Tobenna Ibeabuchi, Eric Li, Claire Cywes, Therese Bittermann, Nadim Mahmud, Peter L Abt
{"title":"The Association Between the Origin of the Donation After Circulatory Death Liver Recovery Team and Graft Survival: A National Study.","authors":"Tobenna Ibeabuchi, Eric Li, Claire Cywes, Therese Bittermann, Nadim Mahmud, Peter L Abt","doi":"10.1097/TXD.0000000000001699","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Transplant centers have traditionally relied upon procurement teams from their own programs (transplant program procurement team [TPT]) to recover donation after circulatory death (DCD) livers and rarely use surgical procurement teams not affiliated with the recipient center (nontransplant program procurement team [NTPT]). However, in the era of wider geographic organ sharing, greater reliance on NTPTs is often necessary.</p><p><strong>Methods: </strong>We used national data to study the association between the origin of the donor procurement team (NTPT versus TPT) and the risk of DCD liver allograft failure.</p><p><strong>Results: </strong>Five hundred NTPT and 2257 TPT DCD transplants were identified: 1-y graft survival was 88.9 and 88.6%, respectively (<i>P</i> = 0.962). In a multivariable model, the origin of the procurement team was not associated with graft failure NTPT versus TPT (hazard ratio, 0.92; 95% confidence interval, 0.71-1.22; <i>P</i> = 0.57) but rather with known risks for DCD graft loss including donor age, degree of recipient illness, cold ischemic time, and retransplantation. The overall incidence of retransplantation and ischemic cholangiopathy as an indication for retransplantation were similar between NTPT and TPT.</p><p><strong>Conclusions: </strong>This data suggests that transplant centers may be able to safely use DCD livers recovered by local surgical teams.</p>","PeriodicalId":23225,"journal":{"name":"Transplantation Direct","volume":"10 10","pages":"e1699"},"PeriodicalIF":1.9000,"publicationDate":"2024-09-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11410324/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplantation Direct","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/TXD.0000000000001699","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"TRANSPLANTATION","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Transplant centers have traditionally relied upon procurement teams from their own programs (transplant program procurement team [TPT]) to recover donation after circulatory death (DCD) livers and rarely use surgical procurement teams not affiliated with the recipient center (nontransplant program procurement team [NTPT]). However, in the era of wider geographic organ sharing, greater reliance on NTPTs is often necessary.
Methods: We used national data to study the association between the origin of the donor procurement team (NTPT versus TPT) and the risk of DCD liver allograft failure.
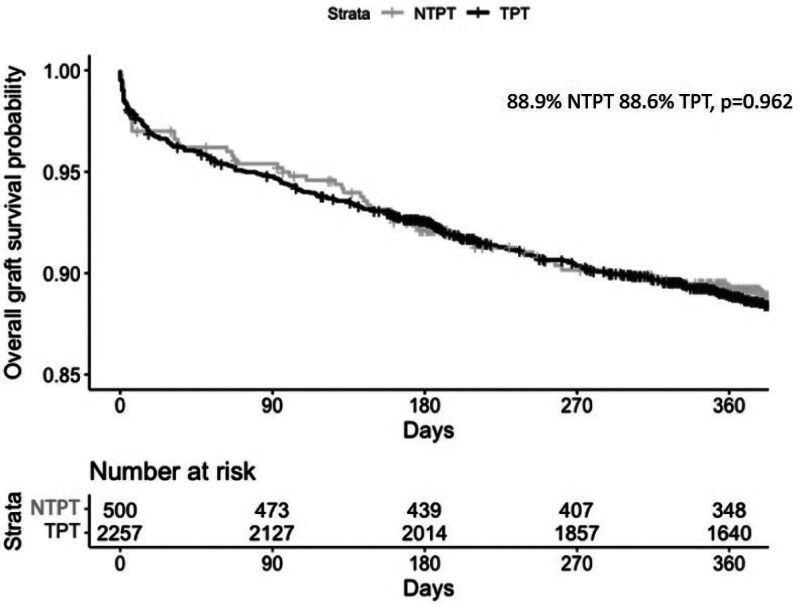
Results: Five hundred NTPT and 2257 TPT DCD transplants were identified: 1-y graft survival was 88.9 and 88.6%, respectively (P = 0.962). In a multivariable model, the origin of the procurement team was not associated with graft failure NTPT versus TPT (hazard ratio, 0.92; 95% confidence interval, 0.71-1.22; P = 0.57) but rather with known risks for DCD graft loss including donor age, degree of recipient illness, cold ischemic time, and retransplantation. The overall incidence of retransplantation and ischemic cholangiopathy as an indication for retransplantation were similar between NTPT and TPT.
Conclusions: This data suggests that transplant centers may be able to safely use DCD livers recovered by local surgical teams.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
