Pedro Luiz Serrano Uson Junior, Ana Luiza Spina Nagy, Igor Wanderley Reis Dias, Marcelo Bruno de Rezende, Roberto Pestana, Diogo Bugano, Francisco Tustumi, Guilherme Naccache Namur, Jaime Arthur Pirola Kruger, Alberto Goldenberg, Sergio Eduardo Alonso Araujo, Nam Jin Kim, Sidney Klajner, Mitesh Borad, Fernando Moura
{"title":"Concomitant or antecedent intraductal papillary mucinous neoplasm is not a prognostic factor in resected pancreatic cancer.","authors":"Pedro Luiz Serrano Uson Junior, Ana Luiza Spina Nagy, Igor Wanderley Reis Dias, Marcelo Bruno de Rezende, Roberto Pestana, Diogo Bugano, Francisco Tustumi, Guilherme Naccache Namur, Jaime Arthur Pirola Kruger, Alberto Goldenberg, Sergio Eduardo Alonso Araujo, Nam Jin Kim, Sidney Klajner, Mitesh Borad, Fernando Moura","doi":"10.21037/jgo-24-157","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Intraductal papillary mucinous neoplasm (IPMN)-associated pancreatic cancer is becoming a common subtype of pancreatic cancer found in resected specimens. The prognostic of this subtype is still under evaluation. The study aims to evaluate the prognosis of IPMN-associated pancreatic adenocarcinoma compared to the conventional pancreatic adenocarcinoma.</p><p><strong>Methods: </strong>In this study, patients with resected pancreatic neoplasms and IPMN treated at Hospital Israelita Albert Einstein, from January 2016 to December 2020, were analyzed. Overall survival (OS) was estimated using the Kaplan-Meier method, and correlations between the variables of interest and the disease specific OS was assessed by multivariate analysis.</p><p><strong>Results: </strong>Of 187 patients undergoing resection for pancreatic adenocarcinoma or IPMN, 125 (67%) had pancreatic adenocarcinoma, 33 (18%) had IPMN-associated pancreatic adenocarcinoma, and 29 (16%) had IPMN. Resected IPMN was associated with long-term OS for most of the patients. Similar OS was identified in this study in upfront resected pancreatic cancer associated or not with IPMN. No statistical differences in median OS were identified between resected pancreatic adenocarcinoma and IPMN-associated pancreatic adenocarcinoma (48 <i>vs.</i> 44 months, P=0.44). Size of the tumor [hazard ratio (HR), 1.33], resected stage III (HR, 1.31), perineural invasion (HR, 1.58), lymphovascular invasion (HR, 1.44), positive lymph nodes (HR, 1.34), and neoadjuvant treatment (HR, 1.70) were associated with worse outcomes.</p><p><strong>Conclusions: </strong>Our findings confirm that resected pancreatic cancer has a poor prognosis and IPMN-associated pancreatic adenocarcinoma has the same prognosis as a conventional pancreatic adenocarcinoma. More than half of the cases of IPMN-associated adenocarcinoma already had positive lymph nodes. The impact of neoadjuvant treatment in this group of patients should be investigated in larger cohorts.</p>","PeriodicalId":15841,"journal":{"name":"Journal of gastrointestinal oncology","volume":"15 4","pages":"1820-1826"},"PeriodicalIF":2.0000,"publicationDate":"2024-08-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11399881/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of gastrointestinal oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/jgo-24-157","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/29 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Intraductal papillary mucinous neoplasm (IPMN)-associated pancreatic cancer is becoming a common subtype of pancreatic cancer found in resected specimens. The prognostic of this subtype is still under evaluation. The study aims to evaluate the prognosis of IPMN-associated pancreatic adenocarcinoma compared to the conventional pancreatic adenocarcinoma.
Methods: In this study, patients with resected pancreatic neoplasms and IPMN treated at Hospital Israelita Albert Einstein, from January 2016 to December 2020, were analyzed. Overall survival (OS) was estimated using the Kaplan-Meier method, and correlations between the variables of interest and the disease specific OS was assessed by multivariate analysis.
