Balloon enteroscopy with a view to endoscopic interventions such as biopsy and haemostasis may not achieve the depth of small intubation required for access. Motorised spiral enteroscopy, used in this case, is a technique with impressive rates of pan-enteroscopy but was associated with a risk of unpredictable serious adverse events due to device impaction, and was recalled from the market. There remains a role for small bowel resection, particularly in an isolated small bowel bleeding mass lesion inaccessible via endoscopy.</p><p><b>364</b></p><p><b>Endoscopy-related musculoskeletal pain and injury in endoscopists and endoscopy nurses</b></p><p><b>Oyekoya Ayonrinde</b><sup>1,2,3</sup>, Alan Doyle<sup>1</sup>, Lena Thin<sup>1,2</sup> and Robert Waller<sup>3</sup></p><p><sup>1</sup><i>Fiona Stanley Hospital, Perth, Australia;</i> <sup>2</sup><i>The University of Western Australia, Perth, Australia;</i> <sup>3</sup><i>Curtin University, Perth, Australia</i></p><p><b><i>Background and Aim:</i></b> Musculoskeletal (MSK) pain and injury is increasingly recognised in endoscopists, potentially resulting in time off work or various therapeutic interventions. Consequently, ergonomic training and strategies to reduce injury are encouraged. There is less known about musculoskeletal pain and injury in endoscopy nurses. We examined patterns of MSK pain in endoscopists and endoscopy nurses at a tertiary hospital.</p><p><b><i>Methods:</i></b> In this single centre survey, a questionnaire survey regarding MSK pain at different body sites, was administered to endoscopists and endoscopy nurses. Specific questions related to location, frequency, duration and severity of pain episodes, professional role, gender, and age. We also enquired about glove size, number and type of endoscopic procedures performed per week, personal weight and height, distribution of patient gender and body mass index, and sites of MSK pain. Respondents documented the occurrence of pain relative to endoscopy procedures, a diagnosis of MSK pain or injury syndromes, which professionals had been consulted about the pain, whether they had been taught about ergonomics in endoscopy or would like to be taught, and personal exercise routines.</p><p><b><i>Results:</i></b> Respondents included 31 endoscopists and 14 nurses, and both considered at least 50% of patients attending an endoscopic procedure to be obese. Endoscopist respondents were 68% gastroenterologists, 22% surgeons and 10% gastroenterology registrars, and 77% male. Overall, 70% were aged ≥40 years, 60% had ≥9 years endoscopy experience, and 52% had medium-sized hands and 23% had small hands. Pain lasting ≥ 6 months was reported by 50%, and 17% reported a pain severity of at least 5/10 in the preceding week. The most common site of pain was the left thumb/thumb base. Other common pain sites were the neck, right-sided low back pain, right shoulder, wrist, and elbow (Figure 1). Pain was experienced only when performing endoscopic procedures in 16%, and during and outside endoscopy in 65%. Pain relief remedies were sought from physiotherapists (23%), massage therapist (21%) chiropractor (8%), rheumatologists (5%) or orthopaedic surgeon (5%). A minority (16%) reported having had endoscopy-related ergonomics training, and 81% stated they want more ergonomics information to reduce endoscopy-related injury (Figure 2). Among 14 endoscopy nurse respondents (all female, 50% aged ≥40 years), 50% reported pain lasting over 1 year. 70% had small hands, and reported pain mostly in their back, neck, shoulder or feet, numbness in their hands or feet, or carpal tunnel syndrome (Figure 1). Pain relief remedies were sought mainly from a physiotherapist (24%) or chiropractor (21%), or massage therapist (14%), and 86% knew an endoscopy nurse who had experienced pain severe enough to require time off work, or a therapeutic intervention. Further, 57% worried often or very often that they might experience work-related musculoskeletal injury, and 36% have accordingly considered changing jobs. In contrast to doctors, 36% of nurses say they were taught about ergonomics, and 86% of them want more ergonomics information to reduce endoscopy-related injury (Figure 2).</p><p><b><i>Conclusion:</i></b> Patterns of musculoskeletal pain are different, comparing endoscopists and endoscopy nurses. Despite musculoskeletal pain being common in endoscopists and endoscopy nurses, and impacting their well-being, the majority have not had ergonomic training but would like more information on how to avoid injury. Ergonomic training and injury prevention strategies are critical to maintaining the endoscopy workforce.</p><p><b>383</b></p><p><b>Iron deficiency without anaemia; any clinically significant outcomes on combined gastroscopy and colonoscopy?</b></p><p><b>Aidan Taylor</b> and Montri Gururatsakul</p><p><i>Cairns and Hinterland Hospital and Health Service, Cairns, Australia</i></p><p><b><i>Background and Aim:</i></b> Iron deficiency anaemia remains a strong indication for combined gastroscopy and colonoscopy to exclude chronic gastrointestinal blood loss, especially malignancy. However, the utility of combined gastroscopy and colonoscopy remains unclear in patients with iron deficiency without anaemia and the aim of the study is to assess for any clinically significant outcomes in these patients.</p><p><b><i>Methods:</i></b> This is a retrospective study, data from patients referred to Endoscopy Unit with iron deficiency without anaemia (Serum ferritin < 20g/L, normal haemoglobin) between 2018 to 2023 were analysed. Patients were assessed for endoscopic evidence of cause for iron deficiency without anaemia compared with age, sex, and presence of alarm symptoms at time of referral.</p><p><b><i>Results:</i></b> 132 patients (65% female, mean age 54.17): 42.4% were aged <50 years, 36.4% were 50 – 69 years, and 21.2% were >70 years old, received endoscopic evaluation for iron deficiency without anaemia. Of those 132 patients, 91% received both gastroscopy and colonoscopy, 4.5% received upper endoscopy alone and 4.5% colonoscopy only. The significant outcomes of interest were divided into minor findings (H pylori gastritis, angioectasia, autoimmune atrophic gastritis and ulcers) and major findings (malignancy, polyps >20mm and adenomas with high grade dysplasias). Of those 132 patients, total of 24 patients referred with iron deficiency without anaemia were found to have abnormal endoscopic findings; 3.8% (n = 5) had major findings and 16% (n=21) had minor findings. 36% (n=48) of patients had alarm symptoms (Dysphagia, odynophagia, weight loss, haematemesis, rectal bleeding) or faecal occult blood test positive at time of referral. Of those referred with alarm symptoms 17% (n = 8) had minor endoscopic findings and 8.3% (n = 4) had major findings. Compared to those who did not have alarm symptoms, 15% (n = 13) had minor findings and 1.2% (n = 1) had major findings. H pylori gastritis was the most common minor finding with 11 cases (55% of cases occurring in patients <50 years of age [n = 6]). There were 7 patients with non-bleeding angioectasia, (57% [n = 4] occurring in patients >70 years of age). 1 patient had autoimmune atrophic gastritis. No patient was found to have gastric or duodenal ulcers. There were 5 major findings, 3 patients had polyps >20mm (tubular adenoma with low grade dysplasia), 1 patient had adenocarcinoma and 1 patient tubular adenoma with high grade dysplasia. Of the major findings 1 was <50 years old and 4 were >50 years of age.</p><p><b><i>Conclusion:</i></b> Overall, the data shows that H pylori gastritis is a common cause for iron deficiency without anaemia in those <50 and reinforces the need to look for malignancy in those aged >50. Patients referred with iron deficiency without anaemia who had alarm symptoms were almost 7 times more likely to have major findings compared to those who did not.</p><p><b>385</b></p><p><b>A rare case of nivolumab induced oesophagitis 4 years after commencement of therapy</b></p><p><b>Aidan Taylor</b> and Montri Gururatsakul</p><p><i>Cairns and Hinterland Hospital and Health Service, Cairns, Australia</i></p><p><b><i>Introduction:</i></b> Nivolumab, an immune check-point inhibitor, is a class of immunotherapy currently approved in Australia for the treatment of various locally advanced and metastatic cancers. Although Nivolumab is an effective treatment option for cancer, this class of medication is associated with immune-related adverse events, including immune mediated colitis, and immune mediated hepatitis are well documented in the literature. However, reports of upper-gastro-intestinal adverse events such as oesophagitis remains rare. This is a case report of a patient who developed Nivolumab induced oesophagitis.</p><p><b><i>Case report:</i></b> A 60-year-old female presented with dysphagia and odynophagia for 4 weeks, her past medical history included metastatic melanoma treated with Nivolumab in the last 4 years. Subsequently, upper endoscopy showed oesophagitis and oesophageal ulceration at the lower oesophagus, which was biopsied. Histopathology demonstrated active chronic inflammation, apoptotic keratinocytes, and reactive changes. In the absence of infection, clinicopathological correlation with nivolumab therapy raised suspicion of nivolumab associated oesophagitis. This is a rare case of Nivolumab associated oesophagitis 4 years after its commencement. Due to the rarity of nivolumab induced oesophagitis, management remains largely non-specific with proton pump inhibitors and oral steroid therapy, with severe cases resulting in cessation of treatment. Fortunately, her symptoms improved with proton pump inhibitors and prednisolone, therefore she was able to continue Nivolumab, with a plan to repeat upper endoscopy soon.</p><p><b>403</b></p><p><b>Systematic review and meta-analysis of the correlation between upper gastrointestinal mucosal thickening on CT and the endoscopic findings</b></p><p><b>Hydar El Jamaly</b><sup>1</sup>, Osamah Al-Obaidi<sup>2</sup>, Noureddin Al-Hajjiri<sup>1</sup> and Mouhannad Jaber<sup>1</sup></p><p><sup>1</sup><i>Wollongong Hospital, Wollongong, Australia;</i> <sup>2</sup><i>Concord Hospital, Concord, Australia</i></p><p><b><i>Background and Aim:</i></b> Upper gastrointestinal (UGI) mural thickening (MT) is often reported on standard CT examinations of the abdomen. It often presents a dilemma for the clinician on whether any further evaluation is needed, especially in the absence of any set guidelines. To evaluate the significance of UGI MT and to assess its correlation with upper Endoscopy.</p><p><b><i>Methods:</i></b> We conducted a comprehensive literature search using a strategy in Medline and this was extended to PubMed and Embase. The studies included patients with UGI MT on CT scans, who underwent endoscopic evaluation. We used a random-effects model using pooled positive predictive value (PPV) with 95% confidence intervals (CI). MT was defined as 5mm or above in the Oesophagus and Stomach, and 3mm or above in the duodenum.</p><p><b><i>Results:</i></b> A total of 11 cohort studies examining 855 patients were selected having undergone both CT and upper Endoscopy. Of the 855 patients with MT, 753 had an abnormal upper Endoscopy. In the presence of MT, the pooled PPV for malignancy was 0.21 (95% CI: 0.11-0.36), 0.35 (95% CI: 0.23-0.50) and 0.28 (95% CI: 0.06-0.69) for the Oesophagus, stomach and duodenum respectively (Figure 1). In the presence of MT, the pooled positive predictive value (PPV) for all pathology at upper Endoscopy was 0.84 (95% CI: 0.72-0.91), 0.86 (95% CI: 0.72-0.94) and 0.50 (95% CI: 0.20-0.80) for the Oesophagus, stomach and duodenum respectively (Figure 1).</p><p><b><i>Conclusion:</i></b> Gastrointestinal Mural thickening (MT) detected on CT scans has a high positive predictive value of finding abnormalities during an upper endoscopy, including potential malignancies. Additional endoscopic confirmation is warranted upon identifying MT on CT examinations. More data with larger sample sizes that accurately define MT and other associated radiological findings are needed.</p><p><b>409</b></p><p><b>Long-term outcomes of patients undergoing capsule endoscopy in the investigation of suspected small bowel bleeding</b></p><p><b>Isaiah Tambyrajah</b><sup>1,2</sup> and <b>Robert B Feller</b><sup>1,2</sup></p><p><sup>1</sup><i>Department of Gastroenterology & Hepatology, St Vincent's Hospital, Sydney, Australia;</i> <sup>2</sup><i>Faculty of Medicine and Health, University of New South Wales, Sydney, Australia</i></p><p><b><i>Background and Aim:</i></b> The long-term outcomes (greater than five years) of patients undergoing small bowel capsule endoscopy (SBCE) for suspected small bowel bleeding (SSBB) remain unclear. This study sought to determine the long-term rebleeding rate and predictive factors for rebleeding in patients investigated for SSBB.</p><p><b><i>Methods:</i></b> This single-centre, retrospective cohort study followed up patients (n = 64) who underwent SBCE between March 2015 and December 2017 at a tertiary hospital in Sydney, Australia by utilising medical records and phone consultations. The Cox proportional hazards model was utilised to evaluate predictive factors of rebleeding, and Kaplan-Meier survival curves to analyse cumulative rebleeding rates.</p><p><b><i>Results:</i></b> Sixty-four patients were included in the analysis. The cumulative rebleeding rate in patients with SSBB was 49.1% (28/57) over a mean follow-up of 81.8 ± 10.3 months. Multivariate analysis using the Cox proportional hazards model revealed that an initial haemoglobin (Hb) less than 100 g/L (hazard ratio [HR] 3.615, 95% confidence interval [CI] 1.454-8.989, p = 0.006), positive SBCE study (HR 22.452, 95% CI 1.312-384.336, p = 0.032) and chronic kidney disease (HR 14.611, 95% CI 1.143-186.838, p = 0.039) were predictors of rebleeding. The rebleeding rate amongst patients with a negative SBCE study was 16.7%.</p><p><b><i>Conclusion:</i></b> Rebleeding is common during the long-term follow-up of patients assessed for SSBB. Negative SBCE is not a definitive predictor of event-free survival. Diligent follow-up is necessary, especially for patients presenting with low initial Hb and positive SBCE findings. Patients presenting with iron deficiency without significant anaemia should undergo a period of iron supplementation before SBCE.</p><p><b>433</b></p><p><b>Safe and effective endoscopic mucosal resection of large premalignant colorectal polyps in a regional centre</b></p><p><b>Daniel Yee Lee Ng</b><sup>1</sup>, Yoland Hsia<sup>2</sup>, Aqsa Farooq<sup>2</sup>, Tania Chapman<sup>1</sup>, Daniel Saitta<sup>1</sup>, Sajith Kattiparambil Gangadharan<sup>1</sup>, Jong Chin<sup>1</sup>, Maree Pekin<sup>1</sup>, Timothy Elliott<sup>1</sup> and Dileep Mangira<sup>1</sup></p><p><sup>1</sup><i>Grampians Health, Ballarat, Australia;</i> <sup>2</sup><i>Deakin University, Ballarat, Australia</i></p><p><b><i>Background and Aim:</i></b> Endoscopic Mucosal Resection (EMR) is the current standard of management for large premalignant colonic polyps. EMR is typically performed at tertiary centres because of the required advanced endoscopic skills and need for adequate surgical support. Patients in regional and remote areas have a higher incidence of, and worse prognosis from, colorectal cancer, when compared with metropolitan patients. They often do not gain access to optimal care because of their remote geographical location. We developed a regional centre colorectal EMR service to improve access to these services for patients from regional and remote areas. The aim of this study was to assess the safety and efficacy of a regional colorectal EMR service.</p><p><b><i>Methods:</i></b> Data were retrospectively obtained via diagnostic coding for colonoscopy with polypectomy on ENDOBASE at a single regional centre between January 2021 and December 2022 for two experienced endoscopists with tertiary centre EMR training. Medical file review identified EMRs by confirming the performance of a submucosal lift prior polypectomy. We collected data relating to the patient (demographic details), the polyp (site, size, Paris, Kudo classification and histology), the EMR procedure (use of hot/cold snares, piecemeal/en bloc resections and complications) and 1st surveillance colonoscopy (timing and presence/size of polyp recurrence). Polyps ≤10mm were excluded.</p><p><b><i>Results:</i></b> 189 colonoscopies with polypectomy were identified during the study period. Medical file review identified 84 patients (mean age 65 +/- 12.3 years) who underwent EMR for polyps > 10mm. In 2 of these patients, EMR was abandoned because of suspected cancer (n=1) (confirmed histologically) and poor elevation (n=1) (technical success: 82/84=98%). A total of 103 lesions were resected (1 patient with 4 lesions, 1 patient with 3 lesions, 14 patients 2 lesions, 68 patients with 1 lesion). Mean polyp size was 23mm +/- 10mm. Paris classification was as follows: 0-IIa (58/103), 0-Is (12/103), 0-Ip (4/103), 0-IIa/Is (4/103), 0-Isp (1/103), others (24/103). Kudo pit pattern was as follows: II (31/103), IV (27/103), III L (10/103), III S (9/103), III (7/103), unspecified (19/103). Histopathology of EMR resected polyps was as follows: tubulovillous adenomas (TVA) (45/103), sessile serrated lesions (SSL) (40/103), tubular adenomas (TA) (16/103), and others (2/103). 14/103 lesions had high-grade dysplasia. No cancer was identified. Procedural complications were identified in 4 patients (4/93=4.3%). There were 2 episodes of per rectal bleeding (2/93=2.15%) - one requiring intervention with endoclips. There were 3 episodes of self-resolving abdominal pain (3/93=3.2%) (1 patient with both per rectal bleeding and abdominal pain). There were no perforations. To date, 55/84 patients who underwent EMR have had a first surveillance colonoscopy at a median interval of 11 months. 52/55 patients had no polyp recurrence and there were no interval cancers identified. Of the 3/55 (5.5%) with polyp recurrence, all were easily resected with a cold snare.</p><p><b><i>Conclusion:</i></b> EMR of large premalignant colonic polyps can be performed safely and effectively in a regional centre. This helps address the well-documented inequity of care delivery for patients from regional and remote areas with precancerous polyps.</p><p><b>434</b></p><p><b>White patch with malignant potential: incidental finding of oesophageal leukoplakia at oesophagogastroduodenoscopy</b></p><p><b>Christopher James Shephard</b> and Bulent Baran</p><p><i>Department of Gastroenterology and Hepatology, Townsville University Hospital, Townsville, Australia</i></p><p><b><i>Introduction:</i></b> Oesophageal leukoplakia, also known as oesophageal epidermoid metaplasia, is a rarely encountered and likely under-recognized entity in endoscopic practice, with an estimated prevalence of 0.19%. Akin to the oral form, it is associated with tobacco and alcohol exposure, although chronic oesophageal irritation from acid reflux is also postulated. It is associated with progression to oesophageal squamous cell dysplasia and squamous cell carcinoma (SCC), although the natural history is less well-described than its oral counterpart. Presentation may be incidental/asymptomatic, or otherwise with dysphagia/odynophagia or globus sensation. It typically manifests in the mid-oesophagus as a translucent white well-demarcated metaplastic patch/plaque. Characteristic histological findings include hyperorthokeratosis, hypergranulosis and epithelial metaplasia. Detection may pose management dilemmas in the absence of recognised guidelines for surveillance and treatment. This case report serves to improve awareness of this rare, yet clinically significant pre-malignant oesophageal lesion.</p><p><b><i>Case report:</i></b> A 55-year-old man with a history of long-term alcohol abuse, tobacco smoking, GORD with Barrett’s metaplasia and hypovitaminosis D was referred for an opinion on newly detected liver cirrhosis on ultrasound. Oesophagogastroduodenoscopy (OGD) three years prior demonstrated LA grade A reflux oesophagitis at the gastro-oesophageal junction, short-segment Barrett’s metaplasia C1-M2 in the distal third of the oesophagus and an absence of oesophageal varices. He denied dysphagia or weight loss but did report intermittent bowel habit with melaena in recent months without an associated anaemia. He was non-compliant with previously prescribed proton-pump inhibitor (PPI) therapy. He proceeded to OGD for varices screening, Barrett’s surveillance and evaluation of suspected upper gastro-intestinal bleeding. Examination findings were pertinent for LA grade C reflux oesophagitis and short-segment Barrett’s metaplasia (consistent with previous) without varices, plus the interval finding of a suspicious fixed, white granular-appearing patch of mucosa in the mid-oesophagus concerning for leukoplakia which was biopsied (figure 1A). Distal examination revealed erosive gastropathy and a Forrest IIc duodenal ulcer. The patient was recommended high-dose PPI therapy and eight-week follow-up endoscopy. Histopathology of the suspicious oesophageal lesion proved consistent with oesophageal leukoplakia, demonstrating prominent hyperkeratosis and glandular metaplasia without dysplasia/neoplasia (figure 1B). Subsequent OGD examination revealed stable leukoplakia (figure 1C) with resolving oesophagitis and duodenal ulceration. A plan for close endoscopic follow-up, as opposed to endoscopic ablation/resection, was enacted considering the patient’s other strong indications for repeat OGD examinations.</p><p><b><i>Conclusion:</i></b> Oesophageal leukoplakia is a rare yet easily recognisable endoscopic entity that may progress to dysplasia and SCC. In the absence of standardised treatment guidelines, clinician discretion regarding either close follow-up or early endoscopic therapy is advised in view of the neoplastic potential. Improved understanding of the natural is necessary to inform best practice management.</p><p><b>435</b></p><p><b>Evaluation of the safety and quality of operator delivered conscious sedation colonoscopy by nurse practitioner endoscopists</b></p><p><b>Grace Magnani</b>, Kylie Ashley and John Masson</p><p><i>Townsville University Hospital, Townsville, Australia</i></p><p><b><i>Background and Aim:</i></b> Sedation models for colonoscopy vary from conscious sedation provided by the proceduralist, to deep sedation provided by an anaesthetist. In 2018 two Nurse Practitioner Endoscopists (NPE) in a regional hospital were formally trained and successfully credentialed by their health service to perform colonoscopy procedures and concurrently administer conscious procedural sedation using intravenous fentanyl and midazolam for low risk patients (American Society of Anaestheologists ASA 1-2). The NPE model complements the existing medical endoscopy service that routinely uses conscious procedural sedation to perform colonoscopy procedures. A hospital procedure outlining a clear NPE scope of practice was developed guided by the Australian and New Zealand College of Anaesthetics (ANZCA) PG09(G) Guideline on procedural sedation 2023 (formerly PS09, 2014). The aim of this evaluation is to demonstrate within a large cohort of patients that the NPE as operator sedationist is safe and able to complete routine high quality colonoscopy procedures on low risk patients. We believe this is the first health service in Australia where NPE were credentialed as operator sedationists.</p><p><b><i>Methods:</i></b> A retrospective audit using prospectively collected demographic and clinical data. Data was obtained from Endoscopy Services Information System Solution (ESSIS) Provation® MD database and the integrated electronic Medical Record (iEMR) between June 2018 and December 2023. Project approval was through the Hospital and Health Service Audit, Quality and Innovation Review Panel.</p><p><b><i>Results:</i></b> Between June 2018 to December 2023, 4419 patients had colonoscopy with the NPE. Total of 4339 (98%) patients having colonoscopy were sedated by the NPE as operator sedationist. Overall caecal intubation rate (CIR) 98%, mean age 57 (range 18-83 years), 45% female. Pre-anaesthesia risk ASA 1 (healthy) 1221 (28%), ASA 2 (mild systemic disease) 3007 (68%), ASA 3 (severe systemic disease) 192 (4%). ASA 3 cases were discussed with a senior consultant prior to sedation administration. Overall total (all ages, including non intact, excluding IBD) adenoma detection rate (ADR) 53%, Sessile Serrated Lesion (SSL) detection rate 15%. Of the cohort of patients > 50 (2884), CIR 98%, ADR 62%, SSL 14%.</p><p>Overall mean total sedation dose, (range) fentanyl 106mcg (50-200mcg), midazolam 3.5mg (0.5-7mg). Doses titrated over fentanyl 150mcg and midazolam 5mg were discussed with a consultant prior to administering. Fifteen non serious complications (Table 1). No patients required reversal agents or Medical Emergency Team (MET) calls. Of 77 patients having unsedated colonoscopy, the ileum/caecum were intubated in 72 (94%), 4 (4.7%) aborted due to intolerance, 1 (1.3%) incomplete due to obstructing mass. Three (0.06%) patients had colonoscopy with sedation augmented by medical staff due to significant co-morbidites/high risk.</p><p><b><i>Conclusion:</i></b> NPE operator sedationist procedures delivers safe, quality colonoscopy procedures. NPE as operator sedationist for colonoscopy procedures using fentanyl and midazolam is a viable and safe option to access routine, low risk colonoscopy. Cost analysis and patient satisfaction studies are currently underway.</p><p><b>438</b></p><p><b>Quality and safety of colonoscopy delivered by nurse practitioner endoscopists in a regional hospital in Queensland – a service evaluation</b></p><p><b>Kylie Ashley</b>, Grace Magnani and John Masson</p><p><i>Townsville University Hospital, Townsville, Australia</i></p><p><b><i>Background and Aim:</i></b> In Australia the demand on colonoscopy services continues to increase driven by the National Bowel Cancer Screening Program (NBCSP) and consequent polyp surveillance. During the same period there has also been increased focus by both providers and patients on the quality and safety of colonoscopy services. This led to the development and implementation of evidence based, measurable key performance indicators (KPI). In 2018 two Nurse Practitioner Endoscopists (NPE) were credentialed by Queensland Health to deliver conscious procedural sedation colonoscopy as operator sedationist within a regional Queensland public hospital. The aim of this study is to evaluate the quality and safety of the NPE service.</p><p><b><i>Methods:</i></b> Retrospective audit of prospectively collected demographic and clinical data obtained from Endoscopy Services Information System Solution (ESSIS) ProVation® MD database and integrated electronic Medical Record (ieMR) between June 2018 and December 2023. Data relating to specific KPIs presented in the National Colonoscopy Clinical Care Standard 2020 (Australian Commission of Safety and Quality in Health Care) were collected. The 30 day hospital readmissions, complications and mortality were independently reviewed. Project approval was through the Hospital and Health Service Audit, Quality and Innovation Review Panel.</p><p><b><i>Results:</i></b> We report the first 5.5 years of the NPE service. Total 4419 patients underwent colonoscopy with operator delivered conscious sedation representing approximately 40% of colonoscopy performed in the unit. Mean age 57 (range 18-83 years), females 45%. ASA 1 1221 (28%), ASA 2 3007 (68%), ASA 3 192 (4%). Overall caecal intubation rate 4210 (98%). Procedures not completed to caecum or requiring a further follow up procedure are listed (Table 1). Patients >50 years, intact colons and excluding inflammatory bowel disease (IBD) (2884), adenoma detection rate 62% (1795), sessile serrated lesion rate 14% (409), adenocarcinoma 2% (51). Fifteen recorded immediate complications (Table 2), resulting in one overnight admission for observation after control of a polypectomy related bleed. Six hospital re-presentations for procedure related or possibly related events within 30 days post colonoscopy, all were considered minor events. One 30 day mortality was due to a CVA in a known arteriopath presenting at day 28 post colonoscopy. On review this was judged not to be procedure related.</p><p><b><i>Conclusion:</i></b> NPE can deliver safe, high-quality colonoscopy. The findings of this evaluation support the vision for expanding NPE services to help meet the demand for safe, effective colonoscopy.</p><p><b>442</b></p><p><b>EXPLORE AI-BO Study: Exploring endoscopists’ knowledge, perception and attitude towards artificial intelligence in endoscopic surveillance for Barrett’s oesophagus</b></p><p><b>Nicholas Wan</b><sup>1,2</sup>, Jin Lin Tan<sup>1,2</sup>, Celine Chan<sup>1</sup>, Mohamed Asif Chinnaratha<sup>1,2</sup> and Rajvinder Singh<sup>1,2</sup></p><p><sup>1</sup><i>Gastroenterology Department, Lyell McEwin Hospital, Adelaide, Australia;</i> <sup>2</sup><i>Adelaide Medical School, University of Adelaide, Adelaide, Australia</i></p><p><b><i>Background and Aim:</i></b> Artificial Intelligence (AI) has been shown to assist endoscopists in detecting early neoplasia in Barrett’s oesophagus (BO). This questionnaire aims to explore endoscopists’ knowledge, perception, and attitude towards AI in BO, providing insights into factors impacting the translation of such models into clinical practice.</p><p><b><i>Methods:</i></b> An online questionnaire was developed and disseminated to one hundred and forty endoscopists across South Australia. Descriptive statistics were used to summarise the results.</p><p><b><i>Results:</i></b> Twenty participants completed the questionnaire, including gastroenterologists (50%), surgeons (30%), and trainees (20%). Overall, participants exhibited positive attitudes on the validated Artificial Intelligence Attitude Scale (AIAS-4), with a mean score of 17.5 (SD = 2.3) out of 20. <b>Domain 1 – Knowledge and Perception Towards AI in Endoscopy:</b> 15% of respondents reported having adequate knowledge of AI application in BO. This compared unfavourably to colorectal polyp detection (60%). However, 85% of participants were willing to use AI for BO surveillance. <b>Domain 2 – Knowledge and Perception Towards AI in BO-Surveillance:</b> White-Light-Imaging (60%) and Narrow-Band-Imaging (55%) were the top two imaging modalities where respondents had some knowledge of AI applications in BO-surveillance. All respondents preferred AI models capable of supporting multiple-imaging modalities. Participants perceived that AI will improve the detection rates of low-grade dysplasia (90%), high-grade dysplasia (95%) and early oesophageal cancer (85%). <b>Domain 3 – Impact on Patients:</b> 50% of respondents anticipated that AI would reduce the frequency of endoscopic surveillance. 60% of respondents indicated that using AI would improve therapeutic relationships with patients. <b>Domain 4 – Impact on Endoscopists:</b> Respondents indicated that AI could extend the duration of procedures (75%). While some suggested an increase in fatigue (25%), others believed it decreases fatigue (50%). <b>Domain 5 – Impact on Clinical Practice:</b> All respondents expressed confidence that AI would enhance their accuracy in dysplasia detection. 70% of respondents indicated their preference to perform random oesophageal biopsies even if AI has >95% sensitivity for detecting early Barrett’s dysplasia. <b>Domain 6 – Medico-legal Concerns:</b> Without clear regulation, only 50% of respondents are open to using AI in endoscopy. Accountability of missed lesions was felt to be the responsibility of endoscopists (70%) rather than AI (5%).</p><p><b><i>Conclusion:</i></b> Endoscopists showed positive attitudes towards integrating AI in BO-surveillance, especially regarding the perceived improvement in detecting early dysplasia. This questionnaire highlights concerns including liability, procedural duration, and its lack of clear regulation.</p><p><b>454</b></p><p><b>Implementation and evaluation of unsedated transnasal endoscopy: an efficient solution for increasing demand for upper gastrointestinal endoscopy?</b></p><p><b>Lea Wiggins</b><sup>1</sup>, Rhian Jones<sup>2</sup>, Angela Carberry<sup>2</sup> and James O'Beirne<sup>1</sup></p><p><sup>1</sup><i>Sunshine Coast University Hospital, Birtinya, Australia;</i> <sup>2</sup><i>Sunshine Coast Health Institute, Birtinya, Australia</i></p><p><b><i>Background and Aim:</i></b> The demand for procedures such as upper gastrointestinal endoscopy is increasing, driven by population growth, higher rates of chronic disease, an ageing population, with the rate of individuals over 70 years in our health district being 40% higher than the Queensland average. Traditionally, upper gastrointestinal endoscopy procedures at our health service have relied heavily on anaesthetists for procedural sedation. However, alternative models such as Unsedated TransNasal Endoscopy (UTNE) offer a potential solution to reduce reliance on anaesthetists and ancillary staff, improve patient flow, shorten waitlists and increase patient convenience. UTNE uses an ultrathin endoscope inserted through the nasal passage following topical anaesthesia, avoiding the need for sedation and reducing the number of procedural healthcare professionals required. Recent technological advancements have improved the utility and image quality of transnasal endoscopes, making UTNE a viable alternative to traditional methods.</p><p><b><i>Methods:</i></b> A mixed-method evaluation approach was used, combining quantitative and qualitative data. Procedural data was collected from hospital electronic medical records and surveys were disseminated to collect patient and clinician experience measures.</p><p><b><i>Results:</i></b> Forty-seven UTNE procedures were completed, with a median procedure time of 6.7 minutes (SD ± 2.8 minutes). In all cases Olympus XP190N gastroscopes (5.4mm outer diameter) were used. The oldest pt was 91 and youngest 24 years of age. The mean age of patients was 55 years (SD ± 15.8 years), with more female patients (n=25) than male patients (n=22). In three cases the procedure was converted to an oral approach due to unfavourable nasal anatomy. Indications for endoscopy were, evaluation of reflux symptoms (39%), dysphagia (23%), eosinophilic oesophgitis (9%), Barretts oesophagus (4%) and others (25%). No procedural complications, emergency department presentations within 72 hours post-procedure, or mortalities were reported. Clinical records indicated no adverse outcomes related to the UTNE procedures. Patient satisfaction was generally high, with positive feedback highlighting personalised care and professional, caring staff. However, some patients expressed uncertainty regarding biopsy outcomes and the communication of results. Specific survey results indicated that all respondents (n=7, 7% response rate) rated the overall care received as very good, appreciated the clear communication from healthcare professionals, and felt involved in decision-making about their care. Most patients felt they had the procedure as soon as necessary (86%), received adequate information to prepare (71%), had the opportunity to ask questions (86%), were informed about post-procedure expectations (80%), and did not experience long waits at the clinic (71%). Half of the patients (50%) experienced some discomfort during the procedure, although this was reported as being less or much less than expected. Majority of patients reported that they did not take any time off work to attend the procedure (60%), and all patients reported that they did not require another person to take time of work to support them to attend their endoscopy appointment.