Julia Lueg, Daniel Schulze, Robert Stöhr, David M. Leistner
{"title":"Distal versus proximal radial access in coronary angiography: a meta-analysis","authors":"Julia Lueg, Daniel Schulze, Robert Stöhr, David M. Leistner","doi":"10.1007/s00392-024-02505-3","DOIUrl":null,"url":null,"abstract":"<h3 data-test=\"abstract-sub-heading\">Background</h3><p>Distal radial access (DRA) represents a promising alternative to conventional proximal radial access (PRA) for coronary angiography. Substantial advantages regarding safety and efficacy have been suggested for DRA, but the ideal access route remains controversial.</p><h3 data-test=\"abstract-sub-heading\">Aims</h3><p>The aim of this study was to compare safety, efficacy and feasibility of DRA to PRA.</p><h3 data-test=\"abstract-sub-heading\">Methods</h3><p>National Library of Medicine PubMed, Web of Science, clinicaltrials.gov and Cochrane Library were systematically searched for randomized controlled trials and registry studies comparing DRA and PRA that were published between January 1, 2017 and April, 2024. Primary endpoint was the rate of radial artery occlusion (RAO). Secondary endpoints were access failure, access time, procedure time, arterial spasm, hematoma, and hemostasis time. Data extraction was performed by two independent investigators. Relative risks were aggregated using a random effects model. We applied meta-analytic regression to assess study characteristic variables as possible moderators of the study effects.</p><h3 data-test=\"abstract-sub-heading\">Results</h3><p>44 studies with a total of 21,081 patients were included. We found a significantly lower rate of RAO after DRA (DRA 1.28%, PRA 4.76%, <i>p</i> < .001) with a 2.92 times lower risk compared to the proximal approach (Log Risk Ratio = −1.07, <i>p</i> < .001). Conversely, the risk for access failure was 2.42 times higher for DRA compared to PRA (Log Risk Ratio = 0.88, <i>p</i> < .001).</p><h3 data-test=\"abstract-sub-heading\">Conclusion</h3><p>In this largest meta-analysis to date, we were able to show that rates of RAO are reduced with DRA compared to conventional PRA. This suggests DRA is a safe alternative to PRA.</p><h3 data-test=\"abstract-sub-heading\">Graphical abstract</h3>\n","PeriodicalId":10474,"journal":{"name":"Clinical Research in Cardiology","volume":"213 1","pages":""},"PeriodicalIF":3.7000,"publicationDate":"2024-09-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Research in Cardiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00392-024-02505-3","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Distal radial access (DRA) represents a promising alternative to conventional proximal radial access (PRA) for coronary angiography. Substantial advantages regarding safety and efficacy have been suggested for DRA, but the ideal access route remains controversial.
Aims
The aim of this study was to compare safety, efficacy and feasibility of DRA to PRA.
Methods
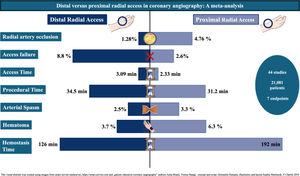
National Library of Medicine PubMed, Web of Science, clinicaltrials.gov and Cochrane Library were systematically searched for randomized controlled trials and registry studies comparing DRA and PRA that were published between January 1, 2017 and April, 2024. Primary endpoint was the rate of radial artery occlusion (RAO). Secondary endpoints were access failure, access time, procedure time, arterial spasm, hematoma, and hemostasis time. Data extraction was performed by two independent investigators. Relative risks were aggregated using a random effects model. We applied meta-analytic regression to assess study characteristic variables as possible moderators of the study effects.
Results
44 studies with a total of 21,081 patients were included. We found a significantly lower rate of RAO after DRA (DRA 1.28%, PRA 4.76%, p < .001) with a 2.92 times lower risk compared to the proximal approach (Log Risk Ratio = −1.07, p < .001). Conversely, the risk for access failure was 2.42 times higher for DRA compared to PRA (Log Risk Ratio = 0.88, p < .001).
Conclusion
In this largest meta-analysis to date, we were able to show that rates of RAO are reduced with DRA compared to conventional PRA. This suggests DRA is a safe alternative to PRA.
期刊介绍:
Clinical Research in Cardiology is an international journal for clinical cardiovascular research. It provides a forum for original and review articles as well as critical perspective articles. Articles are only accepted if they meet stringent scientific standards and have undergone peer review. The journal regularly receives articles from the field of clinical cardiology, angiology, as well as heart and vascular surgery.
As the official journal of the German Cardiac Society, it gives a current and competent survey on the diagnosis and therapy of heart and vascular diseases.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
