{"title":"Clinical, oncological, and prognostic differences of patients with subsequent skeletal-related events in bone metastases.","authors":"Hsiang-Chieh Hsieh, Hung-Kuan Yen, Wen-Tung Hsieh, Ching-Wei Lin, Yu-Ting Pan, Fu-Shan Jaw, Stein J Janssen, Wei-Hsin Lin, Ming-Hsiao Hu, Olivier Groot","doi":"10.1302/2046-3758.139.BJR-2023-0372.R1","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Advances in treatment have extended the life expectancy of patients with metastatic bone disease (MBD). Patients could experience more skeletal-related events (SREs) as a result of this progress. Those who have already experienced a SRE could encounter another local management for a subsequent SRE, which is not part of the treatment for the initial SRE. However, there is a noted gap in research on the rate and characteristics of subsequent SREs requiring further localized treatment, obligating clinicians to extrapolate from experiences with initial SREs when confronting subsequent ones. This study aimed to investigate the proportion of MBD patients developing subsequent SREs requiring local treatment, examine if there are prognostic differences at the initial treatment between those with single versus subsequent SREs, and determine if clinical, oncological, and prognostic features differ between initial and subsequent SRE treatments.</p><p><strong>Methods: </strong>This retrospective study included 3,814 adult patients who received local treatment - surgery and/or radiotherapy - for bone metastasis between 1 January 2010 and 31 December 2019. All included patients had at least one SRE requiring local treatment. A subsequent SRE was defined as a second SRE requiring local treatment. Clinical, oncological, and prognostic features were compared between single SREs and subsequent SREs using Mann-Whitney U test, Fisher's exact test, and Kaplan-Meier curve.</p><p><strong>Results: </strong>Of the 3,814 patients with SREs, 3,159 (83%) patients had a single SRE and 655 (17%) patients developed a subsequent SRE. Patients who developed subsequent SREs generally had characteristics that favoured longer survival, such as higher BMI, higher albumin levels, fewer comorbidities, or lower neutrophil count. Once the patient got to the point of subsequent SRE, their clinical and oncological characteristics and one-year survival (28%) were not as good as those with only a single SRE (35%; p < 0.001), indicating that clinicians' experiences when treating the initial SRE are not similar when treating a subsequent SRE.</p><p><strong>Conclusion: </strong>This study found that 17% of patients required treatments for a second, subsequent SRE, and the current clinical guideline did not provide a specific approach to this clinical condition. We observed that referencing the initial treatment, patients in the subsequent SRE group had longer six-week, 90-day, and one-year median survival than patients in the single SRE group. Once patients develop a subsequent SRE, they have a worse one-year survival rate than those who receive treatment for a single SRE. Future research should identify prognostic factors and assess the applicability of existing survival prediction models for better management of subsequent SREs.</p>","PeriodicalId":9074,"journal":{"name":"Bone & Joint Research","volume":"13 9","pages":"497-506"},"PeriodicalIF":5.1000,"publicationDate":"2024-09-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11402515/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Bone & Joint Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1302/2046-3758.139.BJR-2023-0372.R1","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CELL & TISSUE ENGINEERING","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: Advances in treatment have extended the life expectancy of patients with metastatic bone disease (MBD). Patients could experience more skeletal-related events (SREs) as a result of this progress. Those who have already experienced a SRE could encounter another local management for a subsequent SRE, which is not part of the treatment for the initial SRE. However, there is a noted gap in research on the rate and characteristics of subsequent SREs requiring further localized treatment, obligating clinicians to extrapolate from experiences with initial SREs when confronting subsequent ones. This study aimed to investigate the proportion of MBD patients developing subsequent SREs requiring local treatment, examine if there are prognostic differences at the initial treatment between those with single versus subsequent SREs, and determine if clinical, oncological, and prognostic features differ between initial and subsequent SRE treatments.