</p><p><b><i>Conclusion:</i></b> The UTNE model demonstrated safety and high patient satisfaction, reducing the need for sedation and the number of healthcare professionals involved in upper gastrointestinal procedures. Despite the positive outcomes, challenges such as data accuracy and communication of biopsy results need to be addressed to improve the model’s effectiveness and scalability. Further training of proceduralists and enhancements in data management are recommended to support the broader implementation of UTNE. Addressing these challenges will ensure more efficient and effective patient care, ultimately contributing to the sustainability of healthcare services in the face of rising demand and workforce shortages.</p><p><b>457</b></p><p><b>Adherence to therapeutic gastroscopy guidelines for acute esophageal food bolus impaction: impact on adverse outcomes and length of stay</b></p><p><b>Fei Yang Pan</b><sup>1</sup>, Tuan Anh Duong<sup>2</sup>, Kimberley Davis<sup>2</sup>, Claudia Rogge<sup>2</sup> and Matthew Smale<sup>3</sup></p><p><sup>1</sup><i>Macquarie University Hospital, Sydney, Australia;</i> <sup>2</sup><i>Wollongong Hospital, Wollongong, Australia;</i> <sup>3</sup><i>Liverpool Hospital, Sydney, Australia</i></p><p><b><i>Background and Aim:</i></b> According to the European Society of Gastrointestinal Endoscopy (ESGE), gastroscopy should be conducted within 6 hours for complete obstruction and 24 hours for incomplete obstruction due to food bolus impaction. This study explores whether adults with acute esophageal food bolus (FB) impaction experience adverse outcomes when their time to esophagogastroduodenoscopy (EGD) deviates from the recommended guidelines.</p><p><b><i>Methods:</i></b> A retrospective review was performed on the records of 248 patients who presented at the study site between 2015 and 2022 with symptoms of FB impaction. Local endoscopy software was used to identify patients meeting the inclusion criteria and data was extracted from the patients’ electronic medical records. Age, sex, timestamps (patient reported FB ingestion, ED presentation, EGD and discharge), type of FB, glucagon usage, evidence of complete obstruction (defined as an inability to swallow saliva), biopsy status and results, endoscopic technique, and complications were collated. Time between ingestion and ED presentation, ED presentation and EGD, EGD and discharge and overall length of stay (LOS) were calculated. Complications were categorized into grades with aspiration as a separate category. Statistical analysis was conducted using RStudio V4.1.</p><p><b><i>Results:</i></b> 248 patients underwent EGD for FB impaction. Grade 1 (erosion, ulceration), grade 2 (tear) and grade 3 (perforation) complications were present in 31.6%, 6.9% and 0.8% of cases, respectively. Of the 134 (54.0%) patients with complete obstruction, 51 (38.1%) received EGD within the recommended 6 hours. Whilst of the 114 (46%) patients with incomplete obstructions, 93 (81.6%) received EGD within the recommended 24 hours. There was no statistically significant correlation between LOS post-EGD and any of ingestion to presentation time, presentation to EGD time or ingestion to EGD time. Age and complication level were greater predictors of longer LOS than presentation to EGD time. Patients who presented in hours were significantly more likely to receive EGD within the 6- and 24-hour guidelines than those that presented out of hours (50.7% versus 22.0%).</p><p><b><i>Conclusion:</i></b> Further prospective, multi-center studies may evoke a revision of the current ESGE guidelines on time to EGD for FB impaction. While the importance of prompt therapeutic EGD is necessary for patient comfort, our study did not illustrate a reduced complication rate, complication grade or post-EGD LOS by doing so. Continued research is needed to optimize patient care and outcomes in cases of FB impaction.</p><p><b>465</b></p><p><b>Pop, drop and pull: A case report of acute gastric outlet obstruction secondary to bariatric intragastric balloon requiring endoscopic removal</b></p><p><b>Ayrton Sheehan</b> and Rohit Gupta</p><p><i>Sunshine Coast University Hospital, Birtinya, Australia</i></p><p><b><i>Introduction:</i></b> Bariatric intragastric balloons have emerged in clinical practice for obesity management as a primary strategy for weight loss, or as a bridge to bariatric surgery. Intragastric balloons are inserted endoscopically, or with radiological guidance, under the direction of a bariatric weight loss surgeon or clinic. We present a case of acute gastric outlet obstruction secondary to bariatric intragastric balloon to raise awareness of this complication, and to describe the endoscopic management for the on-call gastroenterologist.</p><p><b><i>Case report:</i></b> A 33 year old female presented to hospital with a two day history of escalating epigastric abdominal pain with associated nausea, vomiting and severe regurgitation. Three days prior, the patient had a radiologically placed intragastric inflatable balloon as a weight loss strategy for obesity. Her current weight was 95kg. She had a previous bariatric intragastric balloon resulting in 15kg weight loss over a 4 month period. There were no symptoms associated with the previous intragastric balloon, and it self-deflated after 16 weeks and was spontaneously passed rectally. On clinical examination, the abdomen was soft and non-tender to palpation. Biochemical testing demonstrated a raised serum creatinine at 87 μmol/L and a normal lipase at 33 unit/L. Evaluation with computed tomography abdominal imaging demonstrated a fluid filled intragastric balloon measuring 12cm x 9cm x 10cm with estimated volume of 540ml. There was no imaging evidence of pancreatitis or perforation. Endoscopic assessment revealed retained gastric contents related to gastric outlet obstruction secondary to the intragastric balloon (see Figure 1). The gastric contents were suctioned, and a needle was passed through the gastroscope and inserted into the intragastric balloon for deflation with a combination of manual and wall suction of the balloon’s contents. Following deflation, the balloon’s edge was grasped with a snare and removed.</p><p><b><i>Conclusion:</i></b> Intragastric balloons are becoming more prevalent as a management strategy for obesity. Gastroenterologists are likely to encounter complications of bariatric intragastric balloons more frequently in clinical practice into the future. Understanding the possible complications and their management is important for future care of these patients.</p><p><b>476</b></p><p><b>Over the scope clip as first or second-line endoscopic therapy in acute non-variceal upper gastrointestinal bleeding</b></p><p><b>Khaliun Batkhurel</b>, <b>Mohammad Shir Ali</b>, <b>Lay Theng Gan</b>, <b>Mark Loewenthal</b>, <b>Randy Tjang</b>, <b>Donna Gilles</b> and <b>Steven Bollipo</b></p><p><i>Department of Gastroenterology, John Hunter Hospital, Newcastle, Australia</i></p><p><b><i>Background and Aim:</i></b> The over the scope clip (OTSC) can potentially overcome limitations of standard clips and achieve reliable haemostasis. This is due to its ability to achieve larger mucosal approximation and capture deeper tissue layers. Recent studies have shown that OTSC is effective in achieving hemostasis for refractory upper GI bleeding. The aim of this study is to evaluate outcomes of OTSC as first and second line therapy for management of acute NVUGIB at our institution.</p><p><b><i>Methods:</i></b> We prospectively and retrospectively collected and analysed our database from January 2019 to May 2024 from all patients who underwent emergency gastroscopy for NVGIB. The patients’ clinical demographics were obtained from patient records. We also looked at patients’ comorbidities, including their use of anticoagulation and antiplatelet agents.</p><p><b><i>Results:</i></b> 52 patients underwent a gastroscopy with OTSC insertion as either first line (n=42) or second line (n=10) endoscopic treatment. Culprit lesions were in the antrum (n=8), gastric body (n=2), first part of duodenum (n=37), and second part of duodenum (n=7). Successful haemostasis at endoscopy was achieved in 44/52 (84.6%). OTSC as first-line therapy had a primary success rate of 37/42 (88%) while as second-line therapy the success rate was 7/10 (70%). Rebleeding after successful endoscopic haemostasis occurred in 6/52 patients (Table 1). In total, 11/52 (21%) patients failed endoscopic treatment and progressed to surgical management (n=5) or interventional radiology (IR) intervention (n=6). We found that of patients who rebled after OTSC, there is a clear leader in NSAID being the primary cause. Technical issues with deployment of OTSC occurred in three cases. One resulted in deployment in the oesophagus, one could not be deployed to the culprit lesion, and one could not be passed down to the culprit lesion due to a proximal stenosis. There was one case of mortality within 30 days. This patient had a through the scope (TTS) clip and adrenaline injection as first line treatment followed by OTSC as second-line which failed necessitating IR intervention.</p><p><b><i>Conclusion:</i></b> OTSC treatment is an effective and feasible treatment for GI bleed, as first line treatment. This effectiveness is particularly notable given that OTSC is typically reserved for larger and more high-risk lesions. Despite being a relatively new technology, and hence less familiarity among endoscopists, technical failures during deployment are uncommon. However, it's important to consider factors such as oesophageal stenosis, which may impede the deployment of the OTSC.</p><p>\n \n </p><p><b>484</b></p><p><b>Those that are not measured suffer: the case for measuring colonoscopy adenoma detection rate in all patients regardless of age</b></p><p><b>Zainul Azhar</b><sup>1,3</sup>, Simone Kefford<sup>2</sup>, Torsten Pennell<sup>2,3</sup>, Chanuli Jayasena<sup>3</sup>, Sophie Jensen<sup>2</sup>, Taylor Gilbert<sup>2</sup>, Andrew Saunders<sup>2</sup>, Daniel Worthley<sup>2</sup> and David Hewett<sup>2,3</sup></p><p><sup>1</sup><i>QEII Jubilee Hospital, Brisbane, Australia;</i> <sup>2</sup><i>Colonoscopy Clinic, Brisbane, Australia;</i> <sup>3</sup><i>Faculty of Medicine, The University of Queensland, Brisbane, Australia</i></p><p><b><i>Background and Aim:</i></b> The incidence of colorectal cancer (CRC) in ages < 50 years is increasing globally. Australian guidelines have endorsed a reduced age of screening initiation, now recommended from age 45. The Hawthorne effect of measuring and reporting ADR motivates endoscopists to perform high quality colonoscopy. However, adenoma detection rates (ADR) are currently only measured in patients aged ≥50 years. This study aimed to assess the impact of measuring and reporting ADR in patients aged 45-49.</p><p><b><i>Methods:</i></b> We conducted a prospective observational study from July 2021 to April 2024 of 16,782 consecutive colonoscopies performed in a large private community clinic in Brisbane. Eligible patients were aged ≥15 years and referred for elective colonoscopy. Exclusion criteria were inflammatory bowel disease, previous colonic resection and incomplete colonoscopy. From July 2021, each doctor received a quarterly report card of colonoscopy quality metrics, including intubation rates, insertion/withdrawal times and detection rates (cancer, adenoma, sessile serrated lesions) for themselves and for all doctors. ADR was reported in patients aged >50 (ADR50). From 1 March 2024, report cards were modified to report ADR in patients aged >45 (ADR45), between 45-49 (ADR45-49) and >50 (ADR50). To assess the impact of the observation of colonoscopy quality in younger patients, we compared ADR before and after 1 March 2024. Outcome measures were ADR45, ADR45-49, and ADR50.</p><p><b><i>Results:</i></b> Overall, ADR in ages 50-54 was 10% higher than in ages 45-49, compared to mean increments of 4.5% for each 5-year increase in age between 40 and 84 years (Figure 1). There was no difference in ADR50 before and after the change in report cards (69.1% vs 69.9%, p 0.66). However, there was a numerical (but not significant) increase in ADR45-49 (46.7% vs 50.6%, p 0.48), which was less for ADR45 (66.8% vs 67.4%, p 0.74).</p><p><b><i>Conclusion:</i></b> The inclusion of ADR in quarterly colonoscopy report cards may improve colonoscopy quality in patients aged 45-49, leveraging the power of the Hawthorne effect. Further longitudinal and larger studies are required.</p><p><b>485</b></p><p><b>The clinical value of \"exception item\" colonoscopy (MBS Item 32228) and predictors of advanced neoplasia</b></p><p><b>Zainul Azhar</b><sup>1,3</sup>, Simone Kefford<sup>2</sup>, Torsten Pennell<sup>2,3</sup>, Chanuli Jayasena<sup>3</sup>, Sophie Jensen<sup>2</sup>, Taylor Gilbert<sup>2</sup>, Andrew Saunders<sup>2</sup>, Daniel Worthley<sup>2</sup> and David Hewett<sup>2,3</sup></p><p><sup>1</sup><i>QEII Jubilee Hospital, Brisbane, Australia;</i> <sup>2</sup><i>Colonoscopy Clinic, Brisbane, Australia;</i> <sup>3</sup><i>Faculty of Medicine, The University of Queensland, Brisbane, Australia</i></p><p><b><i>Background and Aim:</i></b> Most colonoscopies in Australia are subsidised by the Medicare Benefits Schedule (MBS). In November 2019, the MBS introduced an “exception” item (32228) for clinically indicated colonoscopy not covered by other item numbers. Item 32228 is available for a given patient only once. It has been suggested that item 32228 could be removed from the schedule. The aim of this study was to assess the rates of neoplasia in 32228 colonoscopies since its inception and determine any predictors of advanced adenomas among these colonoscopies.</p><p><b><i>Methods:</i></b> We conducted a prospective observational study from July 2021 to April 2024 of 16,783 consecutive colonoscopies performed in a large private community clinic in Brisbane. Eligible patients were aged ≥15 years, referred for elective colonoscopy, and billed MBS item 32228. Exclusion criteria were inflammatory bowel disease, colonic resection, and incomplete colonoscopy. Outcome measures included adenoma detection rate (ADR), advanced adenoma detection rate (AADR), serrated sessile lesion detection rate (SSLDR) and advanced SSLDR (ASSLDR) We used multiple logistic regression to evaluate predictors of colorectal neoplasia including age, sex, index colonoscopy and indication, and to compare detection rates with non-32228 indications.</p><p><b><i>Results:</i></b> There were 1,380 colonoscopies (item 32228) over the 3-year study period. In 32228 colonoscopy, overall ADR, AADR, SSLDR and ASSLDR was 63.6%, 7.0%, 36.1% and 13.70% respectively; cancer was detected in two patients (0.15%). The rates of detection of any advanced polyp (adenoma, SSL) were similar between items 32228 and 32222 (diagnostic procedures: 19.6% vs 19.6%, p=0.99). AADR was lower for item 32228 compared with diagnostic colonoscopy (32222: 6.4% vs 9.0%, p = 0.01), while ASSLDR was similar (13.7% vs 12.0%, p=0.08). Significant predictors for advanced adenomas in ‘32228' colonoscopies were male sex (OR 2.52, p<0.01) and index colonoscopy (OR 2.22, p<0.01). Significant predictors for advanced SSLs were index colonoscopy (OR 1.73, p<0.01) and family history of colorectal cancer (OR 1.39, p=0.04).</p><p><b><i>Conclusion:</i></b> This study builds on our earlier report<sup>1</sup> confirming the clinical relevance of item 32228 with 1 in 5 “exception” colonoscopies detecting advanced colorectal neoplasia. Clinician discretion remains an indispensible component of the MBS for colonoscopy.</p><p><b>Reference</b></p><p>1. \n <span>Lee See, M</span> et al. <span>The clinical value of “exception item” colonoscopy (MBS item 32228)</span>. <i>Med J Aust</i> <span>2022</span>; <span>216</span>: <span>94</span>-<span>95</span>, doi https://doi.org/10.5694/mja2.51241</p><p><b>487</b></p><p><b>Age-standardised adenoma detection rate: exploring the concept of monitoring detection rates for patients of all ages</b></p><p><b>Zainul Azhar</b><sup>1,3</sup>, Simone Kefford<sup>2</sup>, Torsten Pennell<sup>2,3</sup>, Chanuli Jayasena<sup>3</sup>, Sophie Jensen<sup>2</sup>, Taylor Gilbert<sup>2</sup>, Andrew Saunders<sup>2</sup>, Daniel Worthley<sup>2</sup> and David Hewett<sup>2,3</sup></p><p><sup>1</sup><i>QEII Jubilee Hospital, Brisbane, Australia;</i> <sup>2</sup><i>Colonoscopy Clinic, Brisbane, Australia;</i> <sup>3</sup><i>Faculty of Medicine, The University of Queensland, Brisbane, Australia</i></p><p><b><i>Background and Aim:</i></b> Adenoma detection rate (ADR) is the dominant metric for assessing the quality of screening colonoscopy and is inversely related to the risk of post colonoscopy colorectal cancer. ADR is typically measured in patients above 50 years of age. We aim to evaluate the merits of using an age-standardized adenoma ADR as an alternative and inclusive tool for monitoring colonoscopy quality.</p><p><b><i>Methods:</i></b> We conducted a prospective observational study from July 2021 to April 2024 of 16,782 consecutive colonoscopies performed in a large private community clinic in Brisbane. Eligible patients were aged ≥15 years and referred for elective colonoscopy. Exclusion criteria were inflammatory bowel disease, previous colonic resection and incomplete colonoscopy. Outcome measures were ADR in patients >50 years (ADR50), >45 years (ADR45) and age standardized ADR (ASADR) of the practice and individual endoscopists. ASADR is the sum of age-adjusted ADR across all age groups, accounting for the standard population proportion.</p><p><b><i>Results:</i></b> Overall ADR50, ADR45 and ASADR was 69.2%, 66.9% and 60.2% respectively. ASADR for all five individual endoscopists were related to their ADR50 with a median difference of 9.14%. The highest ASADR was 69.4% which corresponded to the endoscopist’s ADR of 77.8% whilst the lowest ASADR was 47.3% corresponding to an ADR of 54.5%.</p><p><b><i>Conclusion:</i></b> Age-standardized ADR is a potential alternative and inclusive marker of colonoscopy quality, which adjusts for patients’ age in ADR calculations. Further research is required to assess its effectiveness for colonoscopy quality monitoring, leveraging the power of the Hawthorne effect.</p><p><b>491</b></p><p><b>The uptake and barriers to artificial intelligence (AI) use in colonoscopy for polyp detection</b></p><p><b>Mohammed Affan Guliyara</b>, Martin Grehan and Calvin Chan</p><p><i>Nepean Blue Mountains Local Health District, Sydney, Australia</i></p><p><b>Background and Aims:</b> The use of Artificial Intelligence (AI) in colonoscopy has shown improvements in polyp detection and characterization, including increased adenoma detection rates (ADR). However, its implementation varies among endoscopists. This study aims to investigate AI utilization in colonoscopy by Australian endoscopists and identify barriers to its routine implementation.</p><p><b><i>Methods:</i></b> We conducted a cross-sectional survey, collecting data on endoscopists' demographics, familiarity, experiences, and reservations regarding AI use in colonoscopy, as well as their general attitudes towards AI. The survey responses were measured using 5-point Likert scales.</p><p><b><i>Results:</i></b> Fourteen proceduralists participated in the web-based survey. The respondents were predominantly male (n=12; 85.7%), with most holding consultant roles (n=11; 78.6%) and specializing in gastroenterology (n=10; 71.4%). Six had less than 5 years of experience (42.9%), and six had over 10 years (42.9%). The majority (n=13; 92.9%) reported high familiarity with AI. Despite this, routine use of AI in colonoscopy was reported by only 23%, while 15% had never used AI. For those who used AI selectively, it was applied in specific cases such as poor bowel preparation, history of serrated polyps, or frail patients with cardiopulmonary comorbidities. Most respondents (n=11; 78.6%) believed AI would enhance polyp detection and increase the number of polyps removed. However, barriers included prolonged colonoscopy times (n=8; 57.2%), false positives (n=8; 57.2%), distraction (n=5; 35.7%), and forgetfulness (n=4; 28.6%). Regarding general attitudes towards AI, most endoscopists felt that AI would improve the quality of care (n=9; 64.3%) and diagnostic efficiency in the future (n=10; 71.4%). They acknowledged potential biases in AI (n=9; 64.3%) and stressed that clinicians must retain final responsibility (n=14; 100%). Reproducible outcomes were deemed a critical feature for AI implementation (n=10; 71.4%). Learning AI technology was not considered a significant barrier (n=10; 71.4%). Despite its limitations, half of the proceduralists intended to use AI technology routinely in patient care in the future (n=7; 50%).</p><p><b><i>Conclusion:</i></b> This study demonstrated that despite high familiarity with AI, its use is limited to selected cases, often hindered by drawbacks such as longer procedure times, false positives, distractions, and forgetfulness. These findings highlight significant barriers to AI adoption among proceduralists at our institution. Addressing these issues can help develop strategies to improve AI uptake during routine colonoscopy.</p><p><b>503</b></p><p><b>Suboptimal inpatient bowel preparation: using a healthcare redesign approach to explore a challenging gastroenterology issue</b></p><p><b>Anna McMahon</b>, Kimberley Ryan, Stefanie Ford, Mark Appleyard and Florian Grimpen</p><p><i>Royal Brisbane and Women's Hospital, Brisbane, Australia</i></p><p><b><i>Background and Aim:</i></b> Bowel preparation for colonoscopy is a standard quality metric. Inadequate bowel preparation is a well-described and challenging issue, particularly for the inpatient cohort in gastroenterology. Adequate bowel preparation is paramount for a safe and optimal diagnostic and therapeutic colonoscopy amongst inpatients. The aim of this study was to contextualise the problem of inadequate bowel preparation in a large tertiary referral hospital.</p><p><b><i>Methods:</i></b> This study utilised Healthcare Redesign methodology as an action research approach, using exploratory sequential mixed-methods. Data was collected from two sources; qualitative, through an informal staff feedback tool which guided and was followed by a retrospective chart audit (Table 1).</p><p><b><i>Results:</i></b> Key themes that emerged from this study included: variation in clinical practice and knowledge, delays and inefficiencies throughout the patient journey, heterogeneity in bowel preparation prescription, documentation and administration of bowel preparation medications and fragmented communication.</p><p><b><i>Conclusion:</i></b> This mixed-methods approach has yielded important insights into the potential causes of inadequate bowel preparation amongst a patient cohort undergoing bowel preparation as an inpatient, providing a great opportunity for change. Findings will inform clinical re-design initiatives aimed to target the identified inefficiencies to improve clinical and process outcomes in hospitalised patients undergoing bowel preparation for colonoscopy.</p><p><b>531</b></p><p><b>Prospective validation of a novel vision transformer model to detect early neoplasia for Barrett’s surveillance: an interim analysis</b></p><p><b>Jin Lin Tan</b><sup>1,2</sup>, Dileepa Pitawela<sup>3</sup>, Mohamed Asif Chinnaratha<sup>1,2</sup>, Hsiang-Ting Chen<sup>3</sup> and Rajvinder Singh<sup>1,2</sup></p><p><sup>1</sup><i>Department of Gastroenterology, Lyell McEwin Hospital, Adelaide, Australia;</i> <sup>2</sup><i>Faculty of Health and Medical Sciences, The University of Adelaide, Adelaide, Australia;</i> <sup>3</sup><i>Australian Institute for Machine Learning, The University of Adelaide, Adelaide, Australia</i></p><p><b><i>Background and Aim:</i></b> Artificial Intelligence (AI) models based on Convolutional Neural Networks (CNN) have been shown to improve detection rates of early Barrett’s neoplasia. However, present algorithms are predominantly trained on white-light imaging (WLI) (1). In addition, models trained on CNN may face issues with scalability as training datasets becomes larger with time. Vision Transformer (ViT) has emerged as the new state-of-the-art deep learning model in the field of computer vision, outperforming CNN models in terms of computational efficiency for larger datasets and accuracy. ViT leverages the power of transformers, using an “attention” mechanism originally designed for natural language processing, for spatial and temporal analysis of images and videos. This study aims to prospectively validate BE-ViT, a pilot ViT model developed to detect early Barrett’s neoplasia on both WLI and narrow-band imaging (NBI).</p><p><b><i>Methods:</i></b> The BE-ViT model was pre-trained with ImageNet. We subsequently trained the model on a dataset of 1,918 (275 patients) clinically validated images of Barrett’s oesophagus with and without neoplasia. The training dataset comprised of 835 WLI and 1,083 NBI images. There were 287 WLI and 262 NBI images which contained neoplasia. Patients with Barrett’s oesophagus undergoing endoscopic surveillance from a large tertiary referral centre from Feb 2022 to Mar 2024 were included in this study. The prospective validation dataset comprised of 380 (14 patients) images: 99 (4 patients) neoplastic images and 281 (13 patients, including three patients in the former group after receiving endoscopic eradication therapy) images without neoplasia. The primary outcome was the performance of the BE-ViT model, which was assessed by accuracy, sensitivity and specificity.</p><p><b><i>Results:</i></b> BE-ViT achieved the following performances for WLI images (80.4% accuracy, 70.6% sensitivity and 84.9% specificity) and NBI images (78.0% accuracy, 70.8% sensitivity and 80.3% specificity), respectively. Excluding images containing low-grade dysplasia, performance improved for both WLI images (81.2% accuracy, 71.4% sensitivity and 84.9% specificity) and NBI (79.2% accuracy, 75.4% sensitivity and 80.3% specificity).</p><p><b><i>Conclusion:</i></b> The pilot BE-ViT model shows promising potential in detecting early Barrett’s neoplasia. This new algorithm is expected to enhance accuracy and outperform current models when trained and refined on larger datasets, marking an important step forward in improving early detection and patient outcomes in patients with Barrett’s oesophagus.</p><p><b>Reference</b></p><p>\n 1. <span>Tan, JL</span>, <span>Chinnaratha, MA</span>, <span>Woodman, R</span>, <span>Martin, R</span>, <span>Chen, H-T</span>, <span>Carneiro, G</span>, et al. <span>Diagnostic Accuracy of Artificial Intelligence (AI) to Detect Early Neoplasia in Barrett’s Esophagus: A Non-comparative Systematic Review and Meta-Analysis</span>. <i>Front Med (Lausanne)</i>. <span>2022</span> Jun 22; <span>9</span>:890720.</p><p><b>541</b></p><p><b>Diffuse oesophageal candidiasis identified on 18F-fluorodeoxyglucose positron emission tomography/computed tomography scan</b></p><p><b>Christopher James Shephard</b><sup>1</sup>, William Jiaen Wang<sup>1,2,3</sup> and Bulent Baran<sup>1</sup></p><p><sup>1</sup><i>Department of Gastroenterology and Hepatology, Townsville University Hospital, Townsville, Australia;</i> <sup>2</sup><i>Department of Gastroenterology and Hepatology, Princess Alexandra Hospital, Brisbane, Australia;</i> <sup>3</sup><i>School of Medicine, Western Sydney University, Sydney, Australia</i></p><p><b><i>Introduction:</i></b> Candida is a commensurate yeast of the gastrointestinal tract, with colonisation rates up to 20% reported in healthy adults. However, symptomatic oropharyngeal/oesophageal candidiasis may develop in the setting of immunosuppression – namely malignancy and anti-neoplastic therapy. Candida oesophagitis typically presents with dysphagia/odynophagia and typical white/yellow mucosal plaque-like lesions visualised at endoscopy and confirmed on biopsy, however it may also be suspected on imaging performed for another purpose. <sup>18</sup>F-fluorodeoxyglucose (FDG) positron emission tomography/computed tomography (PET/CT) is frequently performed in oncology patients for staging and evaluation of treatment response. Abnormal oesophageal FDG uptake with high maximum standard uptake value (SUV<sub>max</sub>) may be observed in candidiasis, malignancy and rarely, immune checkpoint inhibitor (ICI)-mediated oesophagitis. To avoid misdiagnosis, unexpected focal and/or intense visualisation of FDG uptake should prompt endoscopic and histological evaluation, especially if SUV<sub>max</sub> exceeds 3.5.</p><p><b><i>Case report:</i></b> A 54-year-old male with stage IV lung adenocarcinoma receiving maintenance pembrolizumab was admitted from oncology clinic for evaluation of dysphagia/odynophagia with vomiting and 9kg of unintentional weight loss over the preceding month. He also reported pain from several oral mucosal ulcers over the same timeframe, commencing nystatin suspension without clinical improvement. His background was pertinent for lower limb venous thrombosis with pulmonary embolism, hypertension and recent mild hypokalaemia. Current medications included pantoprazole, apixaban, perindopril, oxycodone/naloxone and slow-release potassium. He is an ex-smoker but seldom consumes alcohol. On examination his tongue appeared white-coated without obvious mucosal ulceration. FDG-PET/CT scan five days prior showed no significant pulmonary uptake in keeping with oncological treatment response; however, it highlighted intense tracer uptake throughout the oral cavity and entire oesophagus (Figure 1). Admission investigations showed a leukocytosis of 16.4x10<sup>9</sup>/L, C-reactive protein 24mg/L, potassium 3.1mmol/L and acute kidney injury with creatinine 105micromol/L. Human immunodeficiency virus serology was negative. He received intravenous hydration and potassium replacement. Although there was a high clinical suspicion of oesophageal candidiasis, endoscopy was performed to exclude oesophageal malignancy and ICI-mediated oesophagitis. Oesophagogastroduodenoscopy (OGD) revealed extensive white-yellow plaques throughout the oesophagus (Figure 2). Biopsy demonstrated significant necro-inflammatory debris and inflammation in the setting of fungal hyphae consistent with oesophageal candidiasis, alongside reactive atypia but no neoplasia. The patient completed a 14-day course of fluconazole and amphotericin lozenge (initiated prior to biopsy results) with gradual resolution of symptoms. Nystatin suspension was recommended thereafter to prevent recurrence.</p><p><b><i>Conclusion:</i></b> This case highlights the diagnostic challenges of abnormal oesophageal FDG uptake in oncology patients which is non-specific as it can be physiologic, infective, inflammatory or neoplastic in nature. In this case the FDG uptake was due to oesophageal candidiasis and although it was suspected clinically due to its high prevalence among patients with solid organ tumours, FDG-PET/CT cannot reliably exclude crucial differentials. Endoscopic evaluation with biopsy is necessary for diagnostic clarity to guide targeted treatment which in this case was anti-fungal therapy.</p><p><b>543</b></p><p><b>“Segment anything” with MedSAM: Annotation of Barrett’s dysplasia dataset using artificial intelligence</b></p><p><b>Jin Lin Tan</b><sup>1,2</sup>, Ka Hing Chan<sup>3</sup>, Dileepa Pitawela<sup>3</sup>, Mohamed Asif Chinnaratha<sup>1,2</sup>, Hsiang-Ting Chen<sup>3</sup> and Rajvinder Singh<sup>1,2</sup></p><p><sup>1</sup><i>Department of Gastroenterology, Lyell McEwin Hospital, Adelaide, Australia;</i> <sup>2</sup><i>Faculty of Health and Medical Sciences, The University of Adelaide, Adelaide, Australia;</i> <sup>3</sup><i>Australian Institute for Machine Learning, The University of Adelaide, Adelaide, Australia</i></p><p><b><i>Background and Aim:</i></b> Expert annotations are vital for developing Computer Aided Detection (CADe) and Diagnosis (CADx) systems in endoscopy. While it is relatively easy for clinicians to draw a \"bounding box\" around a lesion, the process of outlining the lesion's exact contours, known as \"segmentation,\" is much more time-consuming. Segmentation annotations are especially crucial for highlighting subtle contour irregularities in lesions, such as early Barrett’s dysplasia. MedSAM, a state-of-the-art model trained on 1.5 million images across ten imaging modalities and over thirty cancer types, can automatically assist clinicians in performing various medical segmentation tasks (1). Prior to MedSAM, training segmentation models required laborious per-pixel annotations, whereas MedSAM simplifies the process by needing only a \"bounding box\" prompt to perform image segmentation, significantly reducing annotation time. In this study, we aim to evaluate the performance of MedSAM on a Barrett’s dysplasia dataset comprising of endoscopic images obtained using Narrow-band imaging (NBI), where lesions have irregular contours and mucosal pit patterns.</p><p><b><i>Methods:</i></b> 248 images from 36 unique patients containing Barrett’s dysplasia (high-grade dysplasia and adenocarcinoma) were annotated by experts and verified against histology reports. There were 196 images from 29 unique patients in the training dataset and 52 images from 7 unique patients in the testing dataset. We trained a model using YOLO v8 to localise areas of dysplasia with a bounding box, which MedSAM used for segmentation (see Figure 1). The dysplasia localisation and segmentation accuracy were assessed using the Intersection over Union (IoU) and Dice coefficient scores, respectively.</p><p><b><i>Results:</i></b> For Barrett’s dysplasia localisation, our model achieved an average IoU of 71.1%, demonstrating significant overlap between predicted and ground truth bounding boxes. Regarding dysplasia segmentation, an average DICE coefficient score of 71.7% was attained, indicating good precision.