Ingo Steinbrück, Viktor Rempel, Armin Kuellmer, Valentin Miedtke, Siegbert Faiss, Thomas von Hahn, Jürgen Pohl, Johannes Grothaus, Matthias Friesicke, Arthur Schmidt, Hans-Peter Allgaier
{"title":"Flexible endoscopic treatment of Zenker’s diverticulum—a retrospective, observational multicenter study","authors":"Ingo Steinbrück, Viktor Rempel, Armin Kuellmer, Valentin Miedtke, Siegbert Faiss, Thomas von Hahn, Jürgen Pohl, Johannes Grothaus, Matthias Friesicke, Arthur Schmidt, Hans-Peter Allgaier","doi":"10.1007/s00464-024-11234-7","DOIUrl":null,"url":null,"abstract":"<h3 data-test=\"abstract-sub-heading\">Background</h3><p>The European Society of Gastroenterology and Endoscopy recommends a primarily flexible endoscopic approach for the treatment of Zenker’s diverticulum. Due to the rarity of the disorder, evidence for its effectiveness and safety comes mainly from small, retrospective, single-center studies.</p><h3 data-test=\"abstract-sub-heading\">Methods</h3><p>In this retrospective, observational, multicenter cohort study, data from six German tertiary referral centers were analyzed. The primary outcome parameters were technical and clinical success; among the secondary outcomes, the rates of adverse events (AE) and re-admission with symptomatic recurrence and mortality were the most relevant.</p><h3 data-test=\"abstract-sub-heading\">Results</h3><p>Between 2003 and 2024, 384 treatments were performed in 327 patients (61.8% male, mean age 74.70 (± 10.60)). Incision methods/techniques were 250 needle knives, 44 ESD knives, 64 stag beetle knives, 24 staplers, one APC-probe, and one Z-POEM. The Zenker’s diverticulum overtube was used in 65.1%, prophylactic clipping in 30.2%, and antibiotic therapy in 25.3% of treatments. The rates of technical and clinical success were 99.2% and 97.4%, and the rates of AE and re-admission with symptomatic recurrence were 11.2% and 16.7%, respectively. Mortality was 0.3%. Comparative subgroup analyses of 312 diverticula without prior treatment versus 72 symptomatic recurrences and incision methods/techniques showed no significant differences in outcome parameters. The use of additional devices and prophylactic measures (clipping, antibiotic therapy) were not independent predictors of technical/clinical success or AE in uni-/multivariable regression analysis.</p><h3 data-test=\"abstract-sub-heading\">Conclusions</h3><p>Flexible endoscopic Zenker’s diverticulotomy is a safe and effective minimally invasive treatment. Recurrences can be treated by flexible endoscopy with comparable results. None of the cutting methods, ancillary devices, or prophylactic measures showed superiority in effectiveness or safety.</p><h3 data-test=\"abstract-sub-heading\">Graphical abstract</h3>\n","PeriodicalId":501625,"journal":{"name":"Surgical Endoscopy","volume":"1 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2024-09-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical Endoscopy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s00464-024-11234-7","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background
The European Society of Gastroenterology and Endoscopy recommends a primarily flexible endoscopic approach for the treatment of Zenker’s diverticulum. Due to the rarity of the disorder, evidence for its effectiveness and safety comes mainly from small, retrospective, single-center studies.
Methods
In this retrospective, observational, multicenter cohort study, data from six German tertiary referral centers were analyzed. The primary outcome parameters were technical and clinical success; among the secondary outcomes, the rates of adverse events (AE) and re-admission with symptomatic recurrence and mortality were the most relevant.
Results
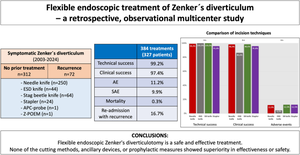
Between 2003 and 2024, 384 treatments were performed in 327 patients (61.8% male, mean age 74.70 (± 10.60)). Incision methods/techniques were 250 needle knives, 44 ESD knives, 64 stag beetle knives, 24 staplers, one APC-probe, and one Z-POEM. The Zenker’s diverticulum overtube was used in 65.1%, prophylactic clipping in 30.2%, and antibiotic therapy in 25.3% of treatments. The rates of technical and clinical success were 99.2% and 97.4%, and the rates of AE and re-admission with symptomatic recurrence were 11.2% and 16.7%, respectively. Mortality was 0.3%. Comparative subgroup analyses of 312 diverticula without prior treatment versus 72 symptomatic recurrences and incision methods/techniques showed no significant differences in outcome parameters. The use of additional devices and prophylactic measures (clipping, antibiotic therapy) were not independent predictors of technical/clinical success or AE in uni-/multivariable regression analysis.
Conclusions
Flexible endoscopic Zenker’s diverticulotomy is a safe and effective minimally invasive treatment. Recurrences can be treated by flexible endoscopy with comparable results. None of the cutting methods, ancillary devices, or prophylactic measures showed superiority in effectiveness or safety.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
