Timing of percutaneous coronary intervention and risk of new-onset acute ischemic stroke in non-ST elevation myocardial infarction: A retrospective cohort study insight into the National Inpatient Sample Database (2016–2019)
Bo Shi, Xueping Ma, Congyan Ye, Rui Yan, Shizhe Fu, Kairu Wang, Mingzhi Cui, Ru Yan, Shaobin Jia, Guangzhi Cong
{"title":"Timing of percutaneous coronary intervention and risk of new-onset acute ischemic stroke in non-ST elevation myocardial infarction: A retrospective cohort study insight into the National Inpatient Sample Database (2016–2019)","authors":"Bo Shi, Xueping Ma, Congyan Ye, Rui Yan, Shizhe Fu, Kairu Wang, Mingzhi Cui, Ru Yan, Shaobin Jia, Guangzhi Cong","doi":"10.1002/hsr2.70029","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background and Aims</h3>\n \n <p>For patients with high-risk non-ST elevation myocardial infarction (NSTEMI), current guidelines recommend an early invasive strategy within 24 h. New-onset acute ischemic stroke (NAIS) is a rare but fatal complication of percutaneous coronary intervention (PCI). However, the effect of the timing of PCI and the risk of NAIS in NSTEMI is poorly defined.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Patients with NSTEMI who underwent PCI were queried from the National Inpatient Sample Database (2016–2019) and stratified into three groups: early (<24 h), medium (24–72 h), and late (>72 h) PCI. Multivariate logistic regression models were used to determine the association between timing of PCI and NAIS.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Among 633,115 weighted hospitalizations, patients in the late PCI group had a higher incidence of NAIS (1.3%) than those in the early (0.67%) and medium (0.71%) PCI groups. Patients undergoing late PCI were older, more likely to be female, and had a greater incidence of comorbidities (e.g., diabetes mellitus, chronic pulmonary and renal illness, and atrial fibrillation) than those undergoing early or medium PCI. After adjustment, only late PCI was significantly associated with a 54% increased NAIS risk (adjusted odds ratio: 1.54 [95% confidence interval: 1.29–1.84]). Additionally, there was heterogeneity in the magnitude of risk by age and sex. Younger people (<65 years) (<i>p</i> for interaction <0.001) and men (interaction-value <i>p</i> = 0.040) were more likely to encounter NAIS.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Late PCI was associated with a higher risk of NAIS than early PCI, particularly among men and those aged <65 years.</p>\n </section>\n </div>","PeriodicalId":36518,"journal":{"name":"Health Science Reports","volume":"7 9","pages":""},"PeriodicalIF":2.1000,"publicationDate":"2024-09-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/hsr2.70029","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health Science Reports","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/hsr2.70029","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background and Aims
For patients with high-risk non-ST elevation myocardial infarction (NSTEMI), current guidelines recommend an early invasive strategy within 24 h. New-onset acute ischemic stroke (NAIS) is a rare but fatal complication of percutaneous coronary intervention (PCI). However, the effect of the timing of PCI and the risk of NAIS in NSTEMI is poorly defined.
Methods
Patients with NSTEMI who underwent PCI were queried from the National Inpatient Sample Database (2016–2019) and stratified into three groups: early (<24 h), medium (24–72 h), and late (>72 h) PCI. Multivariate logistic regression models were used to determine the association between timing of PCI and NAIS.
Results
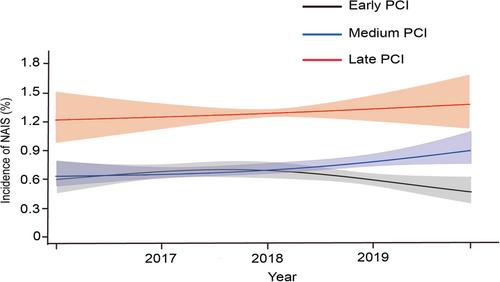
Among 633,115 weighted hospitalizations, patients in the late PCI group had a higher incidence of NAIS (1.3%) than those in the early (0.67%) and medium (0.71%) PCI groups. Patients undergoing late PCI were older, more likely to be female, and had a greater incidence of comorbidities (e.g., diabetes mellitus, chronic pulmonary and renal illness, and atrial fibrillation) than those undergoing early or medium PCI. After adjustment, only late PCI was significantly associated with a 54% increased NAIS risk (adjusted odds ratio: 1.54 [95% confidence interval: 1.29–1.84]). Additionally, there was heterogeneity in the magnitude of risk by age and sex. Younger people (<65 years) (p for interaction <0.001) and men (interaction-value p = 0.040) were more likely to encounter NAIS.
Conclusion
Late PCI was associated with a higher risk of NAIS than early PCI, particularly among men and those aged <65 years.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