</p><p><b><i>Conclusion:</i></b> This study demonstrates the potential of using MedSAM to accelerate and scale the annotation of large endoscopic image and video datasets, as well as its applicability to real-time segmentation in endoscopy in the future. Accurate segmentation could also help endoscopists delineate margins better prior to performing endoscopic resection.</p><p><b>Reference</b></p><p>\n 1. <span>Ma, J</span>, <span>He, Y</span>, <span>Li, F</span>, <span>Han, L</span>, <span>You, C</span>, <span>Wang, B</span>. <span>Segment anything in medical images</span>. <i>Nature Communications.</i> <span>2024</span> Jan 22; <span>15</span>(<span>1</span>): <span>654</span>.</p><p><b>548</b></p><p><b>Lower prevalence of sessile serrated lesions in Asian patients compared to non-Asian patients undergoing bowel cancer screening colonoscopy</b></p><p><b>Andrew Tang</b><sup>1,2</sup>, Jarinya Soieprasounk<sup>1</sup>, Rachel Halkhoree<sup>1</sup>, Karen Jones<sup>1</sup>, Cameron Bell<sup>1,2</sup> and Ian Norton<sup>1,2</sup></p><p><sup>1</sup><i>Ryde Hospital, Sydney, Australia;</i> <sup>2</sup><i>Royal North Shore Hospital, Sydney, Australia</i></p><p><b><i>Background and Aim:</i></b> The accurate identification and removal of precursor lesions is fundamental to colorectal cancer screening. Colonic polyps acquire malignant mutations through two pathways - the classic adenoma-carcinoma sequence and the serrated pathway. Adenoma detection rates (ADR) and sessile serrated lesion detection rates (SSLDR) are widely utilised quality indicators of colonoscopy. Mandatory Australian colonoscopy recertification requires proceduralists to demonstrate an ADR of 25% in all patients over the age of 50 with intact colons. An SSLDR of 5% is currently suggested but will soon be another mandatory KPI. These benchmarks are derived from mostly Caucasian-based studies and current ADR and SSLDR recommendations do not account for ethnic differences. We hypothesise that there could be ethnic variations in the prevalence of adenomatous and sessile serrated lesions, particularly in Asian populations, and this could affect colonoscopy ADR and SSLDR in some practice areas.</p><p><b><i>Methods:</i></b> We conducted a single-centre retrospective cohort study of patients undergoing colonoscopy following positive faecal occult blood test (FOBT) as part of the National Bowel Cancer Screening Program between November 2021 and October 2023 by two experienced endoscopists. Endoscopy and histopathology reports were reviewed to determine type, size and location of lesions. Ethnicity was based on recorded country of birth with patients born in East Asian and South-East Asian countries being classified as Asian for our study. Incomplete procedures, whether by inadequate bowel preparation or failure of caecal intubation, were excluded from analysis.</p><p><b><i>Results:</i></b> A total of 393 patients underwent colonoscopy during the study period including 217 Asian patients (55%) and 176 non-Asian patients (45%). There was no significant difference in baseline characteristics including age and gender. The prevalence of sessile serrated lesions was significantly lower in Asian patients (2.76%) compared to their non-Asian (7.95%) counterparts (P-value = 0.019). By contrast, there was no difference in the prevalence of adenomatous lesions between Asian and non-Asian patients, including in tubular adenoma, advanced adenoma and colon cancer detection.</p><p><b><i>Conclusion:</i></b> Current benchmarks for adenoma and sessile serrated lesion detection rates do not account for ethnic variation. Our study demonstrates that sessile serrated lesions were significantly less common in Asian patients compared to non-Asian patients undergoing colonoscopy arising from an FOBT program. This should be reflected in quality indicators used to determine colonoscopy competence in certain practice populations.</p><p><b>549</b></p><p><b>The yield of endoscopic assessment for iron deficiency in adults</b></p><p><b>Gary Zhang</b><sup>1</sup>, John Olynyk<sup>1,2,3,4</sup> and Oyekoya Ayonrinde<sup>1,2,3</sup></p><p><sup>1</sup><i>Fiona Stanley Hospital, Perth, Australia;</i> <sup>2</sup><i>The University of Western Australia, Perth, Australia;</i> <sup>3</sup><i>Curtin University, Perth, Australia;</i> <sup>4</sup><i>Edith Cowan University, Perth, Australia</i></p><p><b><i>Background and Aim:</i></b> Iron deficiency (ID) is the predominant cause of anaemia and is the commonest micronutrient deficiency worldwide. Age, gender, ethnic background, and severity of ID and/or anaemia (IDA) determine the potential significance, hence the need for targeted investigations to establish an aetiology. Suspected blood loss from the gastrointestinal tract or impaired gastrointestinal absorption are common causes of referral for endoscopic investigation of iron deficiency. Bidirectional endoscopic examination is generally recommended for IDA, as it detects a cause in two-thirds of men and post-menopausal women. There are over 800,000 MBS subsidised colonoscopies per annum in Australia. The diagnostic yield from these when iron deficiency is the primary indication is not known. We aimed to investigate the yield of endoscopic assessment for iron deficiency.</p><p><b><i>Methods:</i></b> The electronic endoscopy database at a single metropolitan hospital in Western Australia was retrospectively searched for endoscopic examinations performed for the indications ‘iron deficiency’ and ‘anaemia’ between 1<sup>st</sup> January 2023 to 31<sup>st</sup> December 2023. Indications, patient characteristics, diagnostic and therapeutic outcomes of endoscopic assessment, and histopathology results of patients with iron deficiency were extracted from the clinical records of unselected patients.</p><p><b><i>Results:</i></b> Of the 250 patients reviewed, 171 (68.4%) had non-anaemic iron deficiency (NAID), 54 (21.6%) had iron deficiency with anaemia (IDA), and 25 patients had anaemia alone or no documented confirmation of iron deficiency. The pathologies identified on endoscopy, stratified by the groups are described in table 1. In the NAID group, the median age was 51 years (IQR 41-63), with 35.1% aged ≤45 years, 71.9% were female, and 90.6% had both gastroscopy and colonoscopy, while 3.51% underwent colonoscopy alone and 5.85% had gastroscopy alone. In the NAID group no patient had colorectal cancer, but one patient had oesophageal adenocarcinoma (0.6%). Other findings included coeliac disease (3.51%), <i>Helicobacter pylori</i> infection (13.5%) and ileal Crohn’s disease (0.6%). In the IDA group, the median age was 49 years (IQR 43-66), with 37% aged ≤45 years, 75.9% were female, and 96.3% had both gastroscopy and colonoscopy. Overall, there was a higher diagnostic yield for potential causes of iron deficiency, using gastroscopy compared with colonoscopy. More malignancies were identified in the IDA group, including oesophageal adenocarcinoma (1.85%), and colorectal adenocarcinoma (3.7%). In patients aged ≤45 years (n=80), the NAID subgroup had 47 females and 13 males; while the IDA subgroup comprised 18 females and 2 males. No malignancies were detected in the young patients, although other pathologies including coeliac disease (7.5%), <i>H pylori</i> (13.75%), and ulcerative colitis (1.25%) were identified.</p><p><b><i>Conclusion:</i></b> Most gastrointestinal causes of iron deficiency were detected using gastroscopy. In the absence of specific gastrointestinal symptoms, IDA, or mid-older age, it may be reasonable to initiate endoscopic investigation of iron deficiency with gastroscopy. This two-step approach could be most relevant to patients who have had colonoscopy in the preceding three years. Further larger studies are required to confirm safety and cost effectiveness of this proposed stepwise and/or a serological testing approach in younger patients with NAID.</p><p>\n \n </p><p><b>557</b></p><p><b>Treatment of haemorrhoids via rubber band ligation followed by pudendal nerve block for analgesia complicated by ischial osteomyelitis: A case report</b></p><p><b>Jason Zhang</b>, Sarah Taylor, Anil Bhagwat, Christopher Middleton and Brent Mitchell</p><p><i>Royal Hobart Hospital, Hobart, Australia</i></p><p><b><i>Introduction:</i></b> Rubber band ligation (RBL) is a procedure used to treat symptomatic haemorrhoids that have failed conservative management. Post operative pain is very common affecting up to 90% of patients. Subsequently pudendal nerve blocks (PNB) have been increasingly utilised as an adjunct to oral analgesia. We discuss a case of ischial osteomyelitis that is a rare but serious complication post PNB.</p><p><b><i>Case report:</i></b> A 53 year old male underwent a colonoscopy for recurrent rectal bleeding. He had no significant medical history, was not immunosuppressed and was not on any regular medications. Rubber band ligation was performed to three columns of large prolapsing haemorrhoids. Bilateral pudendal nerve blocks were performed via a transgluteal technique. The procedure was performed by a senior gastroenterologist with many years of experience performing RBL with PNB. The patient was placed in left lateral position and the perianal area was washed with chlorhexidine. Anatomical landmarks were identified - the ischial tuberosity was palpated percutaneously as was the ischial spine. A 23 gauge needle was inserted percutaneously medial to the ischial tuberosity coursing toward the ischial spine and 20ml of 0.25% bupivacaine injected medial and posterior to the ischial spine. This targets the pudendal nerve as it courses over the sacrospinous ligament and its attachment to the ischial spine into the lesser sciatic foramen. Following the procedure the patient experienced persistent worsening pain and tenderness of the right gluteal region for several weeks. MRI scan showed marrow oedema and swelling within the right ischial tuberosity and oedema of adductor magnus tendon. A subsequent PET/CT showed moderate FDG activity in the right ischial tuberosity with osseous destruction and uptake in the proximal adductor magnus muscle. These findings were suggestive of ischial osteomyelitis and concurrent myositis, likely as a result of inadvertent needle injury to the area and infiltration of local anaesthetic. Further investigations demonstrated a white cell count of 10.3, with neutrophils of 6.7 and a C reactive protein of 15. Multiple sets of blood cultures were negative. Two attempts were made to obtain tissue to confirm osteomyelitis and guide antimicrobial therapy via CT guided biopsy of the ischial tuberosity but unfortunately the samples were non-diagnostic and did not culture an organism. The patient was referred onto the infectious diseases team for consideration of empirical antibiotic therapy. Pudendal nerve blocks are effective in anaesthetising the posterior perineum, anus and genitals and effects are usually noted quickly within 20 minutes. A cross-sectional analysis of RBL for haemorrhoids in Australia accounted for a total of 346542 procedures from 2012 to 2021. Between 2012-13, 1.62% of patients received a PNB compared with 6.63% of patients between 2020-2021. The most common side effect is injection site pain, but other potential complications include bleeding, infection, damage to nerves and surrounding structures and a rare risk of systemic local anaesthetic toxicity. A variety of techniques are utilised including the transvaginal, transperineal, perirectal and transgluteal approach which is often operator dependent. Imaging guidance via ultrasound, CT and fluoroscopy have also been utilised to better delineate underlying structures and avoid injury to surrounding tissue, but this may not be feasible at the time of procedure.</p><p><b><i>Conclusion:</i></b> With the increasing utilisation of PNB for anorectal procedures, this case describes an uncommon and serious complication of the procedure which has not been previously described in literature. It highlights the importance of correct identification of anatomical landmarks and aseptic technique in minimising the risk of infective adverse events.</p><p><b>562</b></p><p><b>Incidental finding of a neuroendocrine tumour on polypectomy</b></p><p><b>Ruth Ducommun</b> and Myat Khaing and Dennis Rubtsov and Reuben Malloy and Rebecca Cohen and Ayesha Chapagain</p><p><i>The Prince Charles Hospital, Brisbane, Australia</i></p><p><b><i>Introduction:</i></b> Neuroendocrine tumours (NET) are a rare but increasing finding within Queensland. The incidence has tripled from 2 per 100,000 to approximately 6.3 per 100,000 people in 2015 over the last three decades. Rectal NETs are typically 5-10 cm from the dentate line with white or yellow retroflexion. They are poorly recognised with no distinct morphological or pathognomonic features and less than twenty percent of NETs were suspected as such by the endoscopist before a biopsy was performed. Neuroendocrine tumours are found in the lung, appendix, small bowel, pancreas, rectum and can also have an unknown primary site. Most rectal NETs are detected incidentally on surveillance colonoscopy and have a favourable prognosis when fully resected. Endoscopic Mucosal Resection to fully resect the NET is advisable with lesions greater than 3mm, however they are most often found incidentally post-polypectomy. Here in this case, if this NET was not incidentally discovered it would likely have grown and had a far worse prognosis, highlighting the need to biopsy polyps.</p><p><b><i>Case report:</i></b> A 53-year-old female underwent surveillance colonoscopy for suspected Sessile Serrated Polyposis syndrome in December 2023. Fifteen polyps were resected, with one 5mm Paris IIa NICE I (hyperplastic appearing polyp) removed with cold snare. The histopathology unexpectedly came back positive for a rectal NET which was 2.3 mm in maximal dimension. It was described as a bland epithelioid neoplasm extending into the lower lamina propria and transected at the lower margin, no invasion into the lymphovascular or perineural invasion was seen. No mitosis or necrosis was found. She had a clear DOTOTATE PET scan and repeat clear colonoscopy, showing no evidence of local recurrence. This confirmed a Grade One rectal NET, Ki67 index <1%, with no nodal metastasis, which has an approximate 100% survival rate at five years.</p><p><b><i>Conclusion:</i></b> This case study highlights the lack of distinct morphological characteristics of neuroendocrine tumours and the need for tissue sample to diagnose this rare potentially life-threatening condition. Recurrence post polypectomy of rectal NETs is estimated at five percent, however in one study of 345 patients, this led to two deaths. Endoscopic Mucosal Resection is indicated when the tumour is >3mm, with surgery indicated when the NET is >2cm, or 1-2cm with risk factors such as high mitotic rate on histopathology. Diagnosis is essential for appropriate management. Most NETs have no distinct pathognomonic features with normal overlying mucosa, which complicates detection. Diagnosis of NETs, whilst difficult, is also exceedingly important as early recognition improves survival.</p><p><b>563</b></p><p><b>Real-time use of artificial intelligence (CADx) on polyp characterisation during colonoscopy: the first Australian trial</b></p><p><b>Lulu Zhang</b><sup>1,2</sup>, Timothy O'Sullivan<sup>1,2</sup>, Enoka Gonsalkorala<sup>1,2</sup>, Florian Grimpen<sup>1</sup>, Guy Lampe<sup>1</sup>, Sally Roberston<sup>1,2</sup>, Katherine Hanigan<sup>1,2</sup>, Lee Jones<sup>3</sup>, Patricia Valery<sup>3</sup> and Mark Appleyard<sup>1,2</sup></p><p><sup>1</sup><i>Royal Brisbane and Women's Hospital, Brisbane, Australia;</i> <sup>2</sup><i>Surgical Treatment and Rehabilitation Service (STARS), Brisbane, Australia;</i> <sup>3</sup><i>QIMR Berghofer, Brisbane, Australia</i></p><p><b><i>Background and Aim:</i></b> Colonoscopy is the gold standard for detecting and resecting colorectal polyps, playing a critical role in bowel cancer prevention. The national bowel cancer screening programs has significantly increased the number of colonoscopies performed, impacting the provision of public Gastroenterology services. Accurate polyp diagnosis is essential to avoid unnecessary polypectomies, thereby supporting cost-saving strategies. Examples of these strategies include the “leave-in-situ” approach for hyperplastic polyps ≤5 mm located in the rectosigmoid region and the “resect-and-discard” approach for ≤5 mm proximal polyps. Recent advancements in artificial intelligence (AI) technology, particularly computer-aided diagnosis (CADx) modules, have made these strategies feasible by providing a real-time optical diagnosis, distinguishing between adenomatous and non-adenomatous polyps during colonoscopy. One promising model is the Medtronic GI Genius CADx module, whose effectiveness has been previously studied in Italy and Japan. At present, no Australian studies have evaluated its use in routine colonoscopy practice. Therefore, our aim is to assess the accuracy of real-time CADx during colonoscopy and determine the appropriateness of implementing “leave-in-situ” and/or “resect-and-discard” strategies in an Australian context.</p><p><b><i>Methods:</i></b> This is a prospective single-centre study reviewing the Medtronic GI Genius CADx module on polyp characterisation for consecutive patients undergoing colonoscopy over a three-month period. During each colonoscopy, the CADx module provided a real-time optical diagnosis for each visualised polyp. Polyps were then resected and sent to a specialised GI pathologist for histological diagnosis. Statistical analysis was conducted using generalised mixed binary logistic models to determine the sensitivity, specificity, and negative predictive value (NPV) of the CADx module. Diagnostic agreement between optical and histological diagnosis was then assessed using Gwet’s statistics.</p><p><b><i>Results:</i></b> We aim to examine 486 polyps in about 244 patients to meet statistical significance. At the time of abstract submission, data collection is still in progress. However, preliminary results will be available by the time of the AGW conference. Based on recent findings from Hassan et al who reviewed the same technology, we anticipate a sensitivity of 82%, a specificity is 93% and NPV of 97.6%. Hassan et al predicted that utilisation of the CADx system had the potential of 44.4% reduction of all polypectomies with the “leave-in-situ” strategy as well as an 83% reduction for need for pathology with the “resect and discard” strategy.</p><p><b><i>Conclusion:</i></b> We will be the first Australian study to review the accuracy of CADx in polyp characterisation during real-time colonoscopy, with significant cost-saving potential for the public healthcare system.</p><p><b>567</b></p><p><b>Caecal Dieulafoy’s lesion – a rare cause of lower gastrointestinal bleeding</b></p><p><b>Christopher James Shephard</b> and Bulent Baran</p><p><i>Department of Gastroenterology and Hepatology, Townsville University Hospital, Townsville, Australia</i></p><p><b><i>Introduction:</i></b> A Dieulafoy’s lesion (DL) is a dilated aberrant submucosal artery that erodes the overlying epithelium in the absence of a primary ulcer. A DL is implicated in 1-2% of all gastrointestinal (GI) bleeds, of which only 2% involve the colon or rectum. Bleeding is typically associated with older age, cardiovascular disease (CVD), chronic kidney disease (CKD), diabetes, and/or alcohol abuse; anticoagulation further compounds the risk. Per limited reports, caecal DLs usually present with painless haematochezia, although isolated melaena or a mixed bleeding picture is possible. Lesions are difficult to visualise endoscopically owing to their small size/calibre and typical lack of mucosal abnormality, further complicated by inadequate bowel preparation and/or diverticulosis with respect to colonic lesions. Endoscopy is particularly advantageous if performed during acute haemorrhage as active arterial pumping may be observed from an area of mucosa devoid of erosion/ulceration. Endotherapy combining thermal and mechanical haemostatic techniques is favoured over injected monotherapy, owing to lower rates of re-bleeding.</p><p><b><i>Case report:</i></b> A 78-year-old woman was referred to hospital by her general practitioner following six days of painless haematochezia and dark stools mixed with bright red blood. Since bleeding onset, she reported light-headedness and worsening of baseline dyspnoea on exertion. Her history was pertinent for nonischaemic cardiomyopathy, slow atrial fibrillation on dabigatran with a pacemaker in situ, diabetes mellitus and CKD stage 3a without any prior GI bleeding. On presentation she was pale and hypotensive with a systolic blood pressure of 93mmHg. Her abdomen was soft and non-tender. Digital rectal examination confirmed melaena mixed with fresh blood. Initial investigations were significant for a haemoglobin of 50g/L and reticulocytosis, normal platelet count and an elevated international normalised ratio of 1.9. Biochemistry highlighted urea of 22.0mmol/L with acute-on-chronic renal impairment evidenced by a creatinine of 135μmol/L (baseline approx. 95μmol/L). Initial resuscitation consisted of intravenous fluid and transfusion of four units of packed red blood cells with subsequent haemoglobin incrementation to 95g/L. Dabigatran was temporarily withheld. Initial upper endoscopy did not identify a bleeding source. Follow-on colonoscopy revealed clotted blood throughout the entire colon and a DL with pulsatile arterial bleeding in the caecum (Figure 1). Haemostasis was achieved using underwater bipolar coagulation probe followed by three haemostatic clips (Figure 2). No active bleeding was evident at procedure close. The patient was monitored in hospital and dabigatran was recommenced after 48hours without concern for re-bleeding.</p><p><b>577</b></p><p><b>Safety and efficacy of light sedation in low-risk endsocopy</b></p><p><b>Babak Sarraf</b>, Reffai Syed Mohamed and Seema Shah</p><p><i>Townsville University Hospital, Townsville, Australia</i></p><p><b><i>Background and Aim:</i></b> Multiple models of care exist for delivery of sedation during endoscopic procedures. Light sedation, achieved by administration of fentanyl and midazolam, without additional agents such as propofol, has become increasingly adopted internationally for low-risk endoscopy. As there is limited Australian data, we performed a retrospective study of the safety and efficacy of non-anaesthetist delivered light sedation for endoscopic procedures.</p><p><b><i>Methods:</i></b> We undertook a retrospective audit of endoscopy performed under light sedation during 2022 at a tertiary hospital in Queensland, Australia. Ethics approval was obtained. High risk and general anaesthetic procedures were excluded. A random sample of 89 procedures on the light sedation list was analysed for demographics, indication, comorbidities, sedation parameters, procedural challenges and complications. Anaesthetic risk was measured by the American Society of Anesthesiology (ASA) score.</p><p><b><i>Results:</i></b> The 89 procedures constituted 34 gastroscopies, 49 colonoscopies, and 6 flexible sigmoidoscopies. The cohort included 37 females (41.5%) and 52 males (58.4%). The mean age was 57 years old. Most cases had an ASA score of 2 (63%), followed by ASA 3 (21.3%) and 2 (14.6%).</p><p>Two colonoscopies were performed without any sedation due to social circumstances. All other procedures (87) were performed with a combination of fentanyl and midazolam, with a mean dose of 110 micrograms and 3 milligrams respectively per procedure. In 3 colonoscopies, inhaled nitrous oxide was used as an adjunct, facilitating completion of the procedure. No sedation related adverse events or complications were identified. Notably, one colonoscopy was unable to be completed due to patient discomfort, and was repeated under general anaesthetic. Furthermore, 15 cases were reported as technically difficult, with 6 cases attributed to non-sedation related technical factors such as body habitus. In 9 (10.1%) cases, however, patient discomfort was cited as contributing to the technical difficulty. The majority of these cases were colonoscopies (7; 7.9%), with 1 flexible sigmoidoscopy (1.1%) and 1 gastroscopy (1.1%).</p><p><b><i>Conclusion:</i></b> In a unit with local expertise, light sedation is safe and effective for performing low-risk endoscopy procedures. In about 10% of cases, patient discomfort may contribute to technical difficulty, particularly in colonoscopies. However, adjuncts such as inhaled nitrous oxide can improve tolerability. Further studies including cost-analysis are required to establish the role of hybrid models of sedation in the Australian endoscopy setting.</p><p><b>581</b></p><p><b>Life-threatening upper gastrointestinal bleeding following percutaneous endoscopic gastrostomy tube removal under traction</b></p><p><b>Christopher James Shephard</b><sup>1</sup>, Xiaomin Ma<sup>1,2</sup> and Rozemary Karamatic<sup>1</sup></p><p><sup>1</sup><i>Department of Gastroenterology and Hepatology, Townsville University Hospital, Townsville, Australia;</i> <sup>2</sup><i>School of Medicine, University of Queensland, Brisbane, Australia</i></p><p><b><i>Introduction:</i></b> Percutaneous endoscopic gastrostomy (PEG) tubes are commonly inserted for long-term enteral feeding. Gastrointestinal (GI) bleeding is reported in up to 2.67% of patients following tube insertion often due to disruption of small gastric vessels. Haemorrhage following tube removal is comparatively rare, with a recent retrospective analysis of 127 cases of traction removal recording zero bleeding events. Post-removal bleeding has been successfully managed with Foley catheter balloon tamponade or endoscopic over-the-scope clipping (OTSC) per previous reports. We present a case of life-threatening GI bleeding following traction PEG tube removal necessitating urgent endotherapy, followed by definitive surgical management – a mode of intervention not previously described.</p><p><b><i>Case report:</i></b> A 73-year-old female undergoing rehabilitation following craniotomy and cranioplasty for subdural haemorrhage was transferred to the emergency department with large volume haematemesis and melaena five hours after PEG tube removal under traction. The tube (original with bumper, appropriate for traction removal) was inserted without complication four months prior for neurological dysphagia without intervening site issues. Background was relevant for monoclonal gammopathy of unknown significance, complex splenic cyst, α<sup>+</sup>-thalassemia trait, laparoscopic cholecystectomy and GI bleed following hyperplastic gastro-oesophageal junction polypectomy, but no previous gastric surgery. She was not on antiplatelet or anti-inflammatory drugs and had not received enoxaparin thromboprophylaxis for 48hours. Presenting haemoglobin was 75g/L from 97g/L three days prior, with platelets of 139x10<sup>9</sup>/L, international normalised ratio of 1.1 and urea of 13.1mmol/L. She continued to have haemodynamically unstable GI bleeding despite aggressive resuscitation and blood transfusion. Rotational thromboelastometry (ROTEM) was conducted en route to emergent endoscopy under anaesthetic support. Upper endoscopy revealed copious fresh and clotted blood in the stomach with active arterial bleeding from the gastrostomy site (Figure 1A). Initial haemostasis was achieved with adrenaline injection around the site plus eight haemostatic clips (Figure 1B). The patient received ROTEM-guided cryoprecipitate and a total seven units of packed red cells on day one of admission, alongside a continuous pantoprazole infusion. Persistent GI bleeding the following day prompted computed tomography abdominal angiogram which demonstrated haematoma involving the PEG tract but no active contrast extravasation or free air, suggesting a sealed tract. Overnight, further haematemesis with haemodynamic instability and worsening anaemia dictated further transfusion and ROTEM-guided Prothrombinex. Due to concern for ongoing bleeding within the PEG tract likely non-amenable to endotherapy or tamponade via tube reinsertion (concern for false tract formation and additive trauma), surgical opinion was sought. Repeat endoscopy (with surgery on standby) revealed clotted gastric blood with haemostatic clips in situ, but no new/alternative bleeding focus. She proceeded to emergency laparotomy, with intra-operative findings of PEG tract haematoma extending under adjacent mesentery, and a limb of omentum interposed between the stomach and abdominal wall harbouring a bleeding vessel. Definitive haemostasis was achieved following excision of the PEG tract.</p><p><b><i>Conclusion:</i></b> Traction PEG tube removal may be rarely complicated by severe, haemodynamically unstable GI bleeding requiring repeated blood transfusion and ROTEM-guided correction of coagulopathy. Arterial bleeding from within the PEG tract may be challenging to treat endoscopically, and even OTSC may not have effectively controlled an omental source. This case highlights the importance of considering timely surgical intervention as an option to treat refractory GI bleeding following PEG tube removal.</p>","PeriodicalId":15877,"journal":{"name":"Journal of Gastroenterology and Hepatology","volume":"39 S1","pages":"331-372"},"PeriodicalIF":3.4000,"publicationDate":"2024-09-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jgh.16708","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Gastroenterology and Hepatology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/jgh.16708","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
8
A rare lesion of the oesophagus: oesophageal submucosal gland duct adenoma
Gary Zhang1,2, Spiro Raftopoulos1,2,3 and Priyanthi Kumarasinghe1,2,3
1Sir Charles Gairdner Osborne Park Health Care Group, Perth, Australia;2The University of Western Australia, Perth, Australia;3Curtin University, Bentley, Australia
Introduction: Oesophageal submucosal gland duct adenomas (ESGDA) are a rare oesophageal lesion usually diagnosed in males 50-80 years of age presenting with abdominal pain or incidentally. Less than 20 cases of ESGDA have been reported in the literature, with two cases reporting incidental accompanying oesophageal squamous cell carcinoma and gastric adenocarcinoma, respectively.
Case report: A 68-year-old Caucasian man without other significant medical history presented with mild reflux symptoms. There were no associated alarm symptoms. He was a non-smoker and consumed up to 2 standard drinks of alcohol a day. Initial upper gastrointestinal endoscopy demonstrated a 10mm subepithelial lesion (SEL) at the gastroesophageal junction with normal overlying squamous mucosa and no evidence of reflux changes (figure 1). Pinch biopsies were acquired and reported as an inflammatory polyp with no evidence of dysplasia. The patient was referred for consideration of endoscopic removal following 8 weeks of high dose twice daily proton pump inhibitor therapy. On subsequent endoscopy, the SEL remained despite high dose PPI and therefore a decision was made for endoscopic removal via local excision using a band and ligation technique (figure 1A-C). The lesion was completely resected, retrieved, pinned and sent for pathological assessment. Histopathological assessment of the SEL demonstrated a predominantly submucosal lesion featuring localised hyperplastic and proliferated oesophageal glands and ducts without malignancy (figure 1D). With histochemical stains, the glandular epithelial cells showed diffuse cytoplasmic positivity with epithelial membrane antigen and CK7. Some basal cells showed a positive reaction with p63 and p40. There was no aberrant p53 over-expression or heightened ki-67 proliferation index. The lesion was consistent with an ESGDA. Endoscopic appearances at follow-up demonstrated a smooth, contracted scar (figure 1E).
17
Colonoscopy in octogenarians and older patients with 1L polyethylene glycol plus ascorbic acid bowel preparation in the real-world setting
Elena Perez-Arellano1, Salvador Machlab2, Miguel A Pantaleón3, Ricardo Gorjão4, Cátia Arieira5, Jose Cotter5, Vicente Lorenzo-Zúñiga6, Sarbelio Rodriguez Muñoz7, David Carral-Martínez8, Carmen Turbi9, Fatma Akriche10, José M Esteban11 and Katherine Davies12
1Hospital La Zarzuela, Madrid, Spain;2Hospital Parc Taulí de Sabadell, Sabadell, Spain;3Hospital del Mar, Barcelona, Spain;4Hospital C UF Descobertas, Lisbon, Portugal;5Hospital Senhora da Oliveira, Guimarães,, Portugal;6Hospital HM Sant Jordi, Barcelona, Spain;7Hospital Ruber Juan Bravo, Madrid, Spain;8Hospital San Rafael, A Coruña, Spain;9Norgine Medical Department, Spain;10Norgine Medical Affairs, Harefield, United Kingdom;11Hospital Clinico Universitario San Carlos, Madrid, Spain;12Norgine, Sydney, Australia
Background and Aim: Colonoscopy for colorectal cancer (CRC) detection in octogenarians is technically challenging due to bowel preparation difficulties in this population. While moderate or poor preparation quality were reported in 25% patients using large volume PEG [1], there is no published literature in octogenarians using validated cleansing scales. The aim of this study was to evaluate the colon cleansing effectiveness and safety of a contemporary bowel preparation, the 1L polyethylene glycol plus ascorbic acid (1L PEG+ASC) in octogenarians and older patients.
Methods: Post-hoc analysis of an observational, multicentre, retrospective real-world study. Outpatients aged ≥ 80 years, who received 1L PEG + ASC before undergoing colonoscopy in 8 centres in Spain and Portugal between July 2019 and September 2021 [2]. Cleansing quality was evaluated using the Boston Bowel Preparation Scale (BBPS). Adequate quality was defined as a BBPS score ≥6 with all segmental scores ≥2. High-quality cleansing was defined overall as a BBPS score ≥8, and segmentally as a BBPS score of 3. Caecal intubation rate (CIR), withdrawal time (WT) and polyp detection rate (PDR) were also assessed. Safety was assessed from recorded adverse events (AEs).
Results: A total of 423/13,169 patients (3.2%), 49.2% male were included. Mean age 83.5 years (range 80 to 95 years). Indication for colonoscopy was screening for CRC (14.4%), diagnostic (56.7%), follow-up (25.5%), or other (3.3%). The bowel preparation method was either as a split-dose (40.9%) or a same-day dose (59.1%) regimen. In total, 94.1% of patients completed the colonoscopy. Incomplete colonoscopy was reported in 5.9% of patients, including 1% due to poor preparation, 1.4% due to stenosing cancer, 1.2% due to technical difficulties, and 2.3% for other reasons. The CIR was 94.9%, the mean WT was 8.4 minutes, and the overall PDR was 45.6%. Cleansing outcomes are shown in Figure 1. The incidence of AEs was 4.5%, with dehydration (2.8%) and nausea (1.2%) being the most reported AEs. No severe AEs were reported.
References
1. Chatrenet, P, Friocourt, P, Ramain, JP, et al. Colonoscopy in the elderly: A study of 200 cases. Eur J Med1993; 2: 411–3.