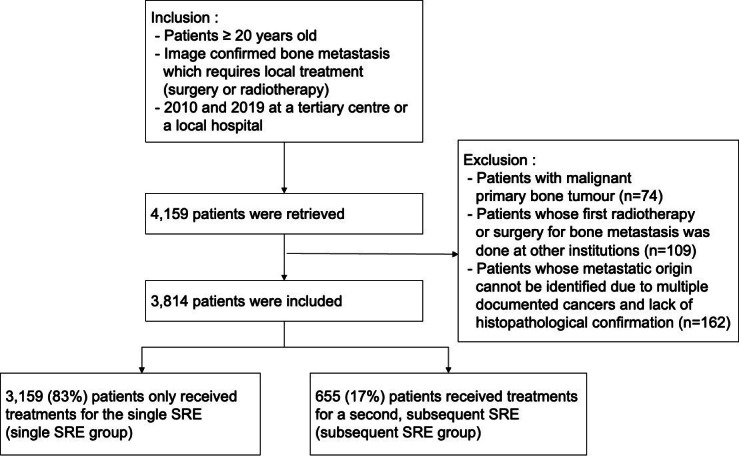
Methods: This retrospective study included 3,814 adult patients who received local treatment - surgery and/or radiotherapy - for bone metastasis between 1 January 2010 and 31 December 2019. All included patients had at least one SRE requiring local treatment. A subsequent SRE was defined as a second SRE requiring local treatment. Clinical, oncological, and prognostic features were compared between single SREs and subsequent SREs using Mann-Whitney U test, Fisher's exact test, and Kaplan-Meier curve.
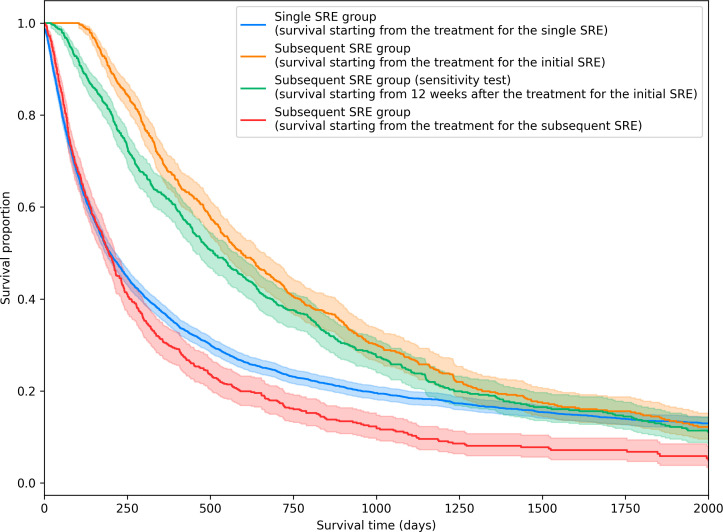
Results: Of the 3,814 patients with SREs, 3,159 (83%) patients had a single SRE and 655 (17%) patients developed a subsequent SRE. Patients who developed subsequent SREs generally had characteristics that favoured longer survival, such as higher BMI, higher albumin levels, fewer comorbidities, or lower neutrophil count. Once the patient got to the point of subsequent SRE, their clinical and oncological characteristics and one-year survival (28%) were not as good as those with only a single SRE (35%; p < 0.001), indicating that clinicians' experiences when treating the initial SRE are not similar when treating a subsequent SRE.
Conclusion: This study found that 17% of patients required treatments for a second, subsequent SRE, and the current clinical guideline did not provide a specific approach to this clinical condition. We observed that referencing the initial treatment, patients in the subsequent SRE group had longer six-week, 90-day, and one-year median survival than patients in the single SRE group. Once patients develop a subsequent SRE, they have a worse one-year survival rate than those who receive treatment for a single SRE. Future research should identify prognostic factors and assess the applicability of existing survival prediction models for better management of subsequent SREs.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
