{"title":"A Predictive Nomogram of In-Hospital Mortality After 48 h for Atrial Fibrillation Patients in the Coronary Care Unit","authors":"Wenhui Wang, Linlin Liu, Lu Jin, Bo Hu","doi":"10.1002/clc.70017","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Patients with atrial fibrillation (AF) suffer a higher risk of death, and it is necessary to develop prediction tools for mortality risk in critically ill patients with AF. This study aimed to develop a novel predictive nomogram of in-hospital mortality after 48 h in the coronary care unit (CCU) for patients with AF.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>We collected information on CCU patients with AF from the “Medical Information Mart for Intensive Care-III” database and developed a nomogram model for predicting the all-cause mortality risk after 48 h in the hospital. Key variables were selected by univariate logistic and least absolute shrinkage and selection operator regression. The independent predictors with <i>p</i> < 0.05 were screened out by multivariate logistic regression. A predictive nomogram was constructed using these independent predictors, and the model calibration and discrimination were evaluated.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>This study finally enrolled 1248 CCU patients with AF, and the in-hospital mortality was 17% (209/1248). The predictive nomogram was constructed by 13 selected independent predictors, including age, smoking status, acute kidney injury, chronic obstructive pulmonary disease, ventricular arrhythmia, shock, urea, red cell distribution width, leucocytosis, continuous renal replacement therapy, continuous positive airway pressure, anticoagulation, and heart rate. The area under the curve of the nomogram was 0.803 (95% confidence interval 0.771–0.835). The nomogram was verified to have good accuracy and calibration.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>This study developed a novel nomogram containing age, acute kidney injury, and heart rate that can be a good predictor of potential in-hospital mortality after 48 h in CCU patients with AF.</p>\n </section>\n </div>","PeriodicalId":10201,"journal":{"name":"Clinical Cardiology","volume":"47 9","pages":""},"PeriodicalIF":2.3000,"publicationDate":"2024-09-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/clc.70017","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Cardiology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/clc.70017","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Patients with atrial fibrillation (AF) suffer a higher risk of death, and it is necessary to develop prediction tools for mortality risk in critically ill patients with AF. This study aimed to develop a novel predictive nomogram of in-hospital mortality after 48 h in the coronary care unit (CCU) for patients with AF.
Methods
We collected information on CCU patients with AF from the “Medical Information Mart for Intensive Care-III” database and developed a nomogram model for predicting the all-cause mortality risk after 48 h in the hospital. Key variables were selected by univariate logistic and least absolute shrinkage and selection operator regression. The independent predictors with p < 0.05 were screened out by multivariate logistic regression. A predictive nomogram was constructed using these independent predictors, and the model calibration and discrimination were evaluated.
Results
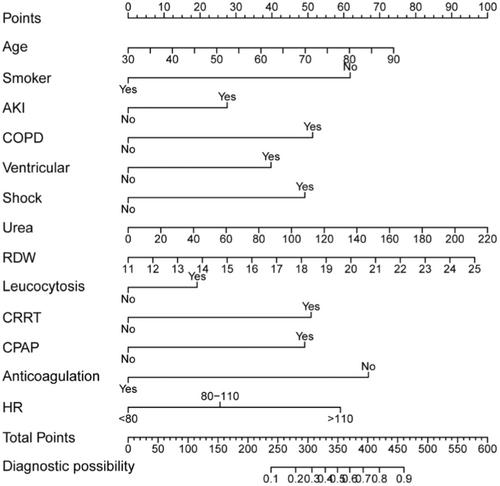
This study finally enrolled 1248 CCU patients with AF, and the in-hospital mortality was 17% (209/1248). The predictive nomogram was constructed by 13 selected independent predictors, including age, smoking status, acute kidney injury, chronic obstructive pulmonary disease, ventricular arrhythmia, shock, urea, red cell distribution width, leucocytosis, continuous renal replacement therapy, continuous positive airway pressure, anticoagulation, and heart rate. The area under the curve of the nomogram was 0.803 (95% confidence interval 0.771–0.835). The nomogram was verified to have good accuracy and calibration.
Conclusions
This study developed a novel nomogram containing age, acute kidney injury, and heart rate that can be a good predictor of potential in-hospital mortality after 48 h in CCU patients with AF.
期刊介绍:
Clinical Cardiology provides a fully Gold Open Access forum for the publication of original clinical research, as well as brief reviews of diagnostic and therapeutic issues in cardiovascular medicine and cardiovascular surgery.
The journal includes Clinical Investigations, Reviews, free standing editorials and commentaries, and bonus online-only content.
The journal also publishes supplements, Expert Panel Discussions, sponsored clinical Reviews, Trial Designs, and Quality and Outcomes.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