2. López-Jamar, JME, et al. Bowel cleansing effectiveness and safety of 1L PEG + Asc in the real-world setting: Observational, retrospective, multicenter study of over 13000 patients. Endosc Int Open2023; 11(08): E785-E793.
24
Endoscopists’ knowledge, perceptions and attitudes towards the use of artificial intelligence in endoscopy: A systematic review
Nicholas Wan1,2, Celine Chan1, Jin Lin Tan1,2, Mohamed Asif Chinnaratha1,2 and Rajvinder Singh1,2
1Gastroenterology Department, Lyell McEwin Hospital, Adelaide, Australia;2Adelaide Medical School, University of Adelaide, Adelaide, Australia
Background and Aim: Artificial Intelligence (AI) is rapidly evolving in the field of gastrointestinal endoscopy. However, the prevailing perceptions and attitudes of endoscopists towards AI remain poorly understood. This review aims to provide a summary on the current views and perspectives covering the incorporation of AI into endoscopy, as well as to identify any obstacles hindering its adoption.
Methods: Electronic databases including MEDLINE, PubMed, and Scopus were searched from inception to 25th March 2024 to identify qualitative studies, such as questionnaires or surveys, conducted on endoscopists regarding the use of AI in endoscopy. The Joanna Briggs Institute critical appraisal checklist was used to assess study quality. Qualitative synthesis of included studies was conducted by employing thematic analysis classified into the following five domains: 1) Knowledge, and attitudes towards AI, 2) Perception on AI’s ability to improve accuracy and quality of endoscopy, 3) Impact of AI on endoscopists, 4) Impact of AI on patients and 5) Barriers towards the implementation of AI.
Results: Ten studies were included in this systematic review comprising of 1587 endoscopists across Europe (32.6%), North America (42.8%), and Asia (24.6%). Domain 1: Most endoscopists (69–100%) reported having basic knowledge of AI. Furthermore, the majority (79.5–87.5%) expressed interest and optimism regarding AI in endoscopy. Domain 2: Most respondents (62.5–97%) supported the notion that AI would positively impact endoscopic performance and quality. Domain 3: There were mixed perceptions regarding the extent of operator dependence on AI (6.2–62.8% agreement), and whether AI would prolong procedural time (21–81.3% in agreement). Most endoscopists (71–100%) disagreed that AI would replace them at work. Domain 4: A substantial proportion of respondents (81.3%) felt that AI would lead to an increase in the quality of patient care. Only a minority of endoscopists (6.2–24%) felt that AI could improve the patient-physician relationship and provide empathetic care. Domain 5: A significant proportion of endoscopists (75.2–91%) identified costs as potential barriers to the implementation of AI in endoscopy. Opinions on ethical concerns and the lack of regulation varied (12.5–100% and 35–88%, respectively), with many endoscopists feeling that there was need for clear guidelines and regulations when integrating AI into clinical practice.
31
Development of hepatic portal venous gas following percutaneous endoscopic gastrostomy – an ominous radiological sign?
Joel Thio
Department of Gastroenterology and Hepatology, Logan Hospital, Meadowbrook, Australia
Introduction: Percutaneous endoscopic gastrostomy (PEG) feeding is widely used to overcome barriers to nutrition in patients with impaired swallowing. Like any intervention, this procedure carries risks of complications. Hepatic portal venous gas (HPVG), a rare radiological entity usually seen as an ominous sign, has only been reported in five case reports to date following PEG insertion. The aim of this case report is to raise awareness of this rare complication following PEG insertion.
Conclusion: HPVG is a rare entity following PEG procedures, with only five case reports in the literature to date – two cases were managed conservatively with antibiotics with good outcomes, one case was managed conservatively without antibiotics with a good outcome, and two cases unfortunately died soon after from septic shock. If we include our case of death from likely intra-abdominal sepsis, this brings the mortality rate associated with findings of HPVG post-PEG insertion to 50%. This supports the increasing need for more data and vigilance of this radiological finding of HPVG following PEG procedures to help guide the course of care in these patients.
40
Over-the-scope clipping of a bleeding duodenal Dieulafoy lesion: a case report
Carl Cosgrave1, Zacchary Tamsett1,2, Eliza Flanagan1,3 and Neel Heerasing1,2
1Barwon Health, Geelong, Australia;2Deakin University, Geelong, Australia;3Monash University, Melbourne, Australia
Introduction: Dieulafoy lesions (DL) are enlarged submucosal blood vessels that bleed in the absence of abnormality such as ulcers or erosions1. They are a rare cause for obscure upper gastrointestinal bleeding (UGIB), accounting for 6% of non-variceal bleeding and 1-2% of all UGIB2. DL can occur at any age but most commonly present clinically in the sixth or seventh decade of life3. Approximately 70% are found in the proximal stomach, with 15% found in the duodenum2. We present a case of a large DL at the second-third (D2/D3) aspect of the duodenum, which made treatment with traditional measures of adrenaline and clipping particularly challenging. Over-the-scope clips have been demonstrated to be an effective means of managing patients with non-variceal UGIB4. Whilst using a colonic over-the-scope (OVESCOTM) clip in the duodenum is uncommon, the procedure was successful with no adverse outcomes.
Case report: An 89-year-old man underwent a gastroscopy to investigate recurrent melaena and profound iron deficiency anaemia. His medical history includes recurrent UGIB due to a suspected DL (previously managed with through-the scope clipping), atrial fibrillation (not on anticoagulation), ischemic heart disease and a transcatheter aortic valve implantation. His medications included pantoprazole, amlodipine, and furosemide. Urgent gastroscopy revealed an enlarged 7mm submucosal lesion on the medial floor of the D2/D3 with intermittent active arterial bleeding (Figure 1). Initial attempts with adrenaline injection and resolutionTM clips failed to achieve haemostasis. Due to the location of the lesion, the endoscope was switched to a paediatric colonoscope. The decision was made to proceed with over-the-scope clipping due to ongoing bleeding and a large underlying arterial pulsation. A 14mm colonic over-the-scope clip was used as a smaller size (11/12mm) over-the-scope clip was not readily available. The clip was placed over the bleeding point capturing the entire lesion (Figures 2 & 3). The lesion was observed for 5 minutes post-therapy with no further ooze noted. The patient's haemoglobin remained stable over the coming days with resolved melaena and he was discharged home.
2.
Nojkov, B, Cappell, M. Gastrointestinal bleeding from Dieulafoy’s lesion: clinical presentation, endoscopic findings, and endoscopic therapy. World J Gastrointest Endosc, 2015; 7(4): 295–307.
3.
Baxter, M, Aly, EH: Dieulafoy’s lesion: current trends in diagnosis and management. Ann R Coll Surg Engl2010; 92(7): 548–554.
4.
Qiu, J et al. Over-the-Scope Clip Applications as First Line Therapy in the Treatment of Upper Non-variceal Gastrointestinal Bleeding, Perforations and Fistulas. Front Med (Lausanne)2022; 9:753956.
72
Penetrating injury and retained toothpick fragment causing bleeding from oesophageal varix
Elaine Koh1, Vikram Rao1, Kim Hay Be1,2 and Leonardo Zorron Cheng Tao Pu1,2,3
1Department of Gastroenterology, Peninsula Health, Australia;2Department of Gastroenterology, Austin Health, Australia;3Department of Surgery, University of Melbourne, Melbourne, Australia
Introduction: A foreign body (FB) lodged within the gastrointestinal tract is a frequent presenting complaint amongst patients presenting to the emergency department. Despite the common nature of this presentation, there are no descriptions of cases where a FB has become embedded within an oesophageal varix. In this case report, we describe a cirrhotic patient presenting with haematemesis, with the eventual diagnosis of a toothpick fragment lodged within an oesophageal varix.
Case report: A 50-year-old man with alcohol-related Child-Pugh C liver cirrhosis presented with a 1-day history of epigastric pain and two episodes of haematemesis. This was in the setting of recently banded grade II oesophageal varices and a pre-emptive transjugular intrahepatic portosystemic shunt (TIPS) insertion a month prior. His haemoglobin was 101g/L on presentation, with no associated urea rise. An abdominopelvic CT scan demonstrated a patent TIPS. Given the patient’s risk factors and concerning history, an urgent gastroscopy was performed. Grade I varices were found in the lower third of the oesophagus, with an area of yellow discoloration noted (Figure 1A). On closer inspection, this appeared to be a solid FB embedded within an oesophageal varix. A single band was applied to the culprit varix, causing the FB to protrude into the lumen (Figure 1B). Given haemostasis had been achieved, the FB was not removed due to the risk of precipitating further bleeding. On further assessment of this patient’s history, this FB was deemed likely to be a fragment of a toothpick accidentally swallowed by the patient while intoxicated. The patient remained stable overnight and was discharged the following day. Though he had a subsequent alcohol-related presentation to our centre, he has yet to attend a follow-up gastroscopy or outpatient clinic appointments despite multiple attempts.
78
Stuck in transit: Food retention in ERCP for liver transplant patients
Vicki McGarrigle, Marios Efthymiou, Rhys Vaughan and Sujievvan Chandran
Austin Health, Melbourne, Australia
Introduction: Food retention during Endoscopic Retrograde Cholangiopancreatography (ERCP) poses significant risks such as aspiration and can lead to procedure delays. Food retention following fasting over four hours is associated with gastroparesis. Liver transplant patients have increased rates of diabetes, which can lead to gastroparesis. Solid organ transplant recipients are known to have higher rates of gastroparesis.
Methods: A retrospective analysis was performed on patients who underwent ERCP between 2022 and 2024. Data from 525 procedures were collected to date, including variables such as food retention, liver transplant, diabetes, and gastric surgery.
Results: A total of 525 ERCPs were analysed (mean age 62 years). Food was present in 3% of total procedures. Thirty-one percent of ERCPs were in liver transplant patients. Twenty-four percent of procedures were in diabetic patients. A significant association was observed between food retention and liver transplant recipients using Pearson’s Chi-squared test (p=0.03). However, there was no association using logistic regression analysis. Age was inversely associated with food retention.
Discussion: The results indicate a higher likelihood of food retention in liver transplant patients during ERCP, although this association was not held with logistic regression analysis. Understanding the factors that cause food retention during ERCP is crucial in determining the need for pre-procedure prokinetics in high-risk groups. To achieve this, we plan to collect further data and increase our sample size to better identify the factors leading to food retention. This data is essential for optimal patient preparation, reducing procedure delays, and improving patient outcomes.
81
Safety of endoscopist directed procedural sedation in patients with severe obesity
Raymond Lewandowski, Montri Gururatsakul, Keith Brick and Peter Boyd
Cairns Base Hospital, Cairns, Australia
Background and Aim: According to Australian Institute of Health and Welfare data, 33% of men and 30% of women are living with obesity and 12% are living with severe obesity, which is defined as having a BMI of 35 or more. Presentations for endoscopic procedures in this population will increase as well. Endoscopist directed sedation has been demonstrated to be safe in low-risk populations. The aim of this review is to determine whether this safety expectation can be expanded to this high-risk group.
Methods: An audit was conducted of patients presenting to our unit for endoscopic procedures between January 2022 and April 2023. Outcomes were evaluated based on model of sedation, BMI and ASA category and complications related to sedation.
Results: 904 endoscopic procedures were performed in our unit on patients with a BMI ≥35 during the time covered by this review including 57 patients with BMI ≥50. 805 (89%) received endoscopist directed sedation, the remaining 99 had sedation provided by an anaesthetic team. The majority of patients in the endoscopist directed group received propofol and midazolam for sedation. There were a total of 4 complications related to sedation in the endoscopist directed group representing 0.49% of patients. Complications included two episodes of bradycardia, one laryngospasm and one transient hypoxic episode. Only one complication, laryngospasm, led to the discontinuation of the procedure.
Conclusion: Endoscopist directed sedation is a safe model for sedation in endoscopic procedures performed in patients with BMI ≥35.
89
Iron deficiency without anaemia: to scope or not to scope?
Zainul Azhar and Rozemary Karamatic
Townsville University Hospital, Townsville, Australia
Background and Aim: Iron deficiency is a common indication for endoscopic assessment, with endoscopy guidelines available to guide the decision to refer. Commonly, patients will have iron deficiency without anaemia. There remains a paucity of evidence for proceeding to endoscopy in iron deficient patients without anaemia. The research aims to explore endoscopic yield of non-anaemic iron deficient (NAID) patients, comparing their counterparts with iron deficiency anaemia (IDA)
Methods: We conducted a retrospective study of 421 patients with iron deficiency referred for endoscopic assessment to a regional tertiary hospital in Queensland from 2022 to 2023. Inclusion criteria is patients ≥ 15 years old and iron deficiency defined as respective laboratory parameters at time of referral. Outcome measures include age, premenopausal status, use of prior iron supplementation, presence and nature of clinically significant lesions causing iron deficiency, malignancy rate, use of antiplatelet and anticoagulants. Multiple logistic regression was used to determine predictors of malignancy.
Results: There were significantly lower rates of malignancy in the NAID arm compared to IDA arm (7.61%, 2.68%, p 0.02). In subgroup analyses, non-anaemia females (NAF) had lower malignancy rates than the anaemia group, among pre-menopausal (PRMF) (1.25% vs 2.94%, p 0.53) and post-menopausal (POMF) group (1.56% vs 7.02%, p = 0.13) respectively. Among non-anaemic females, malignancy rate showed no difference between PRMF and POMF (1.56% vs 1.25%, p 0.87). Significant predictors of malignancy were anaemia (OR 2.97, p 0.03) and presence of overt bleeding (OR 2.91, p 0.03). There were also significantly lower rates of non-neoplastic causes in NAID arm compared to IDA arm (56.70% vs 72.08%, p < 0.01). The most common finding in esophagogastroduodenoscopy in NAID group is Helicobacter pylori gastritis (8.48%) while gastric or duodenal erosions is the most common in the IDA group (7.61%). For colonoscopy, the most common findings in the NAID and IDA group is haemorrhoids (4.91%) and colonic angioectasias (4.59%) respectively.
Conclusion: Our evidence demonstrates that non-anaemic iron deficiency confers a lower risk of gastrointestinal malignancy and detection of non-neoplastic pathology compared to iron deficiency anaemia. Further studies with larger sample sizes are needed to show statistical significance. The decision to proceed or not to proceed to endoscopic assessment among low-risk individuals and rationalize the use of a limited resource can be informed by these results.
91
Use of artificial intelligence improves colonoscopy performance in adenoma detection: A systematic review and meta-analysis
Jonathan Makar1, Jonathan Abdelmalak2,3,4, Danny Con1,2, Bilal Hafeez1 and Mayur Garg1,5
1The University of Melbourne, Melbourne, Australia;2Department of Gastroenterology, Austin Hospital, Melbourne, Australia;3Department of Gastroenterology, Alfred Hospital, Melbourne, Australia;4Central Clinical School, Monash University, Melbourne, Australia;5Department of Gastroenterology, Northern Health, Melbourne, Australia
Background and Aim: Artificial intelligence (AI) is increasingly used to improve adenoma detection during colonoscopy. This meta-analysis aimed to provide an updated evaluation of computer-aided detection (CADe) systems and their impact on key colonoscopy quality indicators.
Methods: We searched the Embase, PubMed and MEDLINE databases from inception until February 15, 2024, for randomised control trials (RCTs) comparing the performance CADe systems with routine unassisted colonoscopy in the detection of colorectal adenomas.
Results: 28 RCTs were selected for inclusion comprising 23861 participants. Random-effects meta-analysis demonstrated a significant 20% increase in adenoma detection rate (ADR, RR 1.20, 95% CI 1.14-1.27, p < 0.01) and 55% decrease in adenoma miss rate (AMR, RR 0.45, 95% CI 0.37-0.54, p < 0.01) with AI-assisted colonoscopy. Subgroup analyses revealed CADe-associated benefits for ADR persisted when considering only expert endoscopists (RR 1.19, 95% CI 1.11-1.27, p < 0.001) and remained for all investigated CADe systems and in both hospital and day-procedure settings. CADe use also significantly increased adenomas per colonoscopy (weighted mean difference 0.21, 95% CI 0.14-0.29, p < 0.01). Subgroup analysis of 8 studies reporting total adenomas categorised by size showed a significant benefit with regards to diminutive lesion detection (IRR 1.46, 95% CI 1.19-1.80, p< 0·001) for the CADe supported study arms, with a non-significant trend towards improved detection associated with small (IRR 1.11, 95% CI 0.94-1.31, p = 0.20) and large polyps (IRR 1.24, 95% CI 0.94-1.62, p = 0.12). Sessile serrated lesion detection (RR 1.10, 95% CI 0.93-1.30, p = 0.27) or miss rates (RR 0.44, 95% CI 0.16-1.19, p = 0.11) were not improved when all CADe systems were combined. There was an average 0.15 minute prolongation of withdrawal time with AI-assisted colonoscopy (weighted mean difference 0.15, 95% CI 0.04-0.25, p = 0.01).
95
Small intestinal bacterial overgrowth as assessed by breath testing: a prospective evaluation to the gold standard aspirate
Ayesha Shah1,2, Teressa Hansen1, Thomas Fairlie1,2, Natasha Koloski1,2,3, Mike Jones4 and Gerald Holtmann1,2
1Princess Alexandra Hospital, Metro South Health, Brisbane, Australia;2The University of Queensland, Brisbane, Australia;3The University of Newcastle, Newcastle, Australia;4Macquarie University, Sydney, Australia
Background: Small intestinal bacterial overgrowth (SIBO) is defined as the presence of excessive and abnormal types of bacteria in the small intestine. SIBO has been linked to several gastrointestinal and extraintestinal diseases. While small bowel aspiration and culture is the accepted gold standard for diagnosis, glucose breath testing (GBT) is widely used in the routine clinical setting. We aimed to prospectively compare in the routine clinical setting results of the GBT with duodenal aspirate and culture for diagnosing SIBO.
Methods: We prospectively recruited patients between 2019-2023 with clinical suspicion of SIBO who underwent GBT as well as a gastroscopy and aspirate collected from the third part of the duodenum and cultured utilizing previously published methods (1). We calculated the sensitivity, specificity, positive and negative predictive value for the GBT against the duodenal aspirate and culture.
Results: The final dataset included 131 patients with suspected SIBO who underwent GBT and had duodenal aspirate collected. The cohort had an average age of 43.2 ±15.6 years, with 73% female. Based upon duodenal aspirates and culture, 51 (38.9%, 95% CI 30.5-47.8) patients were positive for SIBO, at a cut off threshold of ≥103 colony forming units of bacteria/ml (Table 1). In contrast based upon the GBT, 13/131 (9.9%, 95% CI 5.4-16.4) tested positive for SIBO. Compared with the reference standard of small bowel aspirate and culture, GBT had accuracy of 55.7% (sensitivity 5.9%, specificity 87.5%).
Conclusion: The results of this large prospective single centre study shows that GBT has poor sensitivity but good specificity when compared to duodenal aspirate and culture for diagnosing SIBO. However, there is lack of universal acceptance and validation of small bowel aspirate and culture as the gold standard for diagnosing SIBO. This highlights the urgent need to develop better validated diagnostic tests for SIBO in routine clinical settings.
Reference
1. Shah, A, Talley, NJ, Koloski, N, Macdonald, GA, Kendall, BJ, Shanahan, ER, et al. Duodenal bacterial load as determined by quantitative polymerase chain reaction in asymptomatic controls, functional gastrointestinal disorders and inflammatory bowel disease. Alimentary pharmacology & therapeutics.2020; 52(1): 155-67.
104
The effect of computer aided detection system availability on polyp detection during colonoscopy in a real-life scenario
Vikram Rao1, Gordon Chen1, Elaine Koh1, Sheng Wei Lo1, Ibrahim Al Ansari2, Josephine Wanandi1, Brian Chow1, Marcus Robertson1, Leonardo Zorron Cheng Tao Pu1,3,4 and Kim Hay Be1
1Department of Gastroenterology, Peninsula Health, Melbourne, Australia;2Department of Medicine, Monash University, Melbourne, Australia;3Department of Gastroenterology, Austin Health, Melbourne, Australia;4Department of Surgery, University of Melbourne, Melbourne, Australia
Background and Aim: One of colonoscopy's primary aims is to detect and remove precancerous polyps. Several studies have demonstrated that the use of computer aided detection (CADe) technology improves metrics such as the adenoma detection rate (ADR). Implementation of CADe is not yet standard practice across endoscopy centres, and even when available, uptake is variable amongst endoscopists. This makes it questionable if the results from controlled studies can be extrapolated to the real-world scenario. This study assessed the real-world effect of CADe availability on ADR.
Methods: A single-centre retrospective observational study was performed at a metropolitan tertiary centre following the introduction of the Olympus Endo-AID module in July 2023. All colonoscopy reports generated through the network’s reporting software (Endobase) were examined 7-months prior to, and 7-months after the introduction of CADe. Inclusion criteria were: i) patients aged ≥ 40 years, and ii) colonoscopies performed for screening or surveillance. Endoscopists who did not perform eligible colonoscopies in both periods of the study were excluded. Emergency colonoscopies (e.g. for acute colitis, foreign body extraction or suspected active bleeding) were excluded. The frequency of use of CADe by each endoscopist was assessed as: i) Uses CADe for 100% procedures; ii) uses CADe for ≥ 50% procedures; iii) uses CADe for < 50% of the time; or iv) 0% CADe use. The primary outcome was the comparison of ADR before and after introduction of CADe.
Results: Seven endoscopists performed a total of 636 eligible pre-CADe and 386 post-CADe colonoscopies during the study period. No statistically significant differences in baseline pre- and post-CADe procedure data were identified regarding age, gender, procedure indication, bowel preparation score or the endoscopist’s specialty. ADR was significantly improved for endoscopists with a baseline pre-CADe ADR between 25-50%, regardless of whether it was used for every procedure. This effect was not seen for endoscopists with an ADR >50% at baseline pre-CADe, even though for this group CADe use was 100%. Only one endoscopist with a baseline ADR of less than 25% did not show improvement, despite CADe use for more than 75% of the time. However, this endoscopist had only 10% of all their colonoscopies for the study period done after introduction of CAD.
Conclusion: Availability of CADe significantly improved ADR for endoscopists with baseline ADR 25-50%, even if not being used consistently for all procedures. The single endoscopist in this group that did not show improvement is likely due to the low numbers of post-CADe eligible colonoscopies within the study period. The observed effect was not seen in those with a baseline ADR pre-CADe > 50%. These results support the introduction of CADe even if it is not used for every colonoscopy by all endoscopists.
118
EPIC: A novel scoring system to identify patients likely to benefit from extended bowel preparation at index colonoscopy
Matthew Smale and Lok Lee and Jeremy Humphris
Wollongong Hospital, Wollongong, Australia
Background: Despite concerted intervention, bowel preparation remains inadequate in 18-35% of colonoscopies, resulting in reduced caecal intubation rate and adenoma detection rate, and increased procedure time and adverse events.1 For the patient, this increases the risk of delayed diagnosis and disease progression. For the healthcare system, it increases the need for repeat colonoscopy.2 Several studies have identified risk factors for inadequate bowel preparation. Four demonstrate predictive models for identifying patients at risk of inadequate bowel preparation, including Dik et al (2015).3 No predictive model, however, can be generalised to patients at their index colonoscopy, where the benefit is arguably greatest.
Aim: We designed and validated a novel scoring system,”EPIC”, that identifies patients at risk of inadequate bowel preparation using established patient risk factors at their index colonoscopy.
Methods: Risk factors for EPIC were taken from a systematic review and meta-analysis by Mahmood et al (2018)1, which reviewed 24 studies and therein the outcomes of 49,868 colonoscopies. Risk factors and associated odds ratios (ORs) were cirrhosis (OR 0.49), stroke (OR 0.51), tricyclic antidepressant use (OR 0.51), diabetes mellitus (OR 0.58), hypertension (OR 0.58), narcotic use (OR 0.59), history of constipation (OR 0.61) and male gender (OR 0.85). We assigned points based on their ORs in a similar fashion to Dik et al (2015). Three points were assigned to cirrhosis, stroke and TCA use; two points to diabetes mellitus, hypertension, narcotic use and history of constipation; one point to male gender. To validate the system, we collected retrospective data for 500 index colonoscopies from our hospital’s endoscopy database. This included patient age, gender, BBPS and the aforementioned risk factors. ASA score and history of previous abdominal surgery were also collected to allow comparison of the EPIC scoring system with Dik et al (2015).
Results: The median age was 60 years (253 patients male, 247 female). 13.4% had inadequate bowel preparation (total BBPS < 6 or individual segment of 1). Using EPIC, a score of 3 or more was the optimal threshold for predicting inadequate bowel preparation (sensitivity 58%, specificity 71%, PPV 0.24, NPV 0.92). Comparatively, using the Dik et al system, a score of 2 or more was the optimal threshold (sensitivity 36%, specificity 88%, PPV 0.32, NPV 0.90). A ROC analysis found a similar area under the ROC curve of 0.67 (p<0.002, standard error = .04) for each system (Figure 1). However, higher NPV and sensitivity using EPIC renders it a stronger performing scoring system in this population for screening. A binary logistical regression suggested a score of 3 or more was associated with 3.54 times greater odds of inadequate bowel preparation compared to a score of 2 or less, p < 0.001. A Mann-Whitney U test suggested a score of 3 or more was associated with a mean BBPS 2.17 points (out of 9) lower compared to a score of 2 or less (p=.03).
References
134
Comparison of artificial intelligence enhanced versus conventional reading in small bowel capsule endoscopy: a multi-centre australia based study
Phillip Leaver1,2, Fiona Tudehope1, Kevin Choi3, Sneha John4, Aman Yadav4, Arthur J Kaffes3 and Robert B Feller1,2
1Department of Gastroenterology & Hepatology, St Vincent’s Hospital, Sydney, Australia;2St Vincent’s Clinical School, The University of New South Wales, Sydney, Australia;3AW Morrow Gastroenterology and Liver Centre, Royal Prince Alfred Hospital, Sydney, Australia;4Department of Gastroenterology, Gold Coast University Hospital, Gold Coast, Australia
Background and Aim: Capsule endoscopy is a proven, useful, minimally invasive tool for the investigation of small bowel pathology, particularly suspected small bowel bleeding. Important practical limitations include physician reading times and the risk of reader fatigue. The advent of artificial intelligence (AI) assisted reading software has the potential to significantly reduce reading time without compromising efficacy. Our aim was to compare conventional and AI assisted reading modes with respect to reading times and findings, from studies performed at a number of Tertiary Australian sites.
Methods: 30 patients who underwent routine capsule endoscopy with the OMOM® capsule for investigation of obscure gastrointestinal bleeding were retrospectively analysed across three tertiary Australian hospitals. Included patients were over 18-years-old, had suspected overt or occult small bowel bleeding and no known small bowel strictures or Peutz-Jegher syndrome. OMOM® capsule ingestion and post-ingestion protocol were as per standard method. A conventional read (CR) at a frame rate of 12 frames per second was conducted by an experienced capsule endoscopist. The AI enhanced mode (Smart scan-assisted read- SSAR®) was then used for a second read. Comparison was made between the two in the following domains: reading time, reporting time, total number of findings, number of significant findings (using the Sarin classification: P0 insignificant, P1 uncertain, P2 definite). Statistical significance was assessed using the Student t-test.
Results: All thirty patients were included in data analysis. Mean reading time by CR was 29.26 minutes vs 2.96 minutes by SSAR (p<.001). Mean reporting time showed no significant difference (p= 0.654). Comparison of capsule findings across all patients – P2 lesions: CR 57 vs 63 by SSAR (p=0.264), P1 lesions: CR identified 109 vs 70 by SSAR (p=0.032), P0 lesions: CR identified 32 vs 22 by SSAR (p=0.057). The most frequent P2 lesions were angioectasias (n=35/42) followed by ulcers (n=22/20), blood (n=13/13) and tumours (n=4/6). The most common P1 lesions were red spots (n=83/45).
143
Quality improvement using an electronic referral pathway for endoscopic procedures
Brigid Pinnuck1, Kirri Riley2, Sharon Gillespie3, Sharon Killin3, Nicola Mullaney3, Sarah Mendoza4, Amy Schafer2 and Jane Andrews3,5
1Department of Gastroenterology and Hepatology, Royal Adelaide Hospital, Adelaide, Australia;2Surgery Program, Central Adelaide Local Health Network, Adelaide, Australia;3Central Adelaide Local Health Network, Adelaide, Australia;4Gastrointestinal Investigation Unit, Royal Adelaide Hospital, Adelaide, Australia;5Faculty of Health Sciences, University of Adelaide, Adelaide, Australia
Background: Electronic referrals (e-referrals) for endoscopic procedures are becoming the standard of care. However, many healthcare organisations have more than one entry point for referrals, and this leads to unwarranted variation in triage and waiting times for those referred. Accurate triage against accepted indications is fundamental to delivering a quality, safe endoscopic service. Processing and managing large volumes of referrals also presents an administrative challenge, which digital platforms can support by ensuring no loss of referrals, booking in turn (by clinical urgency) and visibility along with audit.
Methods: A consultation and co-design process was run over 18 months examining routine ambulatory endoscopic referrals across 2 sites in one health network. We identified referral entry points and necessary processes. A new agreed process was designed to harmonise practices across sites and reduce processing steps. To manage this new process, a digital platform (Novari ATC™was used. The new dual site, single pathway went live in October 2023. Data pre and post implementation were reviewed.
Results: Since October 2023, 6,911 internal and external referrals were received, of which 5,799 were new referrals (n=558 staged). Of new referrals, colonoscopy (52.4%, n=3,036) was the most commonly referred procedure, followed by endoscopy (24.1%, n=1,399), colonoscopy and endoscopy (18.4%, n=1,066), flexible sigmoidoscopy (4.9%, n= 287) and endoscopy and flexible sigmoidoscopy (0.2%, n=11). To date, 3,609 of the new referrals have exited the pathway; 999 without a procedure, 2,488 were treated/scoped and 122 were diverted to outpatient department (OPD). Since going live, compared to May to October 2023, the number of weekly OPD additions for both colorectal and gastroenterology units decreased (colorectal by 45.9%, gastroenterology by 43.2%, and combined overall by 44.2%).
Conclusion: Creating a single point for receipt, triage, assessment and scheduling of routine ambulatory endoscopic referrals in a digital platform has proved possible across 2 acute care sites. It has enabled us to better see and plan our work and to report on processes and outcomes transparently. It allows for these procedures to be delivered more consistently and reliably and to ensure that each person is verified to receive evidence-based guidelines at pathway exit, which will reduce the future number of inappropriate referrals via consumer and GP education. Significant savings in additions to OPD bookings have also been demonstrated, meaning that, people requiring OPD will have less waiting time and those where a procedure is clearly indicated can progress more rapidly without waiting for OPD.
Average weekly OPD additions before and after the e-referral pathway went live
171
Dual snare endoscopic extraction of a gastric foreign body using a dual-channel endoscope: case report
Amitjeet Singh, Edward Young and Rajvinder Singh
Department of Gastroenterology, Lyell McEwin Hospital, Adelaide, Australia
Introduction: Foreign body ingestions are rare but can pose serious risks. Most pass naturally, but 10-20% require endoscopic removal, and 1% need surgery. Ingested foreign bodies can include organic material, such as food boluses, or non-organic objects, such as coins, toys, magnets or batteries. Foreign bodies are commonly removed endoscopically using forceps, snares, baskets and nets. The physical characteristics of ingested objects greatly influence the available techniques for safe and atraumatic endoscopic retrieval. Long and pointed foreign objects in the stomach are challenging to remove endoscopically and can cause complications such as tears or even perforation. The removal of long and sharp foreign objects has previously been described using a dual-snare technique using two endoscopes either simultaneously or successively. We present a novel case highlighting the use of dual snares with a dual-channel endoscope to safely manoeuvre a gastric foreign body using a push-pull technique.
Case report: A 16-year-old female with a history of anxiety and depression had purposefully ingested a cigarette lighter three weeks prior to presentation. She presented to the hospital due to ongoing abdominal pain over two days duration. There were no significant findings on clinical examination, and laboratory investigations were unremarkable. An X-ray of the patient's abdomen showed a radiopaque foreign body in the left upper quadrant of the abdomen, likely within the gastric body. At endoscopy, a single cigarette lighter was in the gastric body with the metal cap removed, exposing a sharp plastic edge. Initially, grasping forceps were used but these would not capture the lighter adequately to traverse the lower oesophageal sphincter. A single snare was used, but this positioned the lighter perpendicular to the oesophageal lumen when the snare was tightened, which would have made retrieval dangerous. An attempt with an overtube was not attempted as the diameter of the object was too large and using a Roth Net was not attempted as it would not allow for appropriate orientation and could have led to difficulties in releasing the lighter. A dual-channel gastroscope was then used, facilitating the careful positioning of the lighter using two snares. One snare was placed over the rounded edge of the lighter, which was positioned cranially, while the second snare captured the sharp edge of the lighter and was positioned caudally using a push-pull technique (figure). The lighter could then be gradually pulled through the gastroesophageal junction and out of the mouth without complication. After removing the lighter, the scope was re-advanced, and there was no significant trauma.
