Matching-Adjusted Indirect Comparison of the Efficacy and Safety of Erdafitinib vs Enfortumab Vedotin in Patients with Locally Advanced Metastatic Urothelial Carcinoma.
Suzy Van Sanden, Ayman Youssef, Simona Baculea, Keith Stubbs, Spyros Triantos, Zijiao Yuan, Caitlin Daly
{"title":"Matching-Adjusted Indirect Comparison of the Efficacy and Safety of Erdafitinib vs Enfortumab Vedotin in Patients with Locally Advanced Metastatic Urothelial Carcinoma.","authors":"Suzy Van Sanden, Ayman Youssef, Simona Baculea, Keith Stubbs, Spyros Triantos, Zijiao Yuan, Caitlin Daly","doi":"10.36469/001c.120954","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> For patients with locally advanced or metastatic urothelial carcinoma (la/mUC), prognosis is poor and effective treatment options are limited. Erdafitinib is an oral fibroblast growth factor receptor (FGFR) kinase inhibitor approved by the FDA for the treatment of adults with la/mUC harboring FGFR alterations whose disease progressed following at least 1 prior line of therapy, including a PD-1 or PD-L(1) inhibitor, based on the phase 3, randomized THOR trial (NCT03390504, Cohort 1). <b>Objective:</b> To compare the efficacy and safety of erdafitinib vs enfortumab vedotin-ejfv (EV) in the absence of head-to-head comparison via an anchored matching-adjusted indirect comparison (MAIC). <b>Methods:</b> An anchored MAIC was conducted according to the National Institute for Health and Care Excellence Decision Support Unit guidance, with physician's choice of chemotherapy (docetaxel/paclitaxel and vinflunine) as the common comparator. Individual patient data from THOR were adjusted to match published key eligibility criteria and average baseline characteristics of EV-301, such as Bellmunt risk score, liver or visceral metastases, primary site, among others. Erdafitinib was then indirectly compared with EV using the relative treatment effects for the reweighted THOR population and those published for EV-301. <b>Results:</b> After matching, the effective sample size for THOR was 126 patients. The MAIC-recalculated hazard ratio (95% credible interval) for erdafitinib vs EV was 0.92 (0.54, 1.57) for overall survival and 0.93 (0.55, 1.56) for progression-free survival, yielding Bayesian probabilities of erdafitinib being better than EV of 62.1% and 60.5%, respectively. For response outcomes, the MAIC-recalculated risk ratio was 1.49 (0.56, 3.90) for confirmed objective response rate and 2.89 (0.27, 30.33) for confirmed complete response with probabilities of 72.6% and 81.3% for erdafitinib being better than EV, respectively. For safety, MAIC-yielded risk ratios of 1.09 (0.99, 1.21) for any treatment-related adverse events, 0.86 (0.57, 1.28) for grade 3+ TRAEs, and 1.02 (0.98, 1.06) for any treatment-emergent adverse events. <b>Conclusion:</b> The MAIC indicates comparable efficacy of erdafitinib vs EV for overall survival and progression-free survival, with erdafitinib showing a higher probability of achieving deep responses. While erdafitinib is associated with slightly more adverse events compared with EV, these events seem to be less severe.</p>","PeriodicalId":16012,"journal":{"name":"Journal of Health Economics and Outcomes Research","volume":"11 2","pages":"49-57"},"PeriodicalIF":2.3000,"publicationDate":"2024-08-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11392482/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Health Economics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36469/001c.120954","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ECONOMICS","Score":null,"Total":0}
引用次数: 0
Abstract
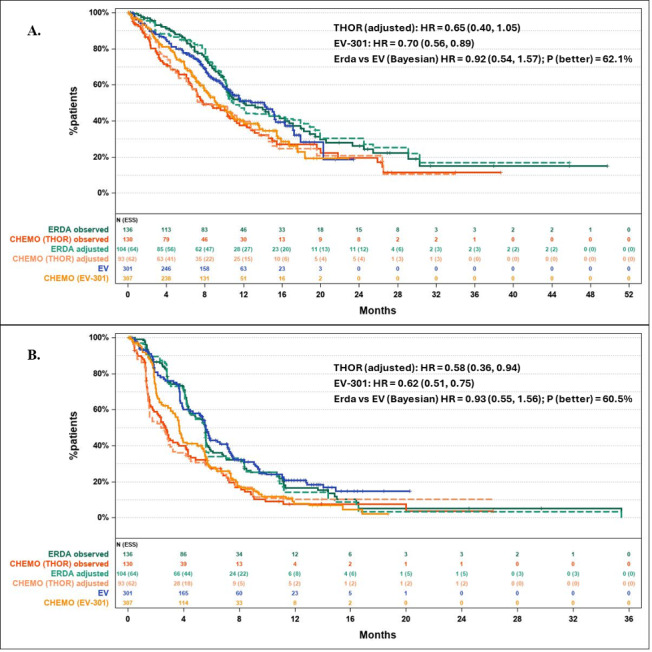
Background: For patients with locally advanced or metastatic urothelial carcinoma (la/mUC), prognosis is poor and effective treatment options are limited. Erdafitinib is an oral fibroblast growth factor receptor (FGFR) kinase inhibitor approved by the FDA for the treatment of adults with la/mUC harboring FGFR alterations whose disease progressed following at least 1 prior line of therapy, including a PD-1 or PD-L(1) inhibitor, based on the phase 3, randomized THOR trial (NCT03390504, Cohort 1). Objective: To compare the efficacy and safety of erdafitinib vs enfortumab vedotin-ejfv (EV) in the absence of head-to-head comparison via an anchored matching-adjusted indirect comparison (MAIC). Methods: An anchored MAIC was conducted according to the National Institute for Health and Care Excellence Decision Support Unit guidance, with physician's choice of chemotherapy (docetaxel/paclitaxel and vinflunine) as the common comparator. Individual patient data from THOR were adjusted to match published key eligibility criteria and average baseline characteristics of EV-301, such as Bellmunt risk score, liver or visceral metastases, primary site, among others. Erdafitinib was then indirectly compared with EV using the relative treatment effects for the reweighted THOR population and those published for EV-301. Results: After matching, the effective sample size for THOR was 126 patients. The MAIC-recalculated hazard ratio (95% credible interval) for erdafitinib vs EV was 0.92 (0.54, 1.57) for overall survival and 0.93 (0.55, 1.56) for progression-free survival, yielding Bayesian probabilities of erdafitinib being better than EV of 62.1% and 60.5%, respectively. For response outcomes, the MAIC-recalculated risk ratio was 1.49 (0.56, 3.90) for confirmed objective response rate and 2.89 (0.27, 30.33) for confirmed complete response with probabilities of 72.6% and 81.3% for erdafitinib being better than EV, respectively. For safety, MAIC-yielded risk ratios of 1.09 (0.99, 1.21) for any treatment-related adverse events, 0.86 (0.57, 1.28) for grade 3+ TRAEs, and 1.02 (0.98, 1.06) for any treatment-emergent adverse events. Conclusion: The MAIC indicates comparable efficacy of erdafitinib vs EV for overall survival and progression-free survival, with erdafitinib showing a higher probability of achieving deep responses. While erdafitinib is associated with slightly more adverse events compared with EV, these events seem to be less severe.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
