Serum procalcitonin and C-reactive protein as indices of early sepsis and mortality in North Indian pediatric burn injuries: a prospective evaluation and literature review.
{"title":"Serum procalcitonin and C-reactive protein as indices of early sepsis and mortality in North Indian pediatric burn injuries: a prospective evaluation and literature review.","authors":"Nupur Aggarwal, Durga Karki, Rajni Gaind, Monika Matlani, Vamseedharan Muthukumar","doi":"10.4266/acc.2023.00759","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Delays in diagnosing sepsis in children afflicted with thermal injuries can result in high morbidity and mortality. Our study evaluated the role of the biomarkers Procalcitonin (PCT) and C-reactive protein (CRP) as predictors of early sepsis and mortality, respectively, in this group of patients.</p><p><strong>Methods: </strong>This was a prospective evaluation of 90 pediatric burn cases treated at a tertiary care burn center in Northern India. Patients, aged 1-16 years, presenting within 24 hours of being burned, with >10% body surface area of burn injury were included in the study. Levels of PCT and CRP were measured on days 1, 3, 5, and 7. Patients were followed until discharge, 30th post-burn day, or death, whichever occurred first.</p><p><strong>Results: </strong>Sepsis was clinically present in 49 of 90 (54.4%) cases with a median 30% total body surface area (TBSA) of burns. Mortality was seen in 31 of 90 (34.4%) cases with a median of 35% TBSA burns. High PCT and CRP were seen in the sepsis group, particularly on days 3, 5, and 7. PCT was also significantly higher in the mortality group (days 1 and 3).</p><p><strong>Conclusions: </strong>While PCT was a good early predictor of sepsis and mortality in children with burns, CRP was reliable as a predictor of sepsis only. Both markers, however, can serve as adjuncts to culture sensitivity reports for diagnosing early onset sepsis and initiation of antibiotic therapy in appropriate patients.</p>","PeriodicalId":44118,"journal":{"name":"Acute and Critical Care","volume":"39 3","pages":"350-358"},"PeriodicalIF":2.0000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11392697/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acute and Critical Care","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4266/acc.2023.00759","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/30 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Delays in diagnosing sepsis in children afflicted with thermal injuries can result in high morbidity and mortality. Our study evaluated the role of the biomarkers Procalcitonin (PCT) and C-reactive protein (CRP) as predictors of early sepsis and mortality, respectively, in this group of patients.
Methods: This was a prospective evaluation of 90 pediatric burn cases treated at a tertiary care burn center in Northern India. Patients, aged 1-16 years, presenting within 24 hours of being burned, with >10% body surface area of burn injury were included in the study. Levels of PCT and CRP were measured on days 1, 3, 5, and 7. Patients were followed until discharge, 30th post-burn day, or death, whichever occurred first.
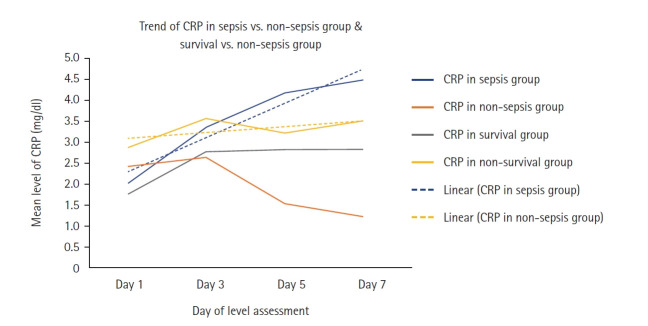
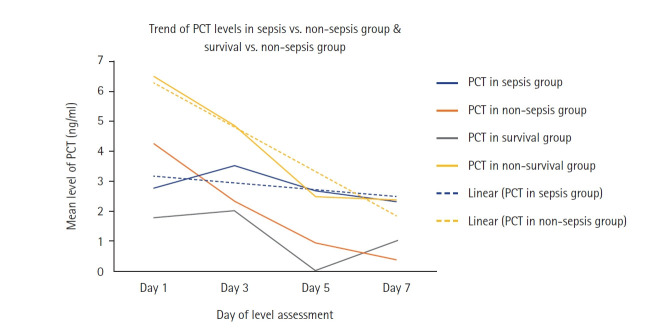
Results: Sepsis was clinically present in 49 of 90 (54.4%) cases with a median 30% total body surface area (TBSA) of burns. Mortality was seen in 31 of 90 (34.4%) cases with a median of 35% TBSA burns. High PCT and CRP were seen in the sepsis group, particularly on days 3, 5, and 7. PCT was also significantly higher in the mortality group (days 1 and 3).
Conclusions: While PCT was a good early predictor of sepsis and mortality in children with burns, CRP was reliable as a predictor of sepsis only. Both markers, however, can serve as adjuncts to culture sensitivity reports for diagnosing early onset sepsis and initiation of antibiotic therapy in appropriate patients.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