Discussion: This case demonstrates the use of dual snares through a dual-channel endoscope to successfully remove a long and sharp object from the stomach using a push-pull technique. Procedural challenges to removing such an object involve positioning the blunt end proximally to prevent perforation or impaction during extraction, orienting the object's long axis in the extraction line and applying traction to the foreign body without losing traction. The use of a push-pull technique has previously been described with other endoscopic accessories (balloons and snares); however, to our knowledge, it has not previously been described using dual snares with a dual-channel endoscope.
192
Changing aetiology and demographics of patients presenting with upper gastrointestinal bleeding at a tertiary hospital over a decade
Aparna Morgan, Deniz Tuncer, Nirosha Pragash, Tharusha Dadallage, Angana Bajracharya, Leonardo Zorron Cheng Tao Pu and Richard La Nauze
Peninsula Health, Frankston, Australia
Background and Aim: Upper gastrointestinal bleeding (UGIB) is a common and potentially life-threatening condition presenting to emergency departments worldwide. Anecdotally, the incidence of UGIB seems to have remained stable over the years, however the aetiology and demographics of patients have thought to have changed. In addition, over the last 10 years, novel endoscopic interventions have been developed to manage UGIB and presumably these have decreased rebleed and mortality rates. There are no recent studies validating these observations, especially in the Australian population. The aim of this retrospective audit is to compare the aetiology, demographics, management and outcomes of patients presenting with UGIB in the year 2012 compared to 2022. Being able to understand these changes can improve patient outcomes by informing clinical decision making and optimising healthcare resources.
Methods: This study is a retrospective cohort study using electronic medical records to identify adult patients who presented with UGIB to a large tertiary hospital from 1/1/2012 to 31/12/2012 and the same period in 2022. Patients were identified using ICD-10 codes. Patients found to have a lower gastrointestinal bleed as the cause of the presentation during inpatient investigations, and patients that were discharged without having a gastroscopy, were excluded.
Results: There were coincidentally exactly 161 patients who presented with UGIB in both 2012 and 2022. The average age of patients presenting with UGIB in 2012 was 69 years-old compared to 73 years-old in 2022, p=0.03. In 2012, 45% of patients had one or more comorbidities (liver disease, heart failure, ischaemic heart disease, chronic kidney disease or malignancy); this increased to 57% patients in 2022, p=0.03. There was also an increase in anticoagulation use in 2022 compared to 2012, (50 vs 17 patients, p <0.001). This was driven by an increase in direct-acting oral anticoagulation (DOAC) use, (39 vs 4 patients, p<0.0001) while Warfarin use remained the same (13 vs 9 patients, p=0.39). There was no difference in gender or rates of cancer. The rate of peptic ulcer disease as the primary aetiology and NSAID/Aspirin/PPI use, as well as incidence of H. Pylori, were similar. However, there was an increase in variceal bleeding in 2022 compared to 2012 (17 vs 4 patients, p<0.01). Endoscopic intervention also increased in 2022 compared to 2012. 21 patients underwent endoscopic intervention for UGI bleed in 2012 compared to 44 patients in 2022, p<0.001. There was no difference between rates of rebleeding, mortality or length of hospital stay.
Conclusion: At our institution, aetiology and intervention for UGIB patients has changed between 2012 and 2022, now with increasing age, more comorbidities and anticoagulation use. Rates of peptic ulcer bleeds have remained the same but variceal bleeding has increased. Despite the increase in endoscopic intervention options, the rates of rebleed, mortality and length of hospital stay have remained the same. Further multi-centre studies are needed to validate these findings.
194
Effect of artificial intelligence on adenoma and polyp detection rate in a real-world, non-randomized setting
Jihan Harki1,2,3, Timothy O'Sullivan2,3, Kimberley Ryan2, Mehul Lamba2,3, Paris Hoey2, Florian Grimpen2, Enoka Gonsalkorala2,3, Stacey Llewellyn4, Katherine Hanigan2,3 and Mark Appleyard2,3
1Haga Ziekenhuis, The Hague, The Netherlands;2Royal Brisbane and Women's Hospital, Brisbane, Australia;3Surgical, Treatment and Rehabilitation Service, Brisbane, Australia;4QIMR Berghofer Medical Research Institute, Brisbane, Australia
Background and Aim: The benefit of computer-assisted detection systems (CADe) has been evaluated in several randomized controlled trials (RCTs) showing improved adenoma detection rate (ADR) (1-3). However, the generalizability of these studies is questioned as these studies are performed in highly controlled setting and thus not represent a real-world clinical setting (4). It is also believed that the increase in ADR is mainly observed in lower detector endoscopists (5, 6). We aimed to evaluate the effect of CADe-assisted colonoscopy on ADR in an actual clinical setting in a high-volume, non-tertiary endoscopy centre with high detector endoscopists.
Methods: A single-centre, observational study was conducted on all patients undergoing colonoscopy due to symptoms of colorectal cancer (CRC), screening colonoscopies for CRC, post-polypectomy surveillance, or colonoscopy due to positive results from a fecal immunochemical test between March 2023 to October 2023. Colonoscopies were performed by 19 experienced endoscopists using the validated CADe system that allows for real-time image analysis. Historical procedural data regarding colonoscopies were obtained up to 10 months before the start of the study and were compared to the CADe-assisted colonoscopies in a 2:1 fashion. The primary outcome was the ADR. The secondary outcomes were polyp detection rate (PDR), advanced adenoma detection rate (AADR), serrated polyp detection rate (SDR) and mean number of polyps and adenomas per colonoscopy. Data were analyzed using logistic mixed effects models expressed as Odds ratio (OR) or Incidence rate ratio (IRR) with a 95% confidence interval (CI).
Results: A total of 7444 colonoscopies were performed. ADR was significantly higher in the CADe-assisted colonoscopy group (50.7%) than in the control group (45.0%) (OR 1.26; 95% CI 1.13-1.41; p<0.001). The PDR was also significantly higher (67.3% vs 62.2%, OR 1.25; 95% CI 1.12-1.41; p<0.001) as was the advanced adenoma detection rate (AADR) (8.0% vs 6.5%, OR 1.26; 95% CI 1.07-1.49; p=0.007). The mean number of polyps per colonoscopy was significantly higher in the CADe group than in the standard group (1.78 vs 1.59, IRR 1.12, 95% CI 1.07-1.17; p<0.001) as was the mean number of adenomas per colonoscopy (0.82 vs 0.68, IRR 1.19; 95% CI 1.1.12-1.27; p<0.001).
215
Enhancing access to gastrointestinal endoscopy: a mixed methods evaluation of the endoscopist directed nurse-administered propofol sedation (EDNAPS) model
Ameya Godambe1, Elizabeth Watson1, Rhian Jones2, Angela Carberry2 and James O'Beirne1
1Sunshine Coast University Hospital, Birtinya, Australia;2Sunshine Coast Health Institute, Birtinya, Australia
Background and Aim: Many hospital and health services are experiencing increasing demand for diagnostic procedures such as colonoscopy. Increasing demand for services coincides with a national health workforce shortage felt most acutely in non-metropolitan areas, potentially leading to inequity of access to diagnostic tests needed to exclude serious conditions like cancer. Current delivery of endoscopy services is heavily reliant on sedation delivered by Anaesthetists. Expansion of access to endoscopy by flexible models of endoscopy delivery without reliance on anaesthetists have been proven to be safe and effective nationally and internationally. One such model is Endoscopist Directed Nurse-Administered Propofol Sedation (EDNAPS). We have implemented the EDNAPS model at our health service and through a comprehensive evaluation methodology, including patient data analysis, consumer surveys, and clinician feedback, the project sought to determine the value and benefits of the EDNAPS model for low-risk gastrointestinal endoscopy procedures.
Methods: A mixed-method evaluation approach was adopted, incorporating both quantitative and qualitative data. Procedural data was collected from hospital electronic medical records and surveys were disseminated to collect patient and clinician experience measures.
Results: A total of 120 EDNAPS procedures (all colonoscopy) have been performed to date. Analysis of post-anaesthesia care unit (PACU) recovery times revealed a statistically significant reduction for EDNAPS patients (median = 18 minutes) when compared to matched control patients (median = 24 minutes, p<0.001). Mean withdrawal time (13 minutes vs 16 minutes) and mean total procedure time (22 minutes vs 23 minutes) were not significantly different between EDNAPS patients and controls. There were no significant differences in adenoma detection rate (50% vs 49%) or sessile lesion detection rate (18% vs 27%) between EDNAPS procedures and controls. The patient experience surveys resulted in 22 EDNAPS and 26 control responses, being 19% and 22% respective recruitment rates. Most respondents from both groups (EDNAPS 77%, Controls 85%) rated the care that they had received as “very good”. Overall, patients felt that they were involved in decisions about their care and treatment (EDNAPS, 95%; Controls, 96%), had their procedure as soon as necessary (EDNAPS, 77%; Controls, 73%), were provided with materials that prepared them for their procedure (EDNAPS, 86%; Controls, 73%), and had an opportunity to ask the healthcare professional questions about the procedure (EDNAPS, 95%; Controls, 69%). No adverse patient outcomes, including hospital admissions following procedure, emergency department presentations within 72 hours, or mortality, were reported among EDNAPS patients. This indicates the safety and effectiveness of the EDNAPS model for eligible patients. The staff experiences survey had a total of eight responses (62% recruitment rate), covering a range of staff members from different professional streams, including nursing, medical and administration. Staff involved in EDNAPS procedures reported increased confidence and competence, attributing this to translational simulation exercises. These exercises facilitated a smooth implementation process and contributed to the successful adoption of the new model of care.
Conclusion: The EDNAPS model has demonstrated its potential as a safe and efficient alternative for low-risk gastrointestinal endoscopic procedures at our health service. Reduced recovery times and high patient satisfaction indicate its efficacy in improving service delivery. Further optimization of training and procedural logistics is recommended to address clinician concerns and enhance the model’s sustainability. The findings support the broader adoption of EDNAPS within the public health sector.
218
Consumer acceptability of a novel point-of-care faecal immunochemical test
Alicia Dallisson1, Ms Geraldine Laven-law1, Robert Le Blanc2, Graeme Young1, Charles Cock1,3 and Erin Symonds1,3
1Flinders University, College of Medicine and Public Health, Flinders Health and Medical Research Institute, Adelaide, Australia;2Health First Systems Ltd, Harrow, United Kingdom;3Department of Gastroenterology and Hepatology, Flinders Medical Centre, Southern Adelaide Local Health Network, Adelaide, Australia
Background and Aim: Colorectal cancer (CRC) screening with the faecal immunochemical test (FIT) has proven effectiveness at reducing CRC incidence and mortality. While most CRC screening programs use FITs, fewer than 50% of people participate. Common non-participation reasons include a lack of familiarity with the test and aversion to faecal sampling. Therefore, a user-friendly approach is needed to increase screening participation. We assessed the acceptability of a novel FIT that samples toilet bowl water containing faeces and provides point-of-care (POC) results using a rapid antigen lateral-flow test, then compared acceptability between consumers with and without prior CRC screening experience.
Methods: This pilot study provided South Australians (18-74 years) with the POC FIT, instructions, and a survey. A broad demographic was approached to ensure that consumers without prior CRC screening experience were also included. Consumers were asked to collect a sample of toilet bowl water after a bowel motion and apply this water to the rapid antigen test. Consumers interpreted their result according to instructions and completed a survey assessing their demographics, user experience, and preference of POC FIT versus other CRC screening tests. Survey responses between those with and without prior CRC screening experience were compared using Chi-squared tests. A p-value <0.05 was considered statistically significant.
Results: A total of 47 out of 52 (90.4%) invitees completed the POC FIT, with 53.2% (25/47) aged over 50 years and 59.6% (28/47) female. 80.9% (38/47) of participants had previously completed a CRC screening test. Most consumers (97.9%; 46/47) were confident they completed the test and read the results correctly, 97.8% (44/45) of consumers were satisfied to obtain an immediate result, and 97.8% (45/46) indicated they would feel comfortable reporting a positive result to their doctor. Useability responses were not significantly different between consumers with and without prior CRC screening experience (p>0.05, Table). Most participants who had previously completed a CRC screening test (64.9%, 24/37) preferred the POC FIT to other CRC screening tests commenting that it was easier, cleaner and quicker. Just two consumers (5.4%, 2/37) preferred other CRC screening tests with 29.7% (11/37) not having a preference between testing types.
Conclusion: The novel POC FIT was well-received and may provide a simple and familiar way of testing to enhance CRC screening participation. Larger studies assessing the user preference and diagnostic accuracy of the POC FIT are warranted.
Table. Comparison of user experience of POC FIT based on CRC screening experience
235
Clinical outcomes following incomplete surveillance colonoscopies in patients at increased risk of colorectal cancer
Syme Aftab1, Michelle Coats2, Kalindra Simpson2, Charles Cock2 and Erin Symonds2,3
1Department of Medicine, Flinders University, Adelaide, Australia;2Department of Gastroenterology and Hepatology, Flinders Medical Centre, Adelaide, Australia;3Flinders Health and Medical Research Institute, Flinders University, Adelaide, Australia
Background and Aim: Optical colonoscopy is the gold standard for colonic surveillance. Following incomplete colonoscopies (i.e., intubation fails to reach the caecum/terminal ileum), computerised tomography colonography (CTC) is recommended to complete colonic evaluation. However, the role of CTC following incomplete colonoscopies in the increased risk surveillance population is unknown. The aim of this study was to review the reason for incomplete colonoscopies in a surveillance population, and to assess the potential role of CTC in completing evaluation.
Methods: Incomplete surveillance colonoscopies in a public hospital setting (Jan 2017-Dec 2022) were audited. Procedures were excluded if the intended intubation site was distal to the caecum/terminal ileum. Data extracted from clinical reports included patient demographics, reasons for incomplete procedures, follow-up CTC results, and prevalence of advanced neoplasia at the next complete colonoscopy, by colonic site. Advanced neoplasia was defined as CRC or advanced pre-cancerous lesions (including adenomas ≥10mm, high-grade dysplasia; villosity, sessile serrated lesions ≥10mm or with dysplasia, traditional serrated adenomas, or ≥5 small tubular adenomas).
Results: Among 153 eligible incomplete colonoscopies (median patient age: 64.7 years, SD 12.3 years; 44.4% (n=68) male), the leading reasons for incompletion were anatomy-related: significant looping, tortuous colon, angulation, or restricted colonic mobility (58.2%, n=89), followed by inadequate bowel preparation (34.6%, n=53) and patient discomfort (20.9%, n=32). More than one reason was reported in 34% of cases (n=52). For follow-up, 20.9% (n=32/153) underwent a CTC, 53.6% (n=82) underwent a colonoscopy, and 25.5% (n=39) had no documented complete investigation to date. Among the CTC group (median 8.5 days (IQR 0.0-65.5) after the incomplete procedure), 30 CTCs detected no polyps. When 11 of these cases had subsequent colonoscopies (25.6 months (IQR 9.8-30.9) after the incomplete colonoscopy), advanced neoplasia was detected in 27.3% (n=3) of individuals, including CRC (n=1). Among patients who had a repeat colonoscopy as their first follow-up procedure (3.6 months (IQR 1.1-11.1) after the incomplete procedure), 88% (n=72) had complete intubation. Advanced adenoma was detected in 29.2% (n=21/72) of cases, with 81.0% (n=17) of these adenomas in a site not reached by the previous incomplete colonoscopy.
Conclusion: Abnormal anatomy, inadequate bowel preparation and patient discomfort were leading causes of incomplete surveillance colonoscopies. Follow-up colonoscopies revealed a significant rate of advanced neoplasia. With the focus in the increased risk surveillance population being detection and removal of advanced neoplasia, we conclude that CTC has a limited role following incomplete colonoscopy, and repeat colonoscopy should be the preferred approach.
258
A bruised TOE in the throat
Moshe Loebenstein, Bowen Xia and Sam Hui
Monash Health, Melbourne, Australia
Introduction: Oesophageal injury is a rare but important complication of transoesophageal echocardiography (TOE). We present a case of an extensive oesophageal haematoma presenting as odynophagia and dysphagia as a result of a TOE performed during a percutaneous mitral valve (MV) repair for severe mitral regurgitation.
Case report: An 80 year old male with a history of cardiomyopathy, pulmonary hypertension, AF and CKD underwent a MV repair with a Halfmoon prosthesis. 12000IU of heparin were administered intraoperatively as per protocol. A TOE probe was placed for the duration of the procedure. Towards the end of the procedure, blood was noted in the oropharynx and nares. His haemoglobin dropped from 119g/L to 85g/L with a concurrent drop in blood pressure requiring vasopressor support and a blood transfusion. The patient was extubated one day after the procedure and commenced on warfarin. He reported severe throat and retrosternal pain with minimal oral intake. On nasoendoscopy there was a small bruise over the right palate with an otherwise normal exam. A contrast CT was recommended however the patient’s renal function (eGFR 25ml/min) precluded this. The patient commenced total parenteral nutrition (TPN) and an urgent gastroenterology opinion was requested. Endoscopic assessment was delayed due to supratherapeutic warfarinisation (INR 9.4) which was treated with intravenous Vitamin K. A gastroscopy was performed 6 days post the initial procedure which demonstrated an extensive linear submucosal haematoma (Figure 1a). The gastroscope was not progressed beyond the distal end of the haematoma due to risk of perforation. The patient was managed conservatively with cautious upgrading of his diet. 12 days after the initial injury parenteral nutrition was ceased. He was anticoagulated first with subcutaneous enoxaparin and then with warfarin. A CT chest with oral contrast performed 2 weeks after the procedure demonstrated residual oesophageal wall thickening but no perforation (Figure 1b).
292
Evaluation of demographics and outcomes of patients undergoing endoscopy after-hours
Zainab Abdul-Rahman, Rohita Reji and Abhey Singh
Fiona Stanley Hospital, Perth, Australia
Background and Aim: After-hours emergency endoscopic procedures are indicated in various settings and utilize significant healthcare resources. Current guidelines recommend performing an endoscopy within 24-hours of upper gastrointestinal bleeding (UGIB) presentation (1). Studies have shown no difference in clinical outcomes in UGIB patients undergoing endoscopy in <6 hours compared to 6-24 hours after hospital presentation (1, 2). We aimed to assess demographics and outcomes of patients undergoing endoscopy after-hours.
Methods: We conducted a single-center retrospective cohort study of adult patients who underwent endoscopy afterhours (1700-0800) from Jan 2023-Jan 2024 at a major tertiary hospital in Western Australia. Information was collected from electronic medical records and analyzed using Graphpad Prism 10.2.3. Patients were categorized based on the timing of endoscopy: urgent (<6 hours) or early (6-24 hours) from presentation. Primary outcome assessed was 30-day all-cause mortality. Secondary outcomes included 30-day rebleeding rate, 30-day ICU admission and length of hospital stay (LOS).
Results: The study included 126 patients, with a mean age of 63 years. 63% (79/126) of cases had afterhours endoscopy for UGIB and 37% (47/126) for non-UGIB. 79% (100/126) of patients required a therapeutic endoscopic intervention. Among UGIB patients, 30% (24/79) were variceal and 70% (55/79) were non-variceal. 56% (44/79) of UGIB patients had endoscopy within 6 hours and 44% (35/79) within 6-24 hours. 30-day all-cause mortality was 9.5% (12/126) among the whole cohort and 11.4% (9/79) among patients with UGIB (9.1% in non-variceal bleeding group vs 17% in variceal UGIB). The mean age of death was 67.6 years. In the non-variceal UGIB group, 4/5 deaths were from complications of ongoing bleeding and 1 was due to underlying cancer. In the variceal UGIB group, all 4 deaths were from complications of chronic liver disease. There was no significant difference in the 30-day all-cause mortality between the urgent (13.6%, 6/44) and early (8.6%, 3/35) groups (p = >0.99, NS). Secondary outcomes of 30-day rebleeding rate and 30-day ICU admission were not significantly different between the two groups. However, the LOS was lower at 8 days in the urgent group vs 17 days in the early group (p = 0.039).
Conclusion: Our study revealed a significant 30-day all-cause mortality of 9.5% among patients undergoing afterhours endoscopy, with most deaths occurring in patients with UGIB. There was no significant difference in 30-day all-cause mortality, 30-day rebleeding rate or ICU admissions of UGIB patients undergoing urgent (<6 hours) versus early endoscopy (6-24 hours). However, urgent endoscopy resulted in a significantly reduced LOS compared to early endoscopy. These findings align with previous observational studies and emphasize the importance of medical optimization before endoscopy. The high mortality rate among UGIB patients highlight the need for enhanced care of these patients such as by utilizing specialized UGIB units with strict protocols.
References
1.
Lau, J., Yu, Y., Tang, R., et al. Timing of Endoscopy for Acute Upper Gastrointestinal Bleeding. N Engl J Med2020; 382: 1299-1308.
2.
Merola, E., Michielan, A. & Pretis, G.Optimal timing of endoscopy for acute upper gastrointestinal bleeding: a systematic review and meta-analysis. Intern Emerg Med16, 1331–1340 (2021). https://doi.org/10.1007/s11739-020-02563-1
297
A rare case of metastatic renal cell carcinoma to the stomach presenting as upper gastrointestinal bleeding
Gurtej Singh1, Nicholas Mingos1, Maeve Slevin2 and Ashok Raj1
1Department of Gastroenterology, The Royal Melbourne Hospital, Melbourne, Australia;2Department of Anatomical Pathology, The Royal Melbourne Hospital, Parkville, Australia
Background: Renal cell carcinoma (RCC) accounts for 2.8% of cancer diagnoses in Australia. 25-30% of patients present with distant metastases at diagnosis with the commonest sites including the lungs, lymph nodes, bone and liver, and portending a poorer prognosis. Gastric metastases are exceedingly rare with few cases reported and an incidence of <1%. We report a unique case of a patient with metastatic RCC to the stomach presenting with upper gastrointestinal bleeding.
Case report: A 73-year-old lady with a history of multiple sclerosis, previous bowel resection for diverticulitis presented with haematemesis and melaena. She reported a one year history of progressive fatigue, 20kg unintentional weight loss, and a one month history of dull right-sided abdominal pain. Laboratory studies revealed anaemia, leukocytosis and hypercalcaemia. Oesophagogastroduodenoscopy (OGD) revealed three 10-20mm sessile fundic gland polyps with stigmata of recent bleeding. All three polyps were injected with adrenaline, hot snared whilst haemostasis was achieved with soft coagulation and endo-clips. A contrast-enhanced computed tomography (CT) scan revealed a large 7cm heterogeneous mass in the right kidney with extrarenal extension into the perinephric space and extensive metastases to the liver and lungs. Histology of the gastric polyps showed high grade malignant spindle cells with smooth muscle differentiation consistent with sarcomatoid renal cell carcinoma. Further tissue biopsy was deemed unnecessary given the histology seen from polypectomy. The patient’s gastrointestinal bleeding resolved following OGD and polypectomy. Unfortunately, they had a liver metastases rupture three weeks after presentation and a palliative approach was taken.
301
Influence of endoscopic biopsy forceps characteristics on tissue specimens
Lulu Zhang1, Mark Bettington2, Mike Jones3 and Nicholas Tutticci1
Background and Aim: Tissue acquisition with biopsy forceps is routine during diagnostic endoscopic procedures. Currently a large variety of forceps are available characterised by differences in jaw size and shape, cup contour (“toothed/alligator cup” vs smooth) or a needle. Pathologic interpretation of biopsy specimens may be impacted by submucosal inclusion, orientation, and crush artifact. Historical studies consistently show jaw size is associated with larger samples. Studies comparing currently available forceps however are lacking, and there is heterogeneity in the preference for biopsy forceps among Endoscopists, as well as in their availability in Endoscopy units. Hence the aim our study was to assess the difference in tissue specimen quality between commonly used biopsy forceps.
Methods: A retrospective pathologist-blinded cohort study was performed. Three biopsy forceps without needle (jaw toothed 2.4mm, smooth cup “toothless” 2.3mm, and jaw toothed 2.2mm) were trialled in an Endoscopy unit to gauge Endoscopist acceptability and inform procurement decisions. From this period, a blinded expert gastrointestinal Pathologist re-reviewed each tissue specimen obtained with these biopsy forceps during routine diagnostic endoscopy and/or colonoscopy. Specimens were assessed for size, orientation, crush artefact and the presence of submucosa. Statistical analysis comprised nonparametric Kruskal-Wallis test for null hypothesis of equality between forceps and three unique pairwise contrasts with Mann-Whitney test.
Results: During the study period, 538 tissue specimens were collected (table 1). The largest forceps returned significantly larger mean specimen size compared to the smaller forceps (p<0.001). Most biopsy specimens did not contain submucosa (87%) however submucosa was more frequently identified in with the larger forceps (p=0.003). Smooth cup 2.3mm forceps had a higher proportion of poorly oriented specimens, while again, larger 2.4mm forceps had the least with poor orientation (p=0.04). All forceps, regardless of jaw contour, exhibited no crushing of tissue (100% intact). Further specific paired comparison between the smooth cup 2.3mm and toothed 2.2mm demonstrated no significant differences. No clinically significant adverse events were recorded in study patients and haemostatic techniques were not required for any biopsy sites.
309
Rare case of doxycycline-induced gastric mucosal injury
Christopher James Shephard and Rozemary Karamatic
Department of Gastroenterology and Hepatology, Townsville University Hospital, Townsville, Australia
Introduction: Doxycycline, a commonly prescribed tetracycline antibiotic, is a well-known cause of drug-induced oesophagitis and ulceration. In contrast, doxycycline-induced gastric mucosal injury (DGMI) is rarely encountered, with small bowel injury even less frequent. Patients may be asymptomatic or exhibit dysphagia, epigastric pain or anaemia due to gastrointestinal (GI) bleeding following a variable lead time (five days to three years). Gastric lesions are characterised by inflamed mucosa with overlying white-yellow plaque and/or ulceration. Histologically, drug-specific injury is depicted by eosinophilic degeneration of superficial capillaries and microthrombi formation with overlying mucosal necrosis. Additionally, reactive foveolar epithelial change, prominent lamina propria neutrophilic infiltrate and erosion/ulceration may be present. We report a case of DGMI to improve awareness regarding this infrequent adverse outcome of doxycycline use.
Case report: A 78-year-old gentleman with diabetes, hypertension, ischaemic heart disease with coronary stenting, chronic kidney disease and chronic back pain was admitted with dyspnoea in the setting of pulmonary oedema due to non-ST segment elevation myocardial infarction and acute normocytic anaemia (haemoglobin 77g/L versus 122g/L from 13 days prior) with melaena concerning for upper GI bleeding. Eleven days earlier he commenced a 2-week course of doxycycline 100mg twice daily following evaluation for pyrexia of unknown origin. Relevant co-medications included aspirin and clopidogrel but no recent anti-inflammatory drug use. Platelet count and international normalised ratio were within normal limits. He was initially managed with temporary antiplatelet interruption, two units of packed red blood cells and high-dose intravenous pantoprazole. Oesophagogastroduodenoscopy revealed widespread gastritis involving the cardia, fundus, and gastric body with isolated white plaque-like lesions (figure 1) but no ulceration, and three small non-bleeding ulcers in the second portion of the duodenum. Gastric biopsy exhibited surface erosion with neutrophilic infiltration and reactive epithelial changes. Multiple superficial mucosal capillaries demonstrated degenerative change with eosinophilic necrosis and microthrombi formation, highly consistent with DGMI (figure 2). There was no evidence of Helicobacter pylori, viral cytopathic changes or dysplasia/neoplasia. Doxycycline was ceased and antiplatelet therapy was resumed under high-dose oral pantoprazole cover without re-bleeding. Without supportive biopsy, it remains unclear whether doxycycline also instigated duodenal ulceration in this case.
314
A serious case of post-colonoscopy colitis
Irene Lu, Eliza Flanagan, Carl Cosgrave, Jack Shembrey and Damian Dowling
Barwon Health, University Hospital Geelong, Geelong, Australia
Introduction: Immediate complications post-colonoscopy includes bleeding and perforation. Colitis as a complication of colonoscopy is incredibly rare. It has only been described in a few case reports (1,2) and often in patients with underlying medical conditions such as connective tissue disorders or vascular risk factors for ischaemia (3,4). There has been reports of chemical colitis from historical use of glutaraldehyde to clean colonoscopy equipment (5) and unexpected reports of ischaemic colitis with aggressive bowel preparation in constipated patients over the age of 75 (6). We report an unusual case of severe colitis post-colonoscopy without clear aetiology.
Case report: A 70-year-old female with obesity and type-2 diabetes underwent routine endoscopy for investigation of iron deficiency anaemia and altered bowel habits. Colonoscopy revealed uncomplicated left-sided diverticular disease and a 5mm splenic flexure polyp removed via cold snare. Random colonic biopsies were taken. The day following colonoscopy she developed abdominal pain, profuse diarrhoea and vomiting. On day two post-colonoscopy, she presented to hospital due to worsening pain despite spontaneous resolution of her diarrhoea. On physical examination, she was found to have diffuse abdominal tenderness with profound hypotension. Her admission CRP was 416 mg/L with normal white-cell count. She was managed with vasopressor support, intravenous fluids and antibiotics, and subsequently continuous renal replacement therapy (CRRT) for anuric renal failure. Computer tomography (CT) revealed diffuse bowel wall thickening of the hepatic flexure, proximal and mid-transverse colon with adjacent fat stranding, without evidence of pneumoperitoneum or intra-abdominal collection. The patient did not open her bowels again until 4 days following presentation, whereby stool testing was negative for infection. Her renal function recovered but her admission was complicated by persistent abdominal pain and nausea limiting oral intake and necessitating total parenteral nutrition. Serial imaging revealed persistent and progressive inflammation of the hepatic flexure without radiological evidence of perforation or pneumoperitoneum. Exploratory laparotomy on day 19 revealed gross inflammation of the distal ascending and proximal transverse colon with multiple mesocolon abscesses and a contained abscess at the hepatic flexure. The patient underwent a right hemicolectomy with stoma formation. Histopathology of the bowel showed non-specific acute on chronic inflammation contained within the submucosal layer. The patient recovered on the ward and was discharged home 20 days post her operation.
Conclusion: The aetiology of colitis in this post-colonoscopy case remains undifferentiated and has resulted in significant morbidity and prolonged hospitalisation. Whilst infective colitis resulting in bacterial septic shock remains a leading differential given the significantly raised inflammatory markers, the lack of positive faecal stool sampling and positive blood or urine culture remains contradictory. As a well-accepted complication, perforation remains possible, but this would typically present with localised radiological findings and would not proceed in this clinical course with organ dysfunction and subsequent histological findings of diffuse inflammation. Some case reports have demonstrated surprising diagnoses of ischaemic colitis after histopathological review, but our patient has a negative arterial phase CT and histological results are non-specific. Endoscopist should be aware of serious colitis as a potential, albeit rare, complication of diagnostic colonoscopy.
References
1.
Shah, Parin; Aggarwal, Aakash; Vaziri, Haleh. A Rare Case of Post Colonoscopy Colitis: 1351. American Journal of Gastroenterology111:p S607, October 2016.
2.
Mathew, Madhu; Elkhouly, Mohamed A.; Mbachi, Chimezie U.
et al. An Unusual Case of Post Colonoscopy Colitis - A Pathological Surprise: 1485. American Journal of Gastroenterology113:p S852-S853, October 2018.
3.
Wheeldon, NM, Grundman, MJ. Ischaemic colitis as a complication of colonoscopy. BMJ1990; 301(6760): 1080–1081.
4.
Versaci, A, Macrì, A, Scuderi, G, Bartolone, S, Familiari, L, Lupattelli, T, et al. Ischemic colitis following colonoscopy in a systemic lupus erythematosus patient: report of a case. Dis Colon Rectum2005; 48 (4): 866–9.
5.
Ahishali, E. Uygur-Bayramiçli, O. Dolapçioğlu, C. Dabak, R. Mengi, A. Işik, A.et al. Chemical colitis due to glutaraldehyde: case series and review of the literatureDig Dis Sci Dec 23 2008 e-pub ahead of print).
6.