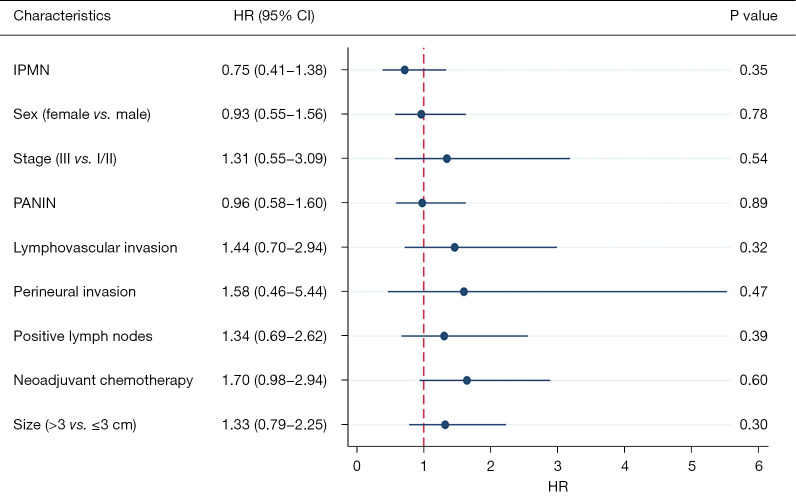
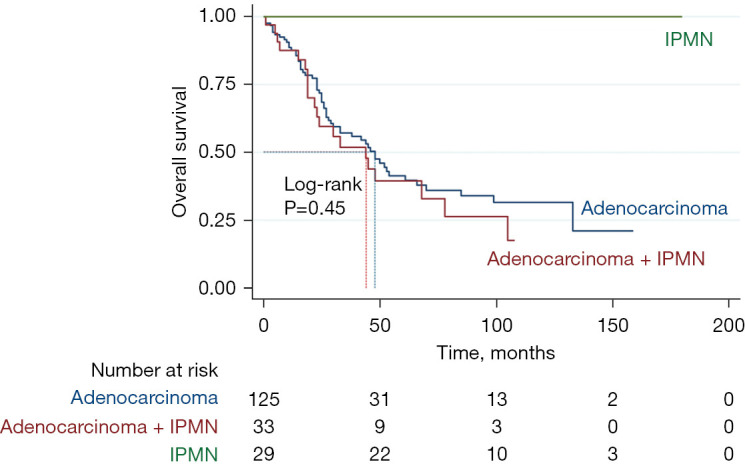
Results: Of 187 patients undergoing resection for pancreatic adenocarcinoma or IPMN, 125 (67%) had pancreatic adenocarcinoma, 33 (18%) had IPMN-associated pancreatic adenocarcinoma, and 29 (16%) had IPMN. Resected IPMN was associated with long-term OS for most of the patients. Similar OS was identified in this study in upfront resected pancreatic cancer associated or not with IPMN. No statistical differences in median OS were identified between resected pancreatic adenocarcinoma and IPMN-associated pancreatic adenocarcinoma (48 vs. 44 months, P=0.44). Size of the tumor [hazard ratio (HR), 1.33], resected stage III (HR, 1.31), perineural invasion (HR, 1.58), lymphovascular invasion (HR, 1.44), positive lymph nodes (HR, 1.34), and neoadjuvant treatment (HR, 1.70) were associated with worse outcomes.
Conclusions: Our findings confirm that resected pancreatic cancer has a poor prognosis and IPMN-associated pancreatic adenocarcinoma has the same prognosis as a conventional pancreatic adenocarcinoma. More than half of the cases of IPMN-associated adenocarcinoma already had positive lymph nodes. The impact of neoadjuvant treatment in this group of patients should be investigated in larger cohorts.
期刊介绍:
ournal of Gastrointestinal Oncology (Print ISSN 2078-6891; Online ISSN 2219-679X; J Gastrointest Oncol; JGO), the official journal of Society for Gastrointestinal Oncology (SGO), is an open-access, international peer-reviewed journal. It is published quarterly (Sep. 2010- Dec. 2013), bimonthly (Feb. 2014 -) and openly distributed worldwide.
JGO publishes manuscripts that focus on updated and practical information about diagnosis, prevention and clinical investigations of gastrointestinal cancer treatment. Specific areas of interest include, but not limited to, multimodality therapy, markers, imaging and tumor biology.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