Kawamura, T, Sakiyama, N, Tanaka, K, Yokota, I, Uno, K, Yasuda, K. Ischemic Colitis Caused by Bowel Preparation for Colonoscopy. Gastroenterology Res. 2021 Oct; 14(5): 296-303. doi: https://doi.org/10.14740/gr1461. Epub 2021 Oct 14. PMID: 34804274; PMCID: PMC8577598
324
Endoscopic retrieval of a partially deflated intragastric balloon: a case report
Denis Rubtsov1 and Nicholas Tutticci2
1The Prince Charles Hospital, Brisbane, Australia;2Royal Brisbane and Women's Hospital, Brisbane, Australia
Introduction: Fluid-filled intragastric balloon (IGB) is a widely utilised non-surgical weight loss modality. Advantages of reversibility and lower cost than bariatric surgery are offset by potential adverse events including balloon rupture, migration and bowel obstruction. There is no consensus on the optimal endoscopic technique for removal of a malfunctioning balloon. We report a case of a successful endoscopic removal of a ruptured and partially deflated IGB with long dwell time.
Case report: A 51-year-old woman presented with a mild epigastric pain and blue-coloured urine. She underwent a placement of an Orbera® IGB (Apollo Endosurgery, Austin, Tex, USA) 18 months prior and elective removal of the balloon at 6 months was delayed in the context of a therapeutic relationship breakdown with the treating practitioner. She was haemodynamically stable on admission, reported no nausea, vomiting or other symptoms of bowel obstruction. However, a CT scan demonstrated a collapsed gastric balloon at the fundus extending through the pylorus into the duodenal bulb (Figure 1). Considering the impending risk of small bowel obstruction, the decision was made to retrieve the IGB emergently in an after-hours setting. Endoscopy was performed under general anaesthesia with endotracheal tube placement. The near completely deflated leaking IGB was found in the stomach. The manufacturer’s recommended draining equipment and balloon retractors were not readily available. Presumably due to the long dwell time of the balloon the material was stiff and inelastic. Attempted removal with a large polypectomy snare failed to grasp the convex balloon end. Attempted removal with a Rescue® Rat Tooth Grasping Forceps (Boston Scientific, Marlborough, MA, USA) failed due to residual fluid in the dependent component limiting passage beyond the lower oesophageal sphincter. The perishing balloon tore under tension. The forceps was then used to intentionally create a 15mm defect in the balloon which permitted complete drainage of IGB fluid with the gastroscope partially inserted into the balloon remnant. Secondly the defect permitted a polypectomy snare purchase of the end of the balloon where it previously slipped repeatedly due to the convex configuration. Atraumatic retrieval through the mouth was then uneventful.
Conclusion: This case demonstrates endoscopic technique of a partially deflated IGB removal, utilising the equipment that is readily accessible to all endoscopists. This approach can be considered for balloons after a long dwell time where other techniques fail as it appears to be effective and safe.
338
Gastrointestinal stromal tumor presenting with life threatening haematemesis - a rare cause of upper gastrointestinal bleeding highlighting the importance of a multidisciplinary approach
Robert O'Neill1,2, Phillip Leaver1,2, Connor Ryan1,2 and Ian Lockart1,2
1St Vincent's Hospital Sydney, Sydney, Australia;2The University of New South Wales, Sydney, Australia
Introduction: Gastrointestinal stromal tumours (GIST) are the most common type of mesenchymal tumor of the gastrointestinal tract. Clinical presentation is variable and is dependent on the tumor's location and size. Approximately 25% of GISTs manifest with recurrent gastrointestinal bleeding, however acute haematemesis with haemodynamic instability and shock is relatively uncommon. We present the case of a patient who presented to our institution with an acute episode of haematemesis secondary to an ulcerated gastric GIST.
Case report: A 61-year-old male was brought in by ambulance to our institution with five episodes of haematesis and pre-syncopal symptoms. He had a medical history notable for a previous lumbar spine laminectomy. He was on no regular medications. On initial examination he was hypotensive to 80/50 mmHg and tachycardic with a heart rate of 122 bpm. Frank haematemesis on initial assessment. The remainder of his examination was normal. Initial biochemical assessment revealed a haemoglobin of 115 g/L and urea of 11.4 mmol/L with preserved renal function. Serum lactate was 2.2 mmol/L. Intravenous fluid resuscitation was commenced along with a pantoprazole infusion. The patient underwent emergent upper gastrointestinal endoscopy which revealed a large gastric mass (5 cm in size) which was 4 cm distal to the gastroesophageal junction over the posterior wall and fundus of the stomach (Figure 1a). Macroscopically the mass appeared to be submucosal in origin with preservation of the overlying mucosal architecture. A large ulcer measuring 1 cm in diameter was present on the posterior surface of the mass with a visible vessel present at the base (Forest class 2a). Bleeding was provoked on minimal trauma (Figure 1b). Haemospray was applied for haemostasis. Computed tomography abdomen was performed which demonstrated a well-circumscribed hypoattenuating lesion within the fundus of the posterior wall of the stomach measuring 30 x49 mm. Surgical opinion was sought and the patient underwent partial gastrectomy. Histopathological analysis of the resected specimen revealed a 40 mm gastric fundus GIST with clear surgical margins (AJCC pT2). The patient had an uncomplicated postoperative period and was discharged home.
Conclusion: GISTs are a relatively uncommon benign gastrointestinal neoplasm that can present with variable symptoms ranging from indolent to hyperacute. This case highlights an uncommon presentation of a GIST with an acute upper gastrointestinal haemorrhage and highlights the importance of multidisciplinary management and definitive surgical management given the limited scope of endoscopy.
344
Eosinophilic gastroenteritis with mucosal and serosal involvement: A rare cause of abdominal pain and ascites
Georgia Zeng1,2, Robert O'Neill1, Phillip Leaver1,2, Connor Ryan1,2, Fiona Tudehope1,2 and Santosh Sanagapalli1,2
1Department of Gastroenterology and Hepatology, St Vincent's Hospital, Sydney, Australia;2St Vincent’s Clinical School, Faculty of Medicine, University of New South Wales, Sydney, Australia
Introduction: Eosinophilic gastroenteritis is a rare immune-mediated condition defined by the presence of gastrointestinal symptoms alongside the histological demonstration of eosinophilic infiltration in the gastrointestinal tract or eosinophilic ascitic fluid. In this case report, we describe a patient who presented with gastrointestinal symptoms and marked peripheral eosinophilia, who was found to have eosinophilic gastroenteritis with both mucosal and serosal disease involvement.
Case report: A 35-year-old man presented to our institution with a 6-week history of abdominal pain with associated nausea, vomiting and anorexia. He described a history of intermittent episodes of abdominal pain for the past few years prior to presentation. Other past medical history was remarkable for hypertension. Clinical examination was notable for epigastric tenderness. His complete blood count was remarkable for an eosinophil count of 2.6. Computed tomography scan of his abdomen demonstrated features of partial gastric outlet obstruction, a cluster of small nodules about a distal small bowel loop in the upper pelvis and a moderate volume of ascites. Endoscopy demonstrated thickening and erythema of the pylorus with an element of gastric outlet obstruction (Figure 1A); the second part of the duodenum was boggy and thickened (Figure 1B), not allowing deeper passage of the paediatric colonoscope. Alternative causes of eosinophilia were excluded on serological assessment. Biopsies of the duodenal mucosa demonstrated an inflammatory infiltrate of predominantly eosinophils, without dysplasia or malignancy. Ascitic fluid, obtained via ultrasound-guided paracentesis, demonstrated a total white cell count of 1900 x 106 cells, of which 91% were eosinophils. Bone marrow aspirate demonstrated a mildly hypercellular aspirate with active trilineage haematopoiesis, with proliferation of left shifted eosinophils averaging 23% of total nucleated cells. There was no evidence of clonality or cytogenic abnormalities detected on this sample. The patient’s eosinophils rose to a peak of 5.2 six days into his admission. He was exquisitely sensitive to intravenous corticosteroids, with a drop of eosinophil count to 0.3 the following day. He was promptly stepped down to oral corticosteroids and discharged on a weaning regimen.
Conclusion: This was a case of eosinophilic gastroenteritis with serosal and mucosal involvement that responded well to initial corticosteroid therapy. Idiopathic hypereosinophilic syndrome was considered as a differential diagnosis but ultimately ruled out given the absence of multi-system involvement. Long-term treatment options include dietary therapy, immunomodulators and biologics, and disease trajectory remains difficult to predict given the sparsity of cases.
349
A retrospect audit of inpatient upper endoscopy for dyspepsia evaluation: Single centre experience
Thant Zaw1,2 and Montri Gururatsakul1,2
1Cairns Hospital, Cairns, Australia;2James Cook University, Cairns, Australia
Background and Aim: Dyspepsia is a collection of non-specific upper epigastric discomfort symptoms that often prompt further evaluation through upper endoscopy. However, the role of dyspepsia as an inpatient workup is both practical and can lead to increased hospital stays and inpatient costs. This study was conducted at a regional hospital to assess the outcomes of inpatient endoscopy for patients presenting with dyspepsia.
Methods: We retrospectively analysed data from inpatients who underwent inpatient endoscopy for dyspepsia at the regional hospital from January 2014 to March 2024. Patient presentation history, endoscopy reports, and biopsy data were gathered from electronic medical records and the endoscopy documentation software (Provation). The primary objective was to determine the cause of dyspepsia, while the secondary goal was to assess the feasibility of conducting these evaluations in outpatient settings.
Results: A total of 57 upper endoscopy procedures were performed over a 10-year and 2-month period. The patients' ages ranged from 15 to 85, with 54% of the subjects (n=31) being above 50 years old. Alarming features were identified during the analysis, with the most common being persistent vomiting in 20 patients and unintentional weight loss in 15 patients. The predominant findings included gastritis (54.4%), normal findings(15.9%), oesophagitis (8.7%), duodenal ulcer (7%), and gastric ulcer(7%). H. pylori was detected in 3 cases, but no cases revealed any urgent issues requiring immediate attention or malignancy.
Conclusion: The results indicated that alarming features have a low predictive value for gastrointestinal malignancy. The findings of the audit suggest that endoscopy assessments for new-onset dyspepsia in elderly patients or those with alarming features can be safely conducted in outpatient settings. This approach has the potential to reduce hospital stays and overall hospitalization costs.
358
Patient sedation satisfaction for endoscopy procedures comparing anaesthetist assisted endoscopy sedation and endoscopist-directed nurse administered propofol sedation (EDNAPS)
Keith Brick and Montri Gururatsakul and Shihaz Hussain and Raymond Lewandowski and Peter Boyd
Queensland Health, Cairns, Australia
Background and Aim: Endoscopist-directed nurse administered propofol sedation (EDNAPS) has been demonstrated to be safe and effective in patients undergoing gastroscopy and colonoscopy procedures. Our regional endoscopy unit utilizes either EDNAPS or anaesthetist assisted endoscopy sedation for such procedures. We aim to investigate patient satisfaction of their sedation at our unit between the anaesthetist assisted endoscopy sedation and EDNAPS.
Methods: In a single centre study, patients at a regional hospital who underwent simple endoscopic procedures (gastroscopy, colonoscopy, endoscopic dilatation) received sedation from either an anaesthetic team or EDNAPS. Over a three week period (with a plan to extend to 6 months) patients undergoing these procedures were phoned 1-2 weeks after their procedure. They were asked 3 questions related to their satisfaction of the sedation they received. The first two questions were graded on a 5 point Likert Scale: 1. Does the patient remember experiencing pain or discomfort during the procedure; 2. The patients overall satisfaction of sedation. The third question (yes or no) asked if the patient would be willing to have similar sedation for the same procedure in the future. Data collectors were blinded to which type of sedation patients received when contacting the patient. Patient co-morbidities, ASA classification, procedural complications, medication doses, procedural timings and discharge timings were all recorded on a data sheet.
Results: A total of 98 patients underwent simple endoscopic procedures, and 70 of these patients were able to be contacted by phone regarding their endoscopic procedure (71% phone call response rate). There were 54 patients who received EDNAPS – of this group 9 were ASA 1, 35 were ASA 2 and 10 were ASA 3. In the anaesthetist assisted endoscopy sedation, there were 16 patients – 3 were ASA 2, 8 were ASA 3 and 5 were ASA 4. There were a total of 23 gastroscopies, 34 colonoscopies, 12 combined gastroscopy and colonoscopies, and 1 endoscopic dilatations. Of those who responded who underwent EDNAPS, 53/54 patients (98%) would be willing to have similar sedation for a repeat procedure and 52/54 patients (96%) had no pain with their procedure. In the anaesthetic group 16/16 patients (100%) experienced no pain and would have similar sedation for a repeat procedure. There were no complications reported in any of the procedures in both groups.
Conclusion: In this audit, the preliminary results showed that patients undergoing simple endoscopic procedures are equally satisfied with EDNAPS compared to anaesthetist assisted endoscopy sedation and there was no difference in complications between the groups. This supports that EDNAPS is both safe and effective for patients given a very high satisfaction rate.
363
Bleeding mid-jejunal lesion accessible only with motorised spiral enteroscopy
Shane Selvanderan, Robert Little, Catriona McLean, Mark Ward and Gregor Brown
The Alfred Hospital, Melbourne, Australia
Introduction: Small bowel lymphangiomas are benign tumours characterised by dilated lymphatic spaces and account for <1% of all lymphangiomas. They are more common in children and may be complicated by gastrointestinal bleeding, torsion or intussusception.
Case report: A 26-year-old man of Thai ethnicity presented in 2013 with symptomatic iron deficiency anaemia (IDA) - haemoglobin 51 g/L, ferritin 3 mcg/L and transferrin saturation 7%. Coeliac serology, haemolytic screens, stool microbial testing, esophagogastroduodenoscopy and ileocolonoscopy were unremarkable. Inconsistent clinic engagement precluded timely investigation over the subsequent nine years despite recurrent profound IDA requiring a total of 11 units of packed red blood cells and four iron infusions. Capsule endoscopy identified a mid-jejunal, erythematous, polypoid, plaque-like circumferential lesion. Given epidemiological exposure risk and positive schistosomiasis serology, the patient was treated with two courses of praziquantel and despite this the patient had recurrent iron deficiency anaemia requiring ongoing transfusions. Abdominal CT revealed intra-abdominal lymphadenopathy and differential diagnoses of tuberculosis and small bowel lymphoma were considered. Bidirectional double-balloon enteroscopy was unable to reach the lesion. Surgical referral was offered but the patient opted for a conservative approach with supportive transfusions. A follow-up surveillance capsule endoscopy identified progression of the mid small bowel lesion with fresh bleeding. Expertise and equipment for motorised spiral enteroscopy became available and the haemorrhagic lesion was reached for tissue biopsies via an antegrade approach (Figure 1). Three days post-procedure the patient experienced melaena, increasing abdominal pain, and eventually a complete small bowel obstruction, attributed to biopsy-related haemorrhage. He underwent an exploratory laparotomy with resection of a 65 x 60 mm firm, obstructing mass. Histopathology demonstrated acute haemorrhage and inflammation with deep ectatic vascular channels containing proteinaceous lymphatic material extending from the mucosa to muscularis propria, consistent with a small bowel lymphangioma.
Conclusion: Mid-jejunal bleeding lesions can pose a diagnostic and therapeutic challenge. Video capsule endoscopy allows for lesion visualisation but not biopsy. Balloon enteroscopy with a view to endoscopic interventions such as biopsy and haemostasis may not achieve the depth of small intubation required for access. Motorised spiral enteroscopy, used in this case, is a technique with impressive rates of pan-enteroscopy but was associated with a risk of unpredictable serious adverse events due to device impaction, and was recalled from the market. There remains a role for small bowel resection, particularly in an isolated small bowel bleeding mass lesion inaccessible via endoscopy.
364
Endoscopy-related musculoskeletal pain and injury in endoscopists and endoscopy nurses
Oyekoya Ayonrinde1,2,3, Alan Doyle1, Lena Thin1,2 and Robert Waller3
1Fiona Stanley Hospital, Perth, Australia;2The University of Western Australia, Perth, Australia;3Curtin University, Perth, Australia
Background and Aim: Musculoskeletal (MSK) pain and injury is increasingly recognised in endoscopists, potentially resulting in time off work or various therapeutic interventions. Consequently, ergonomic training and strategies to reduce injury are encouraged. There is less known about musculoskeletal pain and injury in endoscopy nurses. We examined patterns of MSK pain in endoscopists and endoscopy nurses at a tertiary hospital.
Methods: In this single centre survey, a questionnaire survey regarding MSK pain at different body sites, was administered to endoscopists and endoscopy nurses. Specific questions related to location, frequency, duration and severity of pain episodes, professional role, gender, and age. We also enquired about glove size, number and type of endoscopic procedures performed per week, personal weight and height, distribution of patient gender and body mass index, and sites of MSK pain. Respondents documented the occurrence of pain relative to endoscopy procedures, a diagnosis of MSK pain or injury syndromes, which professionals had been consulted about the pain, whether they had been taught about ergonomics in endoscopy or would like to be taught, and personal exercise routines.
Results: Respondents included 31 endoscopists and 14 nurses, and both considered at least 50% of patients attending an endoscopic procedure to be obese. Endoscopist respondents were 68% gastroenterologists, 22% surgeons and 10% gastroenterology registrars, and 77% male. Overall, 70% were aged ≥40 years, 60% had ≥9 years endoscopy experience, and 52% had medium-sized hands and 23% had small hands. Pain lasting ≥ 6 months was reported by 50%, and 17% reported a pain severity of at least 5/10 in the preceding week. The most common site of pain was the left thumb/thumb base. Other common pain sites were the neck, right-sided low back pain, right shoulder, wrist, and elbow (Figure 1). Pain was experienced only when performing endoscopic procedures in 16%, and during and outside endoscopy in 65%. Pain relief remedies were sought from physiotherapists (23%), massage therapist (21%) chiropractor (8%), rheumatologists (5%) or orthopaedic surgeon (5%). A minority (16%) reported having had endoscopy-related ergonomics training, and 81% stated they want more ergonomics information to reduce endoscopy-related injury (Figure 2). Among 14 endoscopy nurse respondents (all female, 50% aged ≥40 years), 50% reported pain lasting over 1 year. 70% had small hands, and reported pain mostly in their back, neck, shoulder or feet, numbness in their hands or feet, or carpal tunnel syndrome (Figure 1). Pain relief remedies were sought mainly from a physiotherapist (24%) or chiropractor (21%), or massage therapist (14%), and 86% knew an endoscopy nurse who had experienced pain severe enough to require time off work, or a therapeutic intervention. Further, 57% worried often or very often that they might experience work-related musculoskeletal injury, and 36% have accordingly considered changing jobs. In contrast to doctors, 36% of nurses say they were taught about ergonomics, and 86% of them want more ergonomics information to reduce endoscopy-related injury (Figure 2).
Conclusion: Patterns of musculoskeletal pain are different, comparing endoscopists and endoscopy nurses. Despite musculoskeletal pain being common in endoscopists and endoscopy nurses, and impacting their well-being, the majority have not had ergonomic training but would like more information on how to avoid injury. Ergonomic training and injury prevention strategies are critical to maintaining the endoscopy workforce.
383
Iron deficiency without anaemia; any clinically significant outcomes on combined gastroscopy and colonoscopy?
Aidan Taylor and Montri Gururatsakul
Cairns and Hinterland Hospital and Health Service, Cairns, Australia
Background and Aim: Iron deficiency anaemia remains a strong indication for combined gastroscopy and colonoscopy to exclude chronic gastrointestinal blood loss, especially malignancy. However, the utility of combined gastroscopy and colonoscopy remains unclear in patients with iron deficiency without anaemia and the aim of the study is to assess for any clinically significant outcomes in these patients.
Methods: This is a retrospective study, data from patients referred to Endoscopy Unit with iron deficiency without anaemia (Serum ferritin < 20g/L, normal haemoglobin) between 2018 to 2023 were analysed. Patients were assessed for endoscopic evidence of cause for iron deficiency without anaemia compared with age, sex, and presence of alarm symptoms at time of referral.
Results: 132 patients (65% female, mean age 54.17): 42.4% were aged <50 years, 36.4% were 50 – 69 years, and 21.2% were >70 years old, received endoscopic evaluation for iron deficiency without anaemia. Of those 132 patients, 91% received both gastroscopy and colonoscopy, 4.5% received upper endoscopy alone and 4.5% colonoscopy only. The significant outcomes of interest were divided into minor findings (H pylori gastritis, angioectasia, autoimmune atrophic gastritis and ulcers) and major findings (malignancy, polyps >20mm and adenomas with high grade dysplasias). Of those 132 patients, total of 24 patients referred with iron deficiency without anaemia were found to have abnormal endoscopic findings; 3.8% (n = 5) had major findings and 16% (n=21) had minor findings. 36% (n=48) of patients had alarm symptoms (Dysphagia, odynophagia, weight loss, haematemesis, rectal bleeding) or faecal occult blood test positive at time of referral. Of those referred with alarm symptoms 17% (n = 8) had minor endoscopic findings and 8.3% (n = 4) had major findings. Compared to those who did not have alarm symptoms, 15% (n = 13) had minor findings and 1.2% (n = 1) had major findings. H pylori gastritis was the most common minor finding with 11 cases (55% of cases occurring in patients <50 years of age [n = 6]). There were 7 patients with non-bleeding angioectasia, (57% [n = 4] occurring in patients >70 years of age). 1 patient had autoimmune atrophic gastritis. No patient was found to have gastric or duodenal ulcers. There were 5 major findings, 3 patients had polyps >20mm (tubular adenoma with low grade dysplasia), 1 patient had adenocarcinoma and 1 patient tubular adenoma with high grade dysplasia. Of the major findings 1 was <50 years old and 4 were >50 years of age.
Conclusion: Overall, the data shows that H pylori gastritis is a common cause for iron deficiency without anaemia in those <50 and reinforces the need to look for malignancy in those aged >50. Patients referred with iron deficiency without anaemia who had alarm symptoms were almost 7 times more likely to have major findings compared to those who did not.
385
A rare case of nivolumab induced oesophagitis 4 years after commencement of therapy
Aidan Taylor and Montri Gururatsakul
Cairns and Hinterland Hospital and Health Service, Cairns, Australia
Introduction: Nivolumab, an immune check-point inhibitor, is a class of immunotherapy currently approved in Australia for the treatment of various locally advanced and metastatic cancers. Although Nivolumab is an effective treatment option for cancer, this class of medication is associated with immune-related adverse events, including immune mediated colitis, and immune mediated hepatitis are well documented in the literature. However, reports of upper-gastro-intestinal adverse events such as oesophagitis remains rare. This is a case report of a patient who developed Nivolumab induced oesophagitis.
Case report: A 60-year-old female presented with dysphagia and odynophagia for 4 weeks, her past medical history included metastatic melanoma treated with Nivolumab in the last 4 years. Subsequently, upper endoscopy showed oesophagitis and oesophageal ulceration at the lower oesophagus, which was biopsied. Histopathology demonstrated active chronic inflammation, apoptotic keratinocytes, and reactive changes. In the absence of infection, clinicopathological correlation with nivolumab therapy raised suspicion of nivolumab associated oesophagitis. This is a rare case of Nivolumab associated oesophagitis 4 years after its commencement. Due to the rarity of nivolumab induced oesophagitis, management remains largely non-specific with proton pump inhibitors and oral steroid therapy, with severe cases resulting in cessation of treatment. Fortunately, her symptoms improved with proton pump inhibitors and prednisolone, therefore she was able to continue Nivolumab, with a plan to repeat upper endoscopy soon.
403
Systematic review and meta-analysis of the correlation between upper gastrointestinal mucosal thickening on CT and the endoscopic findings
Hydar El Jamaly1, Osamah Al-Obaidi2, Noureddin Al-Hajjiri1 and Mouhannad Jaber1
1Wollongong Hospital, Wollongong, Australia;2Concord Hospital, Concord, Australia
Background and Aim: Upper gastrointestinal (UGI) mural thickening (MT) is often reported on standard CT examinations of the abdomen. It often presents a dilemma for the clinician on whether any further evaluation is needed, especially in the absence of any set guidelines. To evaluate the significance of UGI MT and to assess its correlation with upper Endoscopy.
Methods: We conducted a comprehensive literature search using a strategy in Medline and this was extended to PubMed and Embase. The studies included patients with UGI MT on CT scans, who underwent endoscopic evaluation. We used a random-effects model using pooled positive predictive value (PPV) with 95% confidence intervals (CI). MT was defined as 5mm or above in the Oesophagus and Stomach, and 3mm or above in the duodenum.
Results: A total of 11 cohort studies examining 855 patients were selected having undergone both CT and upper Endoscopy. Of the 855 patients with MT, 753 had an abnormal upper Endoscopy. In the presence of MT, the pooled PPV for malignancy was 0.21 (95% CI: 0.11-0.36), 0.35 (95% CI: 0.23-0.50) and 0.28 (95% CI: 0.06-0.69) for the Oesophagus, stomach and duodenum respectively (Figure 1). In the presence of MT, the pooled positive predictive value (PPV) for all pathology at upper Endoscopy was 0.84 (95% CI: 0.72-0.91), 0.86 (95% CI: 0.72-0.94) and 0.50 (95% CI: 0.20-0.80) for the Oesophagus, stomach and duodenum respectively (Figure 1).
Conclusion: Gastrointestinal Mural thickening (MT) detected on CT scans has a high positive predictive value of finding abnormalities during an upper endoscopy, including potential malignancies. Additional endoscopic confirmation is warranted upon identifying MT on CT examinations. More data with larger sample sizes that accurately define MT and other associated radiological findings are needed.
409
Long-term outcomes of patients undergoing capsule endoscopy in the investigation of suspected small bowel bleeding
Isaiah Tambyrajah1,2 and Robert B Feller1,2
1Department of Gastroenterology & Hepatology, St Vincent's Hospital, Sydney, Australia;2Faculty of Medicine and Health, University of New South Wales, Sydney, Australia
Background and Aim: The long-term outcomes (greater than five years) of patients undergoing small bowel capsule endoscopy (SBCE) for suspected small bowel bleeding (SSBB) remain unclear. This study sought to determine the long-term rebleeding rate and predictive factors for rebleeding in patients investigated for SSBB.
Methods: This single-centre, retrospective cohort study followed up patients (n = 64) who underwent SBCE between March 2015 and December 2017 at a tertiary hospital in Sydney, Australia by utilising medical records and phone consultations. The Cox proportional hazards model was utilised to evaluate predictive factors of rebleeding, and Kaplan-Meier survival curves to analyse cumulative rebleeding rates.
Results: Sixty-four patients were included in the analysis. The cumulative rebleeding rate in patients with SSBB was 49.1% (28/57) over a mean follow-up of 81.8 ± 10.3 months. Multivariate analysis using the Cox proportional hazards model revealed that an initial haemoglobin (Hb) less than 100 g/L (hazard ratio [HR] 3.615, 95% confidence interval [CI] 1.454-8.989, p = 0.006), positive SBCE study (HR 22.452, 95% CI 1.312-384.336, p = 0.032) and chronic kidney disease (HR 14.611, 95% CI 1.143-186.838, p = 0.039) were predictors of rebleeding. The rebleeding rate amongst patients with a negative SBCE study was 16.7%.
Conclusion: Rebleeding is common during the long-term follow-up of patients assessed for SSBB. Negative SBCE is not a definitive predictor of event-free survival. Diligent follow-up is necessary, especially for patients presenting with low initial Hb and positive SBCE findings. Patients presenting with iron deficiency without significant anaemia should undergo a period of iron supplementation before SBCE.
433
Safe and effective endoscopic mucosal resection of large premalignant colorectal polyps in a regional centre
Daniel Yee Lee Ng1, Yoland Hsia2, Aqsa Farooq2, Tania Chapman1, Daniel Saitta1, Sajith Kattiparambil Gangadharan1, Jong Chin1, Maree Pekin1, Timothy Elliott1 and Dileep Mangira1
1Grampians Health, Ballarat, Australia;2Deakin University, Ballarat, Australia
Background and Aim: Endoscopic Mucosal Resection (EMR) is the current standard of management for large premalignant colonic polyps. EMR is typically performed at tertiary centres because of the required advanced endoscopic skills and need for adequate surgical support. Patients in regional and remote areas have a higher incidence of, and worse prognosis from, colorectal cancer, when compared with metropolitan patients. They often do not gain access to optimal care because of their remote geographical location. We developed a regional centre colorectal EMR service to improve access to these services for patients from regional and remote areas. The aim of this study was to assess the safety and efficacy of a regional colorectal EMR service.
Methods: Data were retrospectively obtained via diagnostic coding for colonoscopy with polypectomy on ENDOBASE at a single regional centre between January 2021 and December 2022 for two experienced endoscopists with tertiary centre EMR training. Medical file review identified EMRs by confirming the performance of a submucosal lift prior polypectomy. We collected data relating to the patient (demographic details), the polyp (site, size, Paris, Kudo classification and histology), the EMR procedure (use of hot/cold snares, piecemeal/en bloc resections and complications) and 1st surveillance colonoscopy (timing and presence/size of polyp recurrence). Polyps ≤10mm were excluded.
Results: 189 colonoscopies with polypectomy were identified during the study period. Medical file review identified 84 patients (mean age 65 +/- 12.3 years) who underwent EMR for polyps > 10mm. In 2 of these patients, EMR was abandoned because of suspected cancer (n=1) (confirmed histologically) and poor elevation (n=1) (technical success: 82/84=98%). A total of 103 lesions were resected (1 patient with 4 lesions, 1 patient with 3 lesions, 14 patients 2 lesions, 68 patients with 1 lesion). Mean polyp size was 23mm +/- 10mm. Paris classification was as follows: 0-IIa (58/103), 0-Is (12/103), 0-Ip (4/103), 0-IIa/Is (4/103), 0-Isp (1/103), others (24/103). Kudo pit pattern was as follows: II (31/103), IV (27/103), III L (10/103), III S (9/103), III (7/103), unspecified (19/103). Histopathology of EMR resected polyps was as follows: tubulovillous adenomas (TVA) (45/103), sessile serrated lesions (SSL) (40/103), tubular adenomas (TA) (16/103), and others (2/103). 14/103 lesions had high-grade dysplasia. No cancer was identified. Procedural complications were identified in 4 patients (4/93=4.3%). There were 2 episodes of per rectal bleeding (2/93=2.15%) - one requiring intervention with endoclips. There were 3 episodes of self-resolving abdominal pain (3/93=3.2%) (1 patient with both per rectal bleeding and abdominal pain). There were no perforations. To date, 55/84 patients who underwent EMR have had a first surveillance colonoscopy at a median interval of 11 months. 52/55 patients had no polyp recurrence and there were no interval cancers identified. Of the 3/55 (5.5%) with polyp recurrence, all were easily resected with a cold snare.
Conclusion: EMR of large premalignant colonic polyps can be performed safely and effectively in a regional centre. This helps address the well-documented inequity of care delivery for patients from regional and remote areas with precancerous polyps.
434
White patch with malignant potential: incidental finding of oesophageal leukoplakia at oesophagogastroduodenoscopy
Christopher James Shephard and Bulent Baran
Department of Gastroenterology and Hepatology, Townsville University Hospital, Townsville, Australia
Introduction: Oesophageal leukoplakia, also known as oesophageal epidermoid metaplasia, is a rarely encountered and likely under-recognized entity in endoscopic practice, with an estimated prevalence of 0.19%. Akin to the oral form, it is associated with tobacco and alcohol exposure, although chronic oesophageal irritation from acid reflux is also postulated. It is associated with progression to oesophageal squamous cell dysplasia and squamous cell carcinoma (SCC), although the natural history is less well-described than its oral counterpart. Presentation may be incidental/asymptomatic, or otherwise with dysphagia/odynophagia or globus sensation. It typically manifests in the mid-oesophagus as a translucent white well-demarcated metaplastic patch/plaque. Characteristic histological findings include hyperorthokeratosis, hypergranulosis and epithelial metaplasia. Detection may pose management dilemmas in the absence of recognised guidelines for surveillance and treatment. This case report serves to improve awareness of this rare, yet clinically significant pre-malignant oesophageal lesion.
Case report: A 55-year-old man with a history of long-term alcohol abuse, tobacco smoking, GORD with Barrett’s metaplasia and hypovitaminosis D was referred for an opinion on newly detected liver cirrhosis on ultrasound. Oesophagogastroduodenoscopy (OGD) three years prior demonstrated LA grade A reflux oesophagitis at the gastro-oesophageal junction, short-segment Barrett’s metaplasia C1-M2 in the distal third of the oesophagus and an absence of oesophageal varices. He denied dysphagia or weight loss but did report intermittent bowel habit with melaena in recent months without an associated anaemia. He was non-compliant with previously prescribed proton-pump inhibitor (PPI) therapy. He proceeded to OGD for varices screening, Barrett’s surveillance and evaluation of suspected upper gastro-intestinal bleeding. Examination findings were pertinent for LA grade C reflux oesophagitis and short-segment Barrett’s metaplasia (consistent with previous) without varices, plus the interval finding of a suspicious fixed, white granular-appearing patch of mucosa in the mid-oesophagus concerning for leukoplakia which was biopsied (figure 1A). Distal examination revealed erosive gastropathy and a Forrest IIc duodenal ulcer. The patient was recommended high-dose PPI therapy and eight-week follow-up endoscopy. Histopathology of the suspicious oesophageal lesion proved consistent with oesophageal leukoplakia, demonstrating prominent hyperkeratosis and glandular metaplasia without dysplasia/neoplasia (figure 1B). Subsequent OGD examination revealed stable leukoplakia (figure 1C) with resolving oesophagitis and duodenal ulceration. A plan for close endoscopic follow-up, as opposed to endoscopic ablation/resection, was enacted considering the patient’s other strong indications for repeat OGD examinations.
Conclusion: Oesophageal leukoplakia is a rare yet easily recognisable endoscopic entity that may progress to dysplasia and SCC. In the absence of standardised treatment guidelines, clinician discretion regarding either close follow-up or early endoscopic therapy is advised in view of the neoplastic potential. Improved understanding of the natural is necessary to inform best practice management.
435
Evaluation of the safety and quality of operator delivered conscious sedation colonoscopy by nurse practitioner endoscopists
Grace Magnani, Kylie Ashley and John Masson
Townsville University Hospital, Townsville, Australia
Background and Aim: Sedation models for colonoscopy vary from conscious sedation provided by the proceduralist, to deep sedation provided by an anaesthetist. In 2018 two Nurse Practitioner Endoscopists (NPE) in a regional hospital were formally trained and successfully credentialed by their health service to perform colonoscopy procedures and concurrently administer conscious procedural sedation using intravenous fentanyl and midazolam for low risk patients (American Society of Anaestheologists ASA 1-2). The NPE model complements the existing medical endoscopy service that routinely uses conscious procedural sedation to perform colonoscopy procedures. A hospital procedure outlining a clear NPE scope of practice was developed guided by the Australian and New Zealand College of Anaesthetics (ANZCA) PG09(G) Guideline on procedural sedation 2023 (formerly PS09, 2014). The aim of this evaluation is to demonstrate within a large cohort of patients that the NPE as operator sedationist is safe and able to complete routine high quality colonoscopy procedures on low risk patients. We believe this is the first health service in Australia where NPE were credentialed as operator sedationists.
Methods: A retrospective audit using prospectively collected demographic and clinical data. Data was obtained from Endoscopy Services Information System Solution (ESSIS) Provation® MD database and the integrated electronic Medical Record (iEMR) between June 2018 and December 2023. Project approval was through the Hospital and Health Service Audit, Quality and Innovation Review Panel.
Results: Between June 2018 to December 2023, 4419 patients had colonoscopy with the NPE. Total of 4339 (98%) patients having colonoscopy were sedated by the NPE as operator sedationist. Overall caecal intubation rate (CIR) 98%, mean age 57 (range 18-83 years), 45% female. Pre-anaesthesia risk ASA 1 (healthy) 1221 (28%), ASA 2 (mild systemic disease) 3007 (68%), ASA 3 (severe systemic disease) 192 (4%). ASA 3 cases were discussed with a senior consultant prior to sedation administration. Overall total (all ages, including non intact, excluding IBD) adenoma detection rate (ADR) 53%, Sessile Serrated Lesion (SSL) detection rate 15%. Of the cohort of patients > 50 (2884), CIR 98%, ADR 62%, SSL 14%.
Overall mean total sedation dose, (range) fentanyl 106mcg (50-200mcg), midazolam 3.5mg (0.5-7mg). Doses titrated over fentanyl 150mcg and midazolam 5mg were discussed with a consultant prior to administering. Fifteen non serious complications (Table 1). No patients required reversal agents or Medical Emergency Team (MET) calls. Of 77 patients having unsedated colonoscopy, the ileum/caecum were intubated in 72 (94%), 4 (4.7%) aborted due to intolerance, 1 (1.3%) incomplete due to obstructing mass. Three (0.06%) patients had colonoscopy with sedation augmented by medical staff due to significant co-morbidites/high risk.
Conclusion: NPE operator sedationist procedures delivers safe, quality colonoscopy procedures. NPE as operator sedationist for colonoscopy procedures using fentanyl and midazolam is a viable and safe option to access routine, low risk colonoscopy. Cost analysis and patient satisfaction studies are currently underway.
438
Quality and safety of colonoscopy delivered by nurse practitioner endoscopists in a regional hospital in Queensland – a service evaluation
Kylie Ashley, Grace Magnani and John Masson
Townsville University Hospital, Townsville, Australia
Background and Aim: In Australia the demand on colonoscopy services continues to increase driven by the National Bowel Cancer Screening Program (NBCSP) and consequent polyp surveillance. During the same period there has also been increased focus by both providers and patients on the quality and safety of colonoscopy services. This led to the development and implementation of evidence based, measurable key performance indicators (KPI). In 2018 two Nurse Practitioner Endoscopists (NPE) were credentialed by Queensland Health to deliver conscious procedural sedation colonoscopy as operator sedationist within a regional Queensland public hospital. The aim of this study is to evaluate the quality and safety of the NPE service.
Methods: Retrospective audit of prospectively collected demographic and clinical data obtained from Endoscopy Services Information System Solution (ESSIS) ProVation® MD database and integrated electronic Medical Record (ieMR) between June 2018 and December 2023. Data relating to specific KPIs presented in the National Colonoscopy Clinical Care Standard 2020 (Australian Commission of Safety and Quality in Health Care) were collected. The 30 day hospital readmissions, complications and mortality were independently reviewed. Project approval was through the Hospital and Health Service Audit, Quality and Innovation Review Panel.
Results: We report the first 5.5 years of the NPE service. Total 4419 patients underwent colonoscopy with operator delivered conscious sedation representing approximately 40% of colonoscopy performed in the unit. Mean age 57 (range 18-83 years), females 45%. ASA 1 1221 (28%), ASA 2 3007 (68%), ASA 3 192 (4%). Overall caecal intubation rate 4210 (98%). Procedures not completed to caecum or requiring a further follow up procedure are listed (Table 1). Patients >50 years, intact colons and excluding inflammatory bowel disease (IBD) (2884), adenoma detection rate 62% (1795), sessile serrated lesion rate 14% (409), adenocarcinoma 2% (51). Fifteen recorded immediate complications (Table 2), resulting in one overnight admission for observation after control of a polypectomy related bleed. Six hospital re-presentations for procedure related or possibly related events within 30 days post colonoscopy, all were considered minor events. One 30 day mortality was due to a CVA in a known arteriopath presenting at day 28 post colonoscopy. On review this was judged not to be procedure related.
Conclusion: NPE can deliver safe, high-quality colonoscopy. The findings of this evaluation support the vision for expanding NPE services to help meet the demand for safe, effective colonoscopy.
442
EXPLORE AI-BO Study: Exploring endoscopists’ knowledge, perception and attitude towards artificial intelligence in endoscopic surveillance for Barrett’s oesophagus
Nicholas Wan1,2, Jin Lin Tan1,2, Celine Chan1, Mohamed Asif Chinnaratha1,2 and Rajvinder Singh1,2
1Gastroenterology Department, Lyell McEwin Hospital, Adelaide, Australia;2Adelaide Medical School, University of Adelaide, Adelaide, Australia
Background and Aim: Artificial Intelligence (AI) has been shown to assist endoscopists in detecting early neoplasia in Barrett’s oesophagus (BO). This questionnaire aims to explore endoscopists’ knowledge, perception, and attitude towards AI in BO, providing insights into factors impacting the translation of such models into clinical practice.
Methods: An online questionnaire was developed and disseminated to one hundred and forty endoscopists across South Australia. Descriptive statistics were used to summarise the results.
Results: Twenty participants completed the questionnaire, including gastroenterologists (50%), surgeons (30%), and trainees (20%). Overall, participants exhibited positive attitudes on the validated Artificial Intelligence Attitude Scale (AIAS-4), with a mean score of 17.5 (SD = 2.3) out of 20. Domain 1 – Knowledge and Perception Towards AI in Endoscopy: 15% of respondents reported having adequate knowledge of AI application in BO. This compared unfavourably to colorectal polyp detection (60%). However, 85% of participants were willing to use AI for BO surveillance. Domain 2 – Knowledge and Perception Towards AI in BO-Surveillance: White-Light-Imaging (60%) and Narrow-Band-Imaging (55%) were the top two imaging modalities where respondents had some knowledge of AI applications in BO-surveillance. All respondents preferred AI models capable of supporting multiple-imaging modalities. Participants perceived that AI will improve the detection rates of low-grade dysplasia (90%), high-grade dysplasia (95%) and early oesophageal cancer (85%). Domain 3 – Impact on Patients: 50% of respondents anticipated that AI would reduce the frequency of endoscopic surveillance. 60% of respondents indicated that using AI would improve therapeutic relationships with patients. Domain 4 – Impact on Endoscopists: Respondents indicated that AI could extend the duration of procedures (75%). While some suggested an increase in fatigue (25%), others believed it decreases fatigue (50%). Domain 5 – Impact on Clinical Practice: All respondents expressed confidence that AI would enhance their accuracy in dysplasia detection. 70% of respondents indicated their preference to perform random oesophageal biopsies even if AI has >95% sensitivity for detecting early Barrett’s dysplasia. Domain 6 – Medico-legal Concerns: Without clear regulation, only 50% of respondents are open to using AI in endoscopy. Accountability of missed lesions was felt to be the responsibility of endoscopists (70%) rather than AI (5%).
Conclusion: Endoscopists showed positive attitudes towards integrating AI in BO-surveillance, especially regarding the perceived improvement in detecting early dysplasia. This questionnaire highlights concerns including liability, procedural duration, and its lack of clear regulation.
454
Implementation and evaluation of unsedated transnasal endoscopy: an efficient solution for increasing demand for upper gastrointestinal endoscopy?
Lea Wiggins1, Rhian Jones2, Angela Carberry2 and James O'Beirne1
1Sunshine Coast University Hospital, Birtinya, Australia;2Sunshine Coast Health Institute, Birtinya, Australia
Background and Aim: The demand for procedures such as upper gastrointestinal endoscopy is increasing, driven by population growth, higher rates of chronic disease, an ageing population, with the rate of individuals over 70 years in our health district being 40% higher than the Queensland average. Traditionally, upper gastrointestinal endoscopy procedures at our health service have relied heavily on anaesthetists for procedural sedation. However, alternative models such as Unsedated TransNasal Endoscopy (UTNE) offer a potential solution to reduce reliance on anaesthetists and ancillary staff, improve patient flow, shorten waitlists and increase patient convenience. UTNE uses an ultrathin endoscope inserted through the nasal passage following topical anaesthesia, avoiding the need for sedation and reducing the number of procedural healthcare professionals required. Recent technological advancements have improved the utility and image quality of transnasal endoscopes, making UTNE a viable alternative to traditional methods.
Methods: A mixed-method evaluation approach was used, combining quantitative and qualitative data. Procedural data was collected from hospital electronic medical records and surveys were disseminated to collect patient and clinician experience measures.
Results: Forty-seven UTNE procedures were completed, with a median procedure time of 6.7 minutes (SD ± 2.8 minutes). In all cases Olympus XP190N gastroscopes (5.4mm outer diameter) were used. The oldest pt was 91 and youngest 24 years of age. The mean age of patients was 55 years (SD ± 15.8 years), with more female patients (n=25) than male patients (n=22). In three cases the procedure was converted to an oral approach due to unfavourable nasal anatomy. Indications for endoscopy were, evaluation of reflux symptoms (39%), dysphagia (23%), eosinophilic oesophgitis (9%), Barretts oesophagus (4%) and others (25%). No procedural complications, emergency department presentations within 72 hours post-procedure, or mortalities were reported. Clinical records indicated no adverse outcomes related to the UTNE procedures. Patient satisfaction was generally high, with positive feedback highlighting personalised care and professional, caring staff. However, some patients expressed uncertainty regarding biopsy outcomes and the communication of results. Specific survey results indicated that all respondents (n=7, 7% response rate) rated the overall care received as very good, appreciated the clear communication from healthcare professionals, and felt involved in decision-making about their care. Most patients felt they had the procedure as soon as necessary (86%), received adequate information to prepare (71%), had the opportunity to ask questions (86%), were informed about post-procedure expectations (80%), and did not experience long waits at the clinic (71%). Half of the patients (50%) experienced some discomfort during the procedure, although this was reported as being less or much less than expected. Majority of patients reported that they did not take any time off work to attend the procedure (60%), and all patients reported that they did not require another person to take time of work to support them to attend their endoscopy appointment.
Conclusion: The UTNE model demonstrated safety and high patient satisfaction, reducing the need for sedation and the number of healthcare professionals involved in upper gastrointestinal procedures. Despite the positive outcomes, challenges such as data accuracy and communication of biopsy results need to be addressed to improve the model’s effectiveness and scalability. Further training of proceduralists and enhancements in data management are recommended to support the broader implementation of UTNE. Addressing these challenges will ensure more efficient and effective patient care, ultimately contributing to the sustainability of healthcare services in the face of rising demand and workforce shortages.
457
Adherence to therapeutic gastroscopy guidelines for acute esophageal food bolus impaction: impact on adverse outcomes and length of stay
Fei Yang Pan1, Tuan Anh Duong2, Kimberley Davis2, Claudia Rogge2 and Matthew Smale3
1Macquarie University Hospital, Sydney, Australia;2Wollongong Hospital, Wollongong, Australia;3Liverpool Hospital, Sydney, Australia
Background and Aim: According to the European Society of Gastrointestinal Endoscopy (ESGE), gastroscopy should be conducted within 6 hours for complete obstruction and 24 hours for incomplete obstruction due to food bolus impaction. This study explores whether adults with acute esophageal food bolus (FB) impaction experience adverse outcomes when their time to esophagogastroduodenoscopy (EGD) deviates from the recommended guidelines.
Methods: A retrospective review was performed on the records of 248 patients who presented at the study site between 2015 and 2022 with symptoms of FB impaction. Local endoscopy software was used to identify patients meeting the inclusion criteria and data was extracted from the patients’ electronic medical records. Age, sex, timestamps (patient reported FB ingestion, ED presentation, EGD and discharge), type of FB, glucagon usage, evidence of complete obstruction (defined as an inability to swallow saliva), biopsy status and results, endoscopic technique, and complications were collated. Time between ingestion and ED presentation, ED presentation and EGD, EGD and discharge and overall length of stay (LOS) were calculated. Complications were categorized into grades with aspiration as a separate category. Statistical analysis was conducted using RStudio V4.1.
Results: 248 patients underwent EGD for FB impaction. Grade 1 (erosion, ulceration), grade 2 (tear) and grade 3 (perforation) complications were present in 31.6%, 6.9% and 0.8% of cases, respectively. Of the 134 (54.0%) patients with complete obstruction, 51 (38.1%) received EGD within the recommended 6 hours. Whilst of the 114 (46%) patients with incomplete obstructions, 93 (81.6%) received EGD within the recommended 24 hours. There was no statistically significant correlation between LOS post-EGD and any of ingestion to presentation time, presentation to EGD time or ingestion to EGD time. Age and complication level were greater predictors of longer LOS than presentation to EGD time. Patients who presented in hours were significantly more likely to receive EGD within the 6- and 24-hour guidelines than those that presented out of hours (50.7% versus 22.0%).
Conclusion: Further prospective, multi-center studies may evoke a revision of the current ESGE guidelines on time to EGD for FB impaction. While the importance of prompt therapeutic EGD is necessary for patient comfort, our study did not illustrate a reduced complication rate, complication grade or post-EGD LOS by doing so. Continued research is needed to optimize patient care and outcomes in cases of FB impaction.
465
Pop, drop and pull: A case report of acute gastric outlet obstruction secondary to bariatric intragastric balloon requiring endoscopic removal
Ayrton Sheehan and Rohit Gupta
Sunshine Coast University Hospital, Birtinya, Australia
Introduction: Bariatric intragastric balloons have emerged in clinical practice for obesity management as a primary strategy for weight loss, or as a bridge to bariatric surgery. Intragastric balloons are inserted endoscopically, or with radiological guidance, under the direction of a bariatric weight loss surgeon or clinic. We present a case of acute gastric outlet obstruction secondary to bariatric intragastric balloon to raise awareness of this complication, and to describe the endoscopic management for the on-call gastroenterologist.
Case report: A 33 year old female presented to hospital with a two day history of escalating epigastric abdominal pain with associated nausea, vomiting and severe regurgitation. Three days prior, the patient had a radiologically placed intragastric inflatable balloon as a weight loss strategy for obesity. Her current weight was 95kg. She had a previous bariatric intragastric balloon resulting in 15kg weight loss over a 4 month period. There were no symptoms associated with the previous intragastric balloon, and it self-deflated after 16 weeks and was spontaneously passed rectally. On clinical examination, the abdomen was soft and non-tender to palpation. Biochemical testing demonstrated a raised serum creatinine at 87 μmol/L and a normal lipase at 33 unit/L. Evaluation with computed tomography abdominal imaging demonstrated a fluid filled intragastric balloon measuring 12cm x 9cm x 10cm with estimated volume of 540ml. There was no imaging evidence of pancreatitis or perforation. Endoscopic assessment revealed retained gastric contents related to gastric outlet obstruction secondary to the intragastric balloon (see Figure 1). The gastric contents were suctioned, and a needle was passed through the gastroscope and inserted into the intragastric balloon for deflation with a combination of manual and wall suction of the balloon’s contents. Following deflation, the balloon’s edge was grasped with a snare and removed.
Conclusion: Intragastric balloons are becoming more prevalent as a management strategy for obesity. Gastroenterologists are likely to encounter complications of bariatric intragastric balloons more frequently in clinical practice into the future. Understanding the possible complications and their management is important for future care of these patients.
476
Over the scope clip as first or second-line endoscopic therapy in acute non-variceal upper gastrointestinal bleeding
Khaliun Batkhurel, Mohammad Shir Ali, Lay Theng Gan, Mark Loewenthal, Randy Tjang, Donna Gilles and Steven Bollipo
Department of Gastroenterology, John Hunter Hospital, Newcastle, Australia
Background and Aim: The over the scope clip (OTSC) can potentially overcome limitations of standard clips and achieve reliable haemostasis. This is due to its ability to achieve larger mucosal approximation and capture deeper tissue layers. Recent studies have shown that OTSC is effective in achieving hemostasis for refractory upper GI bleeding. The aim of this study is to evaluate outcomes of OTSC as first and second line therapy for management of acute NVUGIB at our institution.
Methods: We prospectively and retrospectively collected and analysed our database from January 2019 to May 2024 from all patients who underwent emergency gastroscopy for NVGIB. The patients’ clinical demographics were obtained from patient records. We also looked at patients’ comorbidities, including their use of anticoagulation and antiplatelet agents.
Results: 52 patients underwent a gastroscopy with OTSC insertion as either first line (n=42) or second line (n=10) endoscopic treatment. Culprit lesions were in the antrum (n=8), gastric body (n=2), first part of duodenum (n=37), and second part of duodenum (n=7). Successful haemostasis at endoscopy was achieved in 44/52 (84.6%). OTSC as first-line therapy had a primary success rate of 37/42 (88%) while as second-line therapy the success rate was 7/10 (70%). Rebleeding after successful endoscopic haemostasis occurred in 6/52 patients (Table 1). In total, 11/52 (21%) patients failed endoscopic treatment and progressed to surgical management (n=5) or interventional radiology (IR) intervention (n=6). We found that of patients who rebled after OTSC, there is a clear leader in NSAID being the primary cause. Technical issues with deployment of OTSC occurred in three cases. One resulted in deployment in the oesophagus, one could not be deployed to the culprit lesion, and one could not be passed down to the culprit lesion due to a proximal stenosis. There was one case of mortality within 30 days. This patient had a through the scope (TTS) clip and adrenaline injection as first line treatment followed by OTSC as second-line which failed necessitating IR intervention.
Conclusion: OTSC treatment is an effective and feasible treatment for GI bleed, as first line treatment. This effectiveness is particularly notable given that OTSC is typically reserved for larger and more high-risk lesions. Despite being a relatively new technology, and hence less familiarity among endoscopists, technical failures during deployment are uncommon. However, it's important to consider factors such as oesophageal stenosis, which may impede the deployment of the OTSC.
484
Those that are not measured suffer: the case for measuring colonoscopy adenoma detection rate in all patients regardless of age
Zainul Azhar1,3, Simone Kefford2, Torsten Pennell2,3, Chanuli Jayasena3, Sophie Jensen2, Taylor Gilbert2, Andrew Saunders2, Daniel Worthley2 and David Hewett2,3
1QEII Jubilee Hospital, Brisbane, Australia;2Colonoscopy Clinic, Brisbane, Australia;3Faculty of Medicine, The University of Queensland, Brisbane, Australia
Background and Aim: The incidence of colorectal cancer (CRC) in ages < 50 years is increasing globally. Australian guidelines have endorsed a reduced age of screening initiation, now recommended from age 45. The Hawthorne effect of measuring and reporting ADR motivates endoscopists to perform high quality colonoscopy. However, adenoma detection rates (ADR) are currently only measured in patients aged ≥50 years. This study aimed to assess the impact of measuring and reporting ADR in patients aged 45-49.
Methods: We conducted a prospective observational study from July 2021 to April 2024 of 16,782 consecutive colonoscopies performed in a large private community clinic in Brisbane. Eligible patients were aged ≥15 years and referred for elective colonoscopy. Exclusion criteria were inflammatory bowel disease, previous colonic resection and incomplete colonoscopy. From July 2021, each doctor received a quarterly report card of colonoscopy quality metrics, including intubation rates, insertion/withdrawal times and detection rates (cancer, adenoma, sessile serrated lesions) for themselves and for all doctors. ADR was reported in patients aged >50 (ADR50). From 1 March 2024, report cards were modified to report ADR in patients aged >45 (ADR45), between 45-49 (ADR45-49) and >50 (ADR50). To assess the impact of the observation of colonoscopy quality in younger patients, we compared ADR before and after 1 March 2024. Outcome measures were ADR45, ADR45-49, and ADR50.
Results: Overall, ADR in ages 50-54 was 10% higher than in ages 45-49, compared to mean increments of 4.5% for each 5-year increase in age between 40 and 84 years (Figure 1). There was no difference in ADR50 before and after the change in report cards (69.1% vs 69.9%, p 0.66). However, there was a numerical (but not significant) increase in ADR45-49 (46.7% vs 50.6%, p 0.48), which was less for ADR45 (66.8% vs 67.4%, p 0.74).
Conclusion: The inclusion of ADR in quarterly colonoscopy report cards may improve colonoscopy quality in patients aged 45-49, leveraging the power of the Hawthorne effect. Further longitudinal and larger studies are required.
485
The clinical value of "exception item" colonoscopy (MBS Item 32228) and predictors of advanced neoplasia
Zainul Azhar1,3, Simone Kefford2, Torsten Pennell2,3, Chanuli Jayasena3, Sophie Jensen2, Taylor Gilbert2, Andrew Saunders2, Daniel Worthley2 and David Hewett2,3
1QEII Jubilee Hospital, Brisbane, Australia;2Colonoscopy Clinic, Brisbane, Australia;3Faculty of Medicine, The University of Queensland, Brisbane, Australia
Background and Aim: Most colonoscopies in Australia are subsidised by the Medicare Benefits Schedule (MBS). In November 2019, the MBS introduced an “exception” item (32228) for clinically indicated colonoscopy not covered by other item numbers. Item 32228 is available for a given patient only once. It has been suggested that item 32228 could be removed from the schedule. The aim of this study was to assess the rates of neoplasia in 32228 colonoscopies since its inception and determine any predictors of advanced adenomas among these colonoscopies.
Methods: We conducted a prospective observational study from July 2021 to April 2024 of 16,783 consecutive colonoscopies performed in a large private community clinic in Brisbane. Eligible patients were aged ≥15 years, referred for elective colonoscopy, and billed MBS item 32228. Exclusion criteria were inflammatory bowel disease, colonic resection, and incomplete colonoscopy. Outcome measures included adenoma detection rate (ADR), advanced adenoma detection rate (AADR), serrated sessile lesion detection rate (SSLDR) and advanced SSLDR (ASSLDR) We used multiple logistic regression to evaluate predictors of colorectal neoplasia including age, sex, index colonoscopy and indication, and to compare detection rates with non-32228 indications.
Results: There were 1,380 colonoscopies (item 32228) over the 3-year study period. In 32228 colonoscopy, overall ADR, AADR, SSLDR and ASSLDR was 63.6%, 7.0%, 36.1% and 13.70% respectively; cancer was detected in two patients (0.15%). The rates of detection of any advanced polyp (adenoma, SSL) were similar between items 32228 and 32222 (diagnostic procedures: 19.6% vs 19.6%, p=0.99). AADR was lower for item 32228 compared with diagnostic colonoscopy (32222: 6.4% vs 9.0%, p = 0.01), while ASSLDR was similar (13.7% vs 12.0%, p=0.08). Significant predictors for advanced adenomas in ‘32228' colonoscopies were male sex (OR 2.52, p<0.01) and index colonoscopy (OR 2.22, p<0.01). Significant predictors for advanced SSLs were index colonoscopy (OR 1.73, p<0.01) and family history of colorectal cancer (OR 1.39, p=0.04).
Conclusion: This study builds on our earlier report1 confirming the clinical relevance of item 32228 with 1 in 5 “exception” colonoscopies detecting advanced colorectal neoplasia. Clinician discretion remains an indispensible component of the MBS for colonoscopy.
Reference
1.
Lee See, M et al. The clinical value of “exception item” colonoscopy (MBS item 32228). Med J Aust2022; 216: 94-95, doi https://doi.org/10.5694/mja2.51241
487
Age-standardised adenoma detection rate: exploring the concept of monitoring detection rates for patients of all ages
Zainul Azhar1,3, Simone Kefford2, Torsten Pennell2,3, Chanuli Jayasena3, Sophie Jensen2, Taylor Gilbert2, Andrew Saunders2, Daniel Worthley2 and David Hewett2,3
1QEII Jubilee Hospital, Brisbane, Australia;2Colonoscopy Clinic, Brisbane, Australia;3Faculty of Medicine, The University of Queensland, Brisbane, Australia
Background and Aim: Adenoma detection rate (ADR) is the dominant metric for assessing the quality of screening colonoscopy and is inversely related to the risk of post colonoscopy colorectal cancer. ADR is typically measured in patients above 50 years of age. We aim to evaluate the merits of using an age-standardized adenoma ADR as an alternative and inclusive tool for monitoring colonoscopy quality.
Methods: We conducted a prospective observational study from July 2021 to April 2024 of 16,782 consecutive colonoscopies performed in a large private community clinic in Brisbane. Eligible patients were aged ≥15 years and referred for elective colonoscopy. Exclusion criteria were inflammatory bowel disease, previous colonic resection and incomplete colonoscopy. Outcome measures were ADR in patients >50 years (ADR50), >45 years (ADR45) and age standardized ADR (ASADR) of the practice and individual endoscopists. ASADR is the sum of age-adjusted ADR across all age groups, accounting for the standard population proportion.
Results: Overall ADR50, ADR45 and ASADR was 69.2%, 66.9% and 60.2% respectively. ASADR for all five individual endoscopists were related to their ADR50 with a median difference of 9.14%. The highest ASADR was 69.4% which corresponded to the endoscopist’s ADR of 77.8% whilst the lowest ASADR was 47.3% corresponding to an ADR of 54.5%.
Conclusion: Age-standardized ADR is a potential alternative and inclusive marker of colonoscopy quality, which adjusts for patients’ age in ADR calculations. Further research is required to assess its effectiveness for colonoscopy quality monitoring, leveraging the power of the Hawthorne effect.
491
The uptake and barriers to artificial intelligence (AI) use in colonoscopy for polyp detection
Mohammed Affan Guliyara, Martin Grehan and Calvin Chan
Nepean Blue Mountains Local Health District, Sydney, Australia
Background and Aims: The use of Artificial Intelligence (AI) in colonoscopy has shown improvements in polyp detection and characterization, including increased adenoma detection rates (ADR). However, its implementation varies among endoscopists. This study aims to investigate AI utilization in colonoscopy by Australian endoscopists and identify barriers to its routine implementation.
Methods: We conducted a cross-sectional survey, collecting data on endoscopists' demographics, familiarity, experiences, and reservations regarding AI use in colonoscopy, as well as their general attitudes towards AI. The survey responses were measured using 5-point Likert scales.
Results: Fourteen proceduralists participated in the web-based survey. The respondents were predominantly male (n=12; 85.7%), with most holding consultant roles (n=11; 78.6%) and specializing in gastroenterology (n=10; 71.4%). Six had less than 5 years of experience (42.9%), and six had over 10 years (42.9%). The majority (n=13; 92.9%) reported high familiarity with AI. Despite this, routine use of AI in colonoscopy was reported by only 23%, while 15% had never used AI. For those who used AI selectively, it was applied in specific cases such as poor bowel preparation, history of serrated polyps, or frail patients with cardiopulmonary comorbidities. Most respondents (n=11; 78.6%) believed AI would enhance polyp detection and increase the number of polyps removed. However, barriers included prolonged colonoscopy times (n=8; 57.2%), false positives (n=8; 57.2%), distraction (n=5; 35.7%), and forgetfulness (n=4; 28.6%). Regarding general attitudes towards AI, most endoscopists felt that AI would improve the quality of care (n=9; 64.3%) and diagnostic efficiency in the future (n=10; 71.4%). They acknowledged potential biases in AI (n=9; 64.3%) and stressed that clinicians must retain final responsibility (n=14; 100%). Reproducible outcomes were deemed a critical feature for AI implementation (n=10; 71.4%). Learning AI technology was not considered a significant barrier (n=10; 71.4%). Despite its limitations, half of the proceduralists intended to use AI technology routinely in patient care in the future (n=7; 50%).
Conclusion: This study demonstrated that despite high familiarity with AI, its use is limited to selected cases, often hindered by drawbacks such as longer procedure times, false positives, distractions, and forgetfulness. These findings highlight significant barriers to AI adoption among proceduralists at our institution. Addressing these issues can help develop strategies to improve AI uptake during routine colonoscopy.
503
Suboptimal inpatient bowel preparation: using a healthcare redesign approach to explore a challenging gastroenterology issue
Anna McMahon, Kimberley Ryan, Stefanie Ford, Mark Appleyard and Florian Grimpen
Royal Brisbane and Women's Hospital, Brisbane, Australia
Background and Aim: Bowel preparation for colonoscopy is a standard quality metric. Inadequate bowel preparation is a well-described and challenging issue, particularly for the inpatient cohort in gastroenterology. Adequate bowel preparation is paramount for a safe and optimal diagnostic and therapeutic colonoscopy amongst inpatients. The aim of this study was to contextualise the problem of inadequate bowel preparation in a large tertiary referral hospital.
Methods: This study utilised Healthcare Redesign methodology as an action research approach, using exploratory sequential mixed-methods. Data was collected from two sources; qualitative, through an informal staff feedback tool which guided and was followed by a retrospective chart audit (Table 1).
Results: Key themes that emerged from this study included: variation in clinical practice and knowledge, delays and inefficiencies throughout the patient journey, heterogeneity in bowel preparation prescription, documentation and administration of bowel preparation medications and fragmented communication.
Conclusion: This mixed-methods approach has yielded important insights into the potential causes of inadequate bowel preparation amongst a patient cohort undergoing bowel preparation as an inpatient, providing a great opportunity for change. Findings will inform clinical re-design initiatives aimed to target the identified inefficiencies to improve clinical and process outcomes in hospitalised patients undergoing bowel preparation for colonoscopy.
531
Prospective validation of a novel vision transformer model to detect early neoplasia for Barrett’s surveillance: an interim analysis
Jin Lin Tan1,2, Dileepa Pitawela3, Mohamed Asif Chinnaratha1,2, Hsiang-Ting Chen3 and Rajvinder Singh1,2
1Department of Gastroenterology, Lyell McEwin Hospital, Adelaide, Australia;2Faculty of Health and Medical Sciences, The University of Adelaide, Adelaide, Australia;3Australian Institute for Machine Learning, The University of Adelaide, Adelaide, Australia
Background and Aim: Artificial Intelligence (AI) models based on Convolutional Neural Networks (CNN) have been shown to improve detection rates of early Barrett’s neoplasia. However, present algorithms are predominantly trained on white-light imaging (WLI) (1). In addition, models trained on CNN may face issues with scalability as training datasets becomes larger with time. Vision Transformer (ViT) has emerged as the new state-of-the-art deep learning model in the field of computer vision, outperforming CNN models in terms of computational efficiency for larger datasets and accuracy. ViT leverages the power of transformers, using an “attention” mechanism originally designed for natural language processing, for spatial and temporal analysis of images and videos. This study aims to prospectively validate BE-ViT, a pilot ViT model developed to detect early Barrett’s neoplasia on both WLI and narrow-band imaging (NBI).
Methods: The BE-ViT model was pre-trained with ImageNet. We subsequently trained the model on a dataset of 1,918 (275 patients) clinically validated images of Barrett’s oesophagus with and without neoplasia. The training dataset comprised of 835 WLI and 1,083 NBI images. There were 287 WLI and 262 NBI images which contained neoplasia. Patients with Barrett’s oesophagus undergoing endoscopic surveillance from a large tertiary referral centre from Feb 2022 to Mar 2024 were included in this study. The prospective validation dataset comprised of 380 (14 patients) images: 99 (4 patients) neoplastic images and 281 (13 patients, including three patients in the former group after receiving endoscopic eradication therapy) images without neoplasia. The primary outcome was the performance of the BE-ViT model, which was assessed by accuracy, sensitivity and specificity.
Results: BE-ViT achieved the following performances for WLI images (80.4% accuracy, 70.6% sensitivity and 84.9% specificity) and NBI images (78.0% accuracy, 70.8% sensitivity and 80.3% specificity), respectively. Excluding images containing low-grade dysplasia, performance improved for both WLI images (81.2% accuracy, 71.4% sensitivity and 84.9% specificity) and NBI (79.2% accuracy, 75.4% sensitivity and 80.3% specificity).
Conclusion: The pilot BE-ViT model shows promising potential in detecting early Barrett’s neoplasia. This new algorithm is expected to enhance accuracy and outperform current models when trained and refined on larger datasets, marking an important step forward in improving early detection and patient outcomes in patients with Barrett’s oesophagus.
Reference
1. Tan, JL, Chinnaratha, MA, Woodman, R, Martin, R, Chen, H-T, Carneiro, G, et al. Diagnostic Accuracy of Artificial Intelligence (AI) to Detect Early Neoplasia in Barrett’s Esophagus: A Non-comparative Systematic Review and Meta-Analysis. Front Med (Lausanne). 2022 Jun 22; 9:890720.
Christopher James Shephard1, William Jiaen Wang1,2,3 and Bulent Baran1
1Department of Gastroenterology and Hepatology, Townsville University Hospital, Townsville, Australia;2Department of Gastroenterology and Hepatology, Princess Alexandra Hospital, Brisbane, Australia;3School of Medicine, Western Sydney University, Sydney, Australia
Introduction: Candida is a commensurate yeast of the gastrointestinal tract, with colonisation rates up to 20% reported in healthy adults. However, symptomatic oropharyngeal/oesophageal candidiasis may develop in the setting of immunosuppression – namely malignancy and anti-neoplastic therapy. Candida oesophagitis typically presents with dysphagia/odynophagia and typical white/yellow mucosal plaque-like lesions visualised at endoscopy and confirmed on biopsy, however it may also be suspected on imaging performed for another purpose. 18F-fluorodeoxyglucose (FDG) positron emission tomography/computed tomography (PET/CT) is frequently performed in oncology patients for staging and evaluation of treatment response. Abnormal oesophageal FDG uptake with high maximum standard uptake value (SUVmax) may be observed in candidiasis, malignancy and rarely, immune checkpoint inhibitor (ICI)-mediated oesophagitis. To avoid misdiagnosis, unexpected focal and/or intense visualisation of FDG uptake should prompt endoscopic and histological evaluation, especially if SUVmax exceeds 3.5.
Case report: A 54-year-old male with stage IV lung adenocarcinoma receiving maintenance pembrolizumab was admitted from oncology clinic for evaluation of dysphagia/odynophagia with vomiting and 9kg of unintentional weight loss over the preceding month. He also reported pain from several oral mucosal ulcers over the same timeframe, commencing nystatin suspension without clinical improvement. His background was pertinent for lower limb venous thrombosis with pulmonary embolism, hypertension and recent mild hypokalaemia. Current medications included pantoprazole, apixaban, perindopril, oxycodone/naloxone and slow-release potassium. He is an ex-smoker but seldom consumes alcohol. On examination his tongue appeared white-coated without obvious mucosal ulceration. FDG-PET/CT scan five days prior showed no significant pulmonary uptake in keeping with oncological treatment response; however, it highlighted intense tracer uptake throughout the oral cavity and entire oesophagus (Figure 1). Admission investigations showed a leukocytosis of 16.4x109/L, C-reactive protein 24mg/L, potassium 3.1mmol/L and acute kidney injury with creatinine 105micromol/L. Human immunodeficiency virus serology was negative. He received intravenous hydration and potassium replacement. Although there was a high clinical suspicion of oesophageal candidiasis, endoscopy was performed to exclude oesophageal malignancy and ICI-mediated oesophagitis. Oesophagogastroduodenoscopy (OGD) revealed extensive white-yellow plaques throughout the oesophagus (Figure 2). Biopsy demonstrated significant necro-inflammatory debris and inflammation in the setting of fungal hyphae consistent with oesophageal candidiasis, alongside reactive atypia but no neoplasia. The patient completed a 14-day course of fluconazole and amphotericin lozenge (initiated prior to biopsy results) with gradual resolution of symptoms. Nystatin suspension was recommended thereafter to prevent recurrence.
Conclusion: This case highlights the diagnostic challenges of abnormal oesophageal FDG uptake in oncology patients which is non-specific as it can be physiologic, infective, inflammatory or neoplastic in nature. In this case the FDG uptake was due to oesophageal candidiasis and although it was suspected clinically due to its high prevalence among patients with solid organ tumours, FDG-PET/CT cannot reliably exclude crucial differentials. Endoscopic evaluation with biopsy is necessary for diagnostic clarity to guide targeted treatment which in this case was anti-fungal therapy.
543
“Segment anything” with MedSAM: Annotation of Barrett’s dysplasia dataset using artificial intelligence
Jin Lin Tan1,2, Ka Hing Chan3, Dileepa Pitawela3, Mohamed Asif Chinnaratha1,2, Hsiang-Ting Chen3 and Rajvinder Singh1,2
1Department of Gastroenterology, Lyell McEwin Hospital, Adelaide, Australia;2Faculty of Health and Medical Sciences, The University of Adelaide, Adelaide, Australia;3Australian Institute for Machine Learning, The University of Adelaide, Adelaide, Australia
Background and Aim: Expert annotations are vital for developing Computer Aided Detection (CADe) and Diagnosis (CADx) systems in endoscopy. While it is relatively easy for clinicians to draw a "bounding box" around a lesion, the process of outlining the lesion's exact contours, known as "segmentation," is much more time-consuming. Segmentation annotations are especially crucial for highlighting subtle contour irregularities in lesions, such as early Barrett’s dysplasia. MedSAM, a state-of-the-art model trained on 1.5 million images across ten imaging modalities and over thirty cancer types, can automatically assist clinicians in performing various medical segmentation tasks (1). Prior to MedSAM, training segmentation models required laborious per-pixel annotations, whereas MedSAM simplifies the process by needing only a "bounding box" prompt to perform image segmentation, significantly reducing annotation time. In this study, we aim to evaluate the performance of MedSAM on a Barrett’s dysplasia dataset comprising of endoscopic images obtained using Narrow-band imaging (NBI), where lesions have irregular contours and mucosal pit patterns.
Methods: 248 images from 36 unique patients containing Barrett’s dysplasia (high-grade dysplasia and adenocarcinoma) were annotated by experts and verified against histology reports. There were 196 images from 29 unique patients in the training dataset and 52 images from 7 unique patients in the testing dataset. We trained a model using YOLO v8 to localise areas of dysplasia with a bounding box, which MedSAM used for segmentation (see Figure 1). The dysplasia localisation and segmentation accuracy were assessed using the Intersection over Union (IoU) and Dice coefficient scores, respectively.
Results: For Barrett’s dysplasia localisation, our model achieved an average IoU of 71.1%, demonstrating significant overlap between predicted and ground truth bounding boxes. Regarding dysplasia segmentation, an average DICE coefficient score of 71.7% was attained, indicating good precision.
Conclusion: This study demonstrates the potential of using MedSAM to accelerate and scale the annotation of large endoscopic image and video datasets, as well as its applicability to real-time segmentation in endoscopy in the future. Accurate segmentation could also help endoscopists delineate margins better prior to performing endoscopic resection.
Reference
1. Ma, J, He, Y, Li, F, Han, L, You, C, Wang, B. Segment anything in medical images. Nature Communications.2024 Jan 22; 15(1): 654.
548
Lower prevalence of sessile serrated lesions in Asian patients compared to non-Asian patients undergoing bowel cancer screening colonoscopy
Andrew Tang1,2, Jarinya Soieprasounk1, Rachel Halkhoree1, Karen Jones1, Cameron Bell1,2 and Ian Norton1,2
1Ryde Hospital, Sydney, Australia;2Royal North Shore Hospital, Sydney, Australia
Background and Aim: The accurate identification and removal of precursor lesions is fundamental to colorectal cancer screening. Colonic polyps acquire malignant mutations through two pathways - the classic adenoma-carcinoma sequence and the serrated pathway. Adenoma detection rates (ADR) and sessile serrated lesion detection rates (SSLDR) are widely utilised quality indicators of colonoscopy. Mandatory Australian colonoscopy recertification requires proceduralists to demonstrate an ADR of 25% in all patients over the age of 50 with intact colons. An SSLDR of 5% is currently suggested but will soon be another mandatory KPI. These benchmarks are derived from mostly Caucasian-based studies and current ADR and SSLDR recommendations do not account for ethnic differences. We hypothesise that there could be ethnic variations in the prevalence of adenomatous and sessile serrated lesions, particularly in Asian populations, and this could affect colonoscopy ADR and SSLDR in some practice areas.
Methods: We conducted a single-centre retrospective cohort study of patients undergoing colonoscopy following positive faecal occult blood test (FOBT) as part of the National Bowel Cancer Screening Program between November 2021 and October 2023 by two experienced endoscopists. Endoscopy and histopathology reports were reviewed to determine type, size and location of lesions. Ethnicity was based on recorded country of birth with patients born in East Asian and South-East Asian countries being classified as Asian for our study. Incomplete procedures, whether by inadequate bowel preparation or failure of caecal intubation, were excluded from analysis.
Results: A total of 393 patients underwent colonoscopy during the study period including 217 Asian patients (55%) and 176 non-Asian patients (45%). There was no significant difference in baseline characteristics including age and gender. The prevalence of sessile serrated lesions was significantly lower in Asian patients (2.76%) compared to their non-Asian (7.95%) counterparts (P-value = 0.019). By contrast, there was no difference in the prevalence of adenomatous lesions between Asian and non-Asian patients, including in tubular adenoma, advanced adenoma and colon cancer detection.
Conclusion: Current benchmarks for adenoma and sessile serrated lesion detection rates do not account for ethnic variation. Our study demonstrates that sessile serrated lesions were significantly less common in Asian patients compared to non-Asian patients undergoing colonoscopy arising from an FOBT program. This should be reflected in quality indicators used to determine colonoscopy competence in certain practice populations.
549
The yield of endoscopic assessment for iron deficiency in adults
Gary Zhang1, John Olynyk1,2,3,4 and Oyekoya Ayonrinde1,2,3
1Fiona Stanley Hospital, Perth, Australia;2The University of Western Australia, Perth, Australia;3Curtin University, Perth, Australia;4Edith Cowan University, Perth, Australia
Background and Aim: Iron deficiency (ID) is the predominant cause of anaemia and is the commonest micronutrient deficiency worldwide. Age, gender, ethnic background, and severity of ID and/or anaemia (IDA) determine the potential significance, hence the need for targeted investigations to establish an aetiology. Suspected blood loss from the gastrointestinal tract or impaired gastrointestinal absorption are common causes of referral for endoscopic investigation of iron deficiency. Bidirectional endoscopic examination is generally recommended for IDA, as it detects a cause in two-thirds of men and post-menopausal women. There are over 800,000 MBS subsidised colonoscopies per annum in Australia. The diagnostic yield from these when iron deficiency is the primary indication is not known. We aimed to investigate the yield of endoscopic assessment for iron deficiency.
Methods: The electronic endoscopy database at a single metropolitan hospital in Western Australia was retrospectively searched for endoscopic examinations performed for the indications ‘iron deficiency’ and ‘anaemia’ between 1st January 2023 to 31st December 2023. Indications, patient characteristics, diagnostic and therapeutic outcomes of endoscopic assessment, and histopathology results of patients with iron deficiency were extracted from the clinical records of unselected patients.
Results: Of the 250 patients reviewed, 171 (68.4%) had non-anaemic iron deficiency (NAID), 54 (21.6%) had iron deficiency with anaemia (IDA), and 25 patients had anaemia alone or no documented confirmation of iron deficiency. The pathologies identified on endoscopy, stratified by the groups are described in table 1. In the NAID group, the median age was 51 years (IQR 41-63), with 35.1% aged ≤45 years, 71.9% were female, and 90.6% had both gastroscopy and colonoscopy, while 3.51% underwent colonoscopy alone and 5.85% had gastroscopy alone. In the NAID group no patient had colorectal cancer, but one patient had oesophageal adenocarcinoma (0.6%). Other findings included coeliac disease (3.51%), Helicobacter pylori infection (13.5%) and ileal Crohn’s disease (0.6%). In the IDA group, the median age was 49 years (IQR 43-66), with 37% aged ≤45 years, 75.9% were female, and 96.3% had both gastroscopy and colonoscopy. Overall, there was a higher diagnostic yield for potential causes of iron deficiency, using gastroscopy compared with colonoscopy. More malignancies were identified in the IDA group, including oesophageal adenocarcinoma (1.85%), and colorectal adenocarcinoma (3.7%). In patients aged ≤45 years (n=80), the NAID subgroup had 47 females and 13 males; while the IDA subgroup comprised 18 females and 2 males. No malignancies were detected in the young patients, although other pathologies including coeliac disease (7.5%), H pylori (13.75%), and ulcerative colitis (1.25%) were identified.
Conclusion: Most gastrointestinal causes of iron deficiency were detected using gastroscopy. In the absence of specific gastrointestinal symptoms, IDA, or mid-older age, it may be reasonable to initiate endoscopic investigation of iron deficiency with gastroscopy. This two-step approach could be most relevant to patients who have had colonoscopy in the preceding three years. Further larger studies are required to confirm safety and cost effectiveness of this proposed stepwise and/or a serological testing approach in younger patients with NAID.
557
Treatment of haemorrhoids via rubber band ligation followed by pudendal nerve block for analgesia complicated by ischial osteomyelitis: A case report
Jason Zhang, Sarah Taylor, Anil Bhagwat, Christopher Middleton and Brent Mitchell
Royal Hobart Hospital, Hobart, Australia
Introduction: Rubber band ligation (RBL) is a procedure used to treat symptomatic haemorrhoids that have failed conservative management. Post operative pain is very common affecting up to 90% of patients. Subsequently pudendal nerve blocks (PNB) have been increasingly utilised as an adjunct to oral analgesia. We discuss a case of ischial osteomyelitis that is a rare but serious complication post PNB.
Case report: A 53 year old male underwent a colonoscopy for recurrent rectal bleeding. He had no significant medical history, was not immunosuppressed and was not on any regular medications. Rubber band ligation was performed to three columns of large prolapsing haemorrhoids. Bilateral pudendal nerve blocks were performed via a transgluteal technique. The procedure was performed by a senior gastroenterologist with many years of experience performing RBL with PNB. The patient was placed in left lateral position and the perianal area was washed with chlorhexidine. Anatomical landmarks were identified - the ischial tuberosity was palpated percutaneously as was the ischial spine. A 23 gauge needle was inserted percutaneously medial to the ischial tuberosity coursing toward the ischial spine and 20ml of 0.25% bupivacaine injected medial and posterior to the ischial spine. This targets the pudendal nerve as it courses over the sacrospinous ligament and its attachment to the ischial spine into the lesser sciatic foramen. Following the procedure the patient experienced persistent worsening pain and tenderness of the right gluteal region for several weeks. MRI scan showed marrow oedema and swelling within the right ischial tuberosity and oedema of adductor magnus tendon. A subsequent PET/CT showed moderate FDG activity in the right ischial tuberosity with osseous destruction and uptake in the proximal adductor magnus muscle. These findings were suggestive of ischial osteomyelitis and concurrent myositis, likely as a result of inadvertent needle injury to the area and infiltration of local anaesthetic. Further investigations demonstrated a white cell count of 10.3, with neutrophils of 6.7 and a C reactive protein of 15. Multiple sets of blood cultures were negative. Two attempts were made to obtain tissue to confirm osteomyelitis and guide antimicrobial therapy via CT guided biopsy of the ischial tuberosity but unfortunately the samples were non-diagnostic and did not culture an organism. The patient was referred onto the infectious diseases team for consideration of empirical antibiotic therapy. Pudendal nerve blocks are effective in anaesthetising the posterior perineum, anus and genitals and effects are usually noted quickly within 20 minutes. A cross-sectional analysis of RBL for haemorrhoids in Australia accounted for a total of 346542 procedures from 2012 to 2021. Between 2012-13, 1.62% of patients received a PNB compared with 6.63% of patients between 2020-2021. The most common side effect is injection site pain, but other potential complications include bleeding, infection, damage to nerves and surrounding structures and a rare risk of systemic local anaesthetic toxicity. A variety of techniques are utilised including the transvaginal, transperineal, perirectal and transgluteal approach which is often operator dependent. Imaging guidance via ultrasound, CT and fluoroscopy have also been utilised to better delineate underlying structures and avoid injury to surrounding tissue, but this may not be feasible at the time of procedure.
Conclusion: With the increasing utilisation of PNB for anorectal procedures, this case describes an uncommon and serious complication of the procedure which has not been previously described in literature. It highlights the importance of correct identification of anatomical landmarks and aseptic technique in minimising the risk of infective adverse events.
562
Incidental finding of a neuroendocrine tumour on polypectomy
Ruth Ducommun and Myat Khaing and Dennis Rubtsov and Reuben Malloy and Rebecca Cohen and Ayesha Chapagain
The Prince Charles Hospital, Brisbane, Australia
Introduction: Neuroendocrine tumours (NET) are a rare but increasing finding within Queensland. The incidence has tripled from 2 per 100,000 to approximately 6.3 per 100,000 people in 2015 over the last three decades. Rectal NETs are typically 5-10 cm from the dentate line with white or yellow retroflexion. They are poorly recognised with no distinct morphological or pathognomonic features and less than twenty percent of NETs were suspected as such by the endoscopist before a biopsy was performed. Neuroendocrine tumours are found in the lung, appendix, small bowel, pancreas, rectum and can also have an unknown primary site. Most rectal NETs are detected incidentally on surveillance colonoscopy and have a favourable prognosis when fully resected. Endoscopic Mucosal Resection to fully resect the NET is advisable with lesions greater than 3mm, however they are most often found incidentally post-polypectomy. Here in this case, if this NET was not incidentally discovered it would likely have grown and had a far worse prognosis, highlighting the need to biopsy polyps.
Case report: A 53-year-old female underwent surveillance colonoscopy for suspected Sessile Serrated Polyposis syndrome in December 2023. Fifteen polyps were resected, with one 5mm Paris IIa NICE I (hyperplastic appearing polyp) removed with cold snare. The histopathology unexpectedly came back positive for a rectal NET which was 2.3 mm in maximal dimension. It was described as a bland epithelioid neoplasm extending into the lower lamina propria and transected at the lower margin, no invasion into the lymphovascular or perineural invasion was seen. No mitosis or necrosis was found. She had a clear DOTOTATE PET scan and repeat clear colonoscopy, showing no evidence of local recurrence. This confirmed a Grade One rectal NET, Ki67 index <1%, with no nodal metastasis, which has an approximate 100% survival rate at five years.
Conclusion: This case study highlights the lack of distinct morphological characteristics of neuroendocrine tumours and the need for tissue sample to diagnose this rare potentially life-threatening condition. Recurrence post polypectomy of rectal NETs is estimated at five percent, however in one study of 345 patients, this led to two deaths. Endoscopic Mucosal Resection is indicated when the tumour is >3mm, with surgery indicated when the NET is >2cm, or 1-2cm with risk factors such as high mitotic rate on histopathology. Diagnosis is essential for appropriate management. Most NETs have no distinct pathognomonic features with normal overlying mucosa, which complicates detection. Diagnosis of NETs, whilst difficult, is also exceedingly important as early recognition improves survival.
563
Real-time use of artificial intelligence (CADx) on polyp characterisation during colonoscopy: the first Australian trial
Lulu Zhang1,2, Timothy O'Sullivan1,2, Enoka Gonsalkorala1,2, Florian Grimpen1, Guy Lampe1, Sally Roberston1,2, Katherine Hanigan1,2, Lee Jones3, Patricia Valery3 and Mark Appleyard1,2
1Royal Brisbane and Women's Hospital, Brisbane, Australia;2Surgical Treatment and Rehabilitation Service (STARS), Brisbane, Australia;3QIMR Berghofer, Brisbane, Australia
Background and Aim: Colonoscopy is the gold standard for detecting and resecting colorectal polyps, playing a critical role in bowel cancer prevention. The national bowel cancer screening programs has significantly increased the number of colonoscopies performed, impacting the provision of public Gastroenterology services. Accurate polyp diagnosis is essential to avoid unnecessary polypectomies, thereby supporting cost-saving strategies. Examples of these strategies include the “leave-in-situ” approach for hyperplastic polyps ≤5 mm located in the rectosigmoid region and the “resect-and-discard” approach for ≤5 mm proximal polyps. Recent advancements in artificial intelligence (AI) technology, particularly computer-aided diagnosis (CADx) modules, have made these strategies feasible by providing a real-time optical diagnosis, distinguishing between adenomatous and non-adenomatous polyps during colonoscopy. One promising model is the Medtronic GI Genius CADx module, whose effectiveness has been previously studied in Italy and Japan. At present, no Australian studies have evaluated its use in routine colonoscopy practice. Therefore, our aim is to assess the accuracy of real-time CADx during colonoscopy and determine the appropriateness of implementing “leave-in-situ” and/or “resect-and-discard” strategies in an Australian context.
Methods: This is a prospective single-centre study reviewing the Medtronic GI Genius CADx module on polyp characterisation for consecutive patients undergoing colonoscopy over a three-month period. During each colonoscopy, the CADx module provided a real-time optical diagnosis for each visualised polyp. Polyps were then resected and sent to a specialised GI pathologist for histological diagnosis. Statistical analysis was conducted using generalised mixed binary logistic models to determine the sensitivity, specificity, and negative predictive value (NPV) of the CADx module. Diagnostic agreement between optical and histological diagnosis was then assessed using Gwet’s statistics.
Results: We aim to examine 486 polyps in about 244 patients to meet statistical significance. At the time of abstract submission, data collection is still in progress. However, preliminary results will be available by the time of the AGW conference. Based on recent findings from Hassan et al who reviewed the same technology, we anticipate a sensitivity of 82%, a specificity is 93% and NPV of 97.6%. Hassan et al predicted that utilisation of the CADx system had the potential of 44.4% reduction of all polypectomies with the “leave-in-situ” strategy as well as an 83% reduction for need for pathology with the “resect and discard” strategy.
Conclusion: We will be the first Australian study to review the accuracy of CADx in polyp characterisation during real-time colonoscopy, with significant cost-saving potential for the public healthcare system.
567
Caecal Dieulafoy’s lesion – a rare cause of lower gastrointestinal bleeding
Christopher James Shephard and Bulent Baran
Department of Gastroenterology and Hepatology, Townsville University Hospital, Townsville, Australia
Introduction: A Dieulafoy’s lesion (DL) is a dilated aberrant submucosal artery that erodes the overlying epithelium in the absence of a primary ulcer. A DL is implicated in 1-2% of all gastrointestinal (GI) bleeds, of which only 2% involve the colon or rectum. Bleeding is typically associated with older age, cardiovascular disease (CVD), chronic kidney disease (CKD), diabetes, and/or alcohol abuse; anticoagulation further compounds the risk. Per limited reports, caecal DLs usually present with painless haematochezia, although isolated melaena or a mixed bleeding picture is possible. Lesions are difficult to visualise endoscopically owing to their small size/calibre and typical lack of mucosal abnormality, further complicated by inadequate bowel preparation and/or diverticulosis with respect to colonic lesions. Endoscopy is particularly advantageous if performed during acute haemorrhage as active arterial pumping may be observed from an area of mucosa devoid of erosion/ulceration. Endotherapy combining thermal and mechanical haemostatic techniques is favoured over injected monotherapy, owing to lower rates of re-bleeding.
Case report: A 78-year-old woman was referred to hospital by her general practitioner following six days of painless haematochezia and dark stools mixed with bright red blood. Since bleeding onset, she reported light-headedness and worsening of baseline dyspnoea on exertion. Her history was pertinent for nonischaemic cardiomyopathy, slow atrial fibrillation on dabigatran with a pacemaker in situ, diabetes mellitus and CKD stage 3a without any prior GI bleeding. On presentation she was pale and hypotensive with a systolic blood pressure of 93mmHg. Her abdomen was soft and non-tender. Digital rectal examination confirmed melaena mixed with fresh blood. Initial investigations were significant for a haemoglobin of 50g/L and reticulocytosis, normal platelet count and an elevated international normalised ratio of 1.9. Biochemistry highlighted urea of 22.0mmol/L with acute-on-chronic renal impairment evidenced by a creatinine of 135μmol/L (baseline approx. 95μmol/L). Initial resuscitation consisted of intravenous fluid and transfusion of four units of packed red blood cells with subsequent haemoglobin incrementation to 95g/L. Dabigatran was temporarily withheld. Initial upper endoscopy did not identify a bleeding source. Follow-on colonoscopy revealed clotted blood throughout the entire colon and a DL with pulsatile arterial bleeding in the caecum (Figure 1). Haemostasis was achieved using underwater bipolar coagulation probe followed by three haemostatic clips (Figure 2). No active bleeding was evident at procedure close. The patient was monitored in hospital and dabigatran was recommenced after 48hours without concern for re-bleeding.
577
Safety and efficacy of light sedation in low-risk endsocopy
Babak Sarraf, Reffai Syed Mohamed and Seema Shah
Townsville University Hospital, Townsville, Australia
Background and Aim: Multiple models of care exist for delivery of sedation during endoscopic procedures. Light sedation, achieved by administration of fentanyl and midazolam, without additional agents such as propofol, has become increasingly adopted internationally for low-risk endoscopy. As there is limited Australian data, we performed a retrospective study of the safety and efficacy of non-anaesthetist delivered light sedation for endoscopic procedures.
Methods: We undertook a retrospective audit of endoscopy performed under light sedation during 2022 at a tertiary hospital in Queensland, Australia. Ethics approval was obtained. High risk and general anaesthetic procedures were excluded. A random sample of 89 procedures on the light sedation list was analysed for demographics, indication, comorbidities, sedation parameters, procedural challenges and complications. Anaesthetic risk was measured by the American Society of Anesthesiology (ASA) score.
Results: The 89 procedures constituted 34 gastroscopies, 49 colonoscopies, and 6 flexible sigmoidoscopies. The cohort included 37 females (41.5%) and 52 males (58.4%). The mean age was 57 years old. Most cases had an ASA score of 2 (63%), followed by ASA 3 (21.3%) and 2 (14.6%).
Two colonoscopies were performed without any sedation due to social circumstances. All other procedures (87) were performed with a combination of fentanyl and midazolam, with a mean dose of 110 micrograms and 3 milligrams respectively per procedure. In 3 colonoscopies, inhaled nitrous oxide was used as an adjunct, facilitating completion of the procedure. No sedation related adverse events or complications were identified. Notably, one colonoscopy was unable to be completed due to patient discomfort, and was repeated under general anaesthetic. Furthermore, 15 cases were reported as technically difficult, with 6 cases attributed to non-sedation related technical factors such as body habitus. In 9 (10.1%) cases, however, patient discomfort was cited as contributing to the technical difficulty. The majority of these cases were colonoscopies (7; 7.9%), with 1 flexible sigmoidoscopy (1.1%) and 1 gastroscopy (1.1%).
Conclusion: In a unit with local expertise, light sedation is safe and effective for performing low-risk endoscopy procedures. In about 10% of cases, patient discomfort may contribute to technical difficulty, particularly in colonoscopies. However, adjuncts such as inhaled nitrous oxide can improve tolerability. Further studies including cost-analysis are required to establish the role of hybrid models of sedation in the Australian endoscopy setting.
581
Life-threatening upper gastrointestinal bleeding following percutaneous endoscopic gastrostomy tube removal under traction
Christopher James Shephard1, Xiaomin Ma1,2 and Rozemary Karamatic1
1Department of Gastroenterology and Hepatology, Townsville University Hospital, Townsville, Australia;2School of Medicine, University of Queensland, Brisbane, Australia
Introduction: Percutaneous endoscopic gastrostomy (PEG) tubes are commonly inserted for long-term enteral feeding. Gastrointestinal (GI) bleeding is reported in up to 2.67% of patients following tube insertion often due to disruption of small gastric vessels. Haemorrhage following tube removal is comparatively rare, with a recent retrospective analysis of 127 cases of traction removal recording zero bleeding events. Post-removal bleeding has been successfully managed with Foley catheter balloon tamponade or endoscopic over-the-scope clipping (OTSC) per previous reports. We present a case of life-threatening GI bleeding following traction PEG tube removal necessitating urgent endotherapy, followed by definitive surgical management – a mode of intervention not previously described.
Case report: A 73-year-old female undergoing rehabilitation following craniotomy and cranioplasty for subdural haemorrhage was transferred to the emergency department with large volume haematemesis and melaena five hours after PEG tube removal under traction. The tube (original with bumper, appropriate for traction removal) was inserted without complication four months prior for neurological dysphagia without intervening site issues. Background was relevant for monoclonal gammopathy of unknown significance, complex splenic cyst, α+-thalassemia trait, laparoscopic cholecystectomy and GI bleed following hyperplastic gastro-oesophageal junction polypectomy, but no previous gastric surgery. She was not on antiplatelet or anti-inflammatory drugs and had not received enoxaparin thromboprophylaxis for 48hours. Presenting haemoglobin was 75g/L from 97g/L three days prior, with platelets of 139x109/L, international normalised ratio of 1.1 and urea of 13.1mmol/L. She continued to have haemodynamically unstable GI bleeding despite aggressive resuscitation and blood transfusion. Rotational thromboelastometry (ROTEM) was conducted en route to emergent endoscopy under anaesthetic support. Upper endoscopy revealed copious fresh and clotted blood in the stomach with active arterial bleeding from the gastrostomy site (Figure 1A). Initial haemostasis was achieved with adrenaline injection around the site plus eight haemostatic clips (Figure 1B). The patient received ROTEM-guided cryoprecipitate and a total seven units of packed red cells on day one of admission, alongside a continuous pantoprazole infusion. Persistent GI bleeding the following day prompted computed tomography abdominal angiogram which demonstrated haematoma involving the PEG tract but no active contrast extravasation or free air, suggesting a sealed tract. Overnight, further haematemesis with haemodynamic instability and worsening anaemia dictated further transfusion and ROTEM-guided Prothrombinex. Due to concern for ongoing bleeding within the PEG tract likely non-amenable to endotherapy or tamponade via tube reinsertion (concern for false tract formation and additive trauma), surgical opinion was sought. Repeat endoscopy (with surgery on standby) revealed clotted gastric blood with haemostatic clips in situ, but no new/alternative bleeding focus. She proceeded to emergency laparotomy, with intra-operative findings of PEG tract haematoma extending under adjacent mesentery, and a limb of omentum interposed between the stomach and abdominal wall harbouring a bleeding vessel. Definitive haemostasis was achieved following excision of the PEG tract.
Conclusion: Traction PEG tube removal may be rarely complicated by severe, haemodynamically unstable GI bleeding requiring repeated blood transfusion and ROTEM-guided correction of coagulopathy. Arterial bleeding from within the PEG tract may be challenging to treat endoscopically, and even OTSC may not have effectively controlled an omental source. This case highlights the importance of considering timely surgical intervention as an option to treat refractory GI bleeding following PEG tube removal.
期刊介绍:
Journal of Gastroenterology and Hepatology is produced 12 times per year and publishes peer-reviewed original papers, reviews and editorials concerned with clinical practice and research in the fields of hepatology, gastroenterology and endoscopy. Papers cover the medical, radiological, pathological, biochemical, physiological and historical aspects of the subject areas. All submitted papers are reviewed by at least two referees expert in the field of the submitted paper.
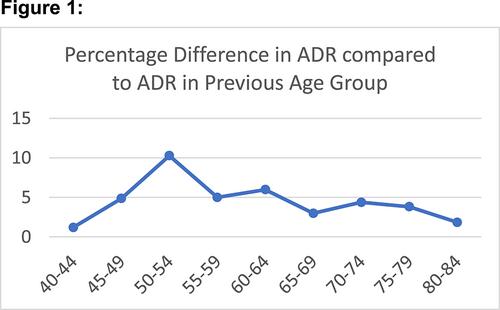


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
