John L Gore, Phoebe Wright, Vanessa Shih, Nancy N Chang, Sina Noshad, Gabriel G Rey, Steven Wang, Sujata Narayanan
{"title":"Development and Optimization of a Bladder Cancer Algorithm Using SEER-Medicare Claims Data.","authors":"John L Gore, Phoebe Wright, Vanessa Shih, Nancy N Chang, Sina Noshad, Gabriel G Rey, Steven Wang, Sujata Narayanan","doi":"10.1200/CCI.24.00073","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Categorizing patients with cancer by their disease stage can be an important tool when conducting administrative claims-based studies. As claims databases frequently do not capture this information, algorithms are increasingly used to define disease stage. To our knowledge, to date, no study has used an algorithm to categorize patients with bladder cancer (BC) by disease stage (non-muscle-invasive BC [NMIBC], muscle-invasive BC [MIBC], or locally advanced/metastatic urothelial carcinoma [la/mUC]) in a US-based health care claims database.</p><p><strong>Methods: </strong>A claims-based algorithm was developed to categorize patients by disease stage on the basis of the administrative claims portion of the SEER-Medicare linked data. The algorithm was validated against a reference SEER registry, and the algorithm's parameters were iteratively modified to improve its performance. Patients were included if they had an initial diagnosis of BC between January 2016 and December 2017 recorded in SEER registry data. Medicare claims data were available for these patients until December 31, 2019. The algorithm was evaluated by assessing percentage agreement, Cohen's kappa (κ), specificity, positive predictive value (PPV), and negative predictive value (NPV) against the SEER categorization.</p><p><strong>Results: </strong>A total of 15,484 patients with SEER-confirmed BC were included: 10,991 (71.0%) with NMIBC, 3,645 (23.5%) with MIBC, and 848 (5.5%) with la/mUC. After multiple rounds of algorithm optimization, the final algorithm had an agreement of 82.5% with SEER, with a κ of 0.58, a PPV of 87.0% for NMIBC, and 76.8% for MIBC and a high NPV for la/mUC of 98.0%.</p><p><strong>Conclusion: </strong>This claims-based algorithm could be a useful approach for researchers conducting claims-based studies categorizing patients with BC at diagnosis.</p>","PeriodicalId":51626,"journal":{"name":"JCO Clinical Cancer Informatics","volume":"8 ","pages":"e2400073"},"PeriodicalIF":2.8000,"publicationDate":"2024-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11421559/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JCO Clinical Cancer Informatics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1200/CCI.24.00073","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Categorizing patients with cancer by their disease stage can be an important tool when conducting administrative claims-based studies. As claims databases frequently do not capture this information, algorithms are increasingly used to define disease stage. To our knowledge, to date, no study has used an algorithm to categorize patients with bladder cancer (BC) by disease stage (non-muscle-invasive BC [NMIBC], muscle-invasive BC [MIBC], or locally advanced/metastatic urothelial carcinoma [la/mUC]) in a US-based health care claims database.
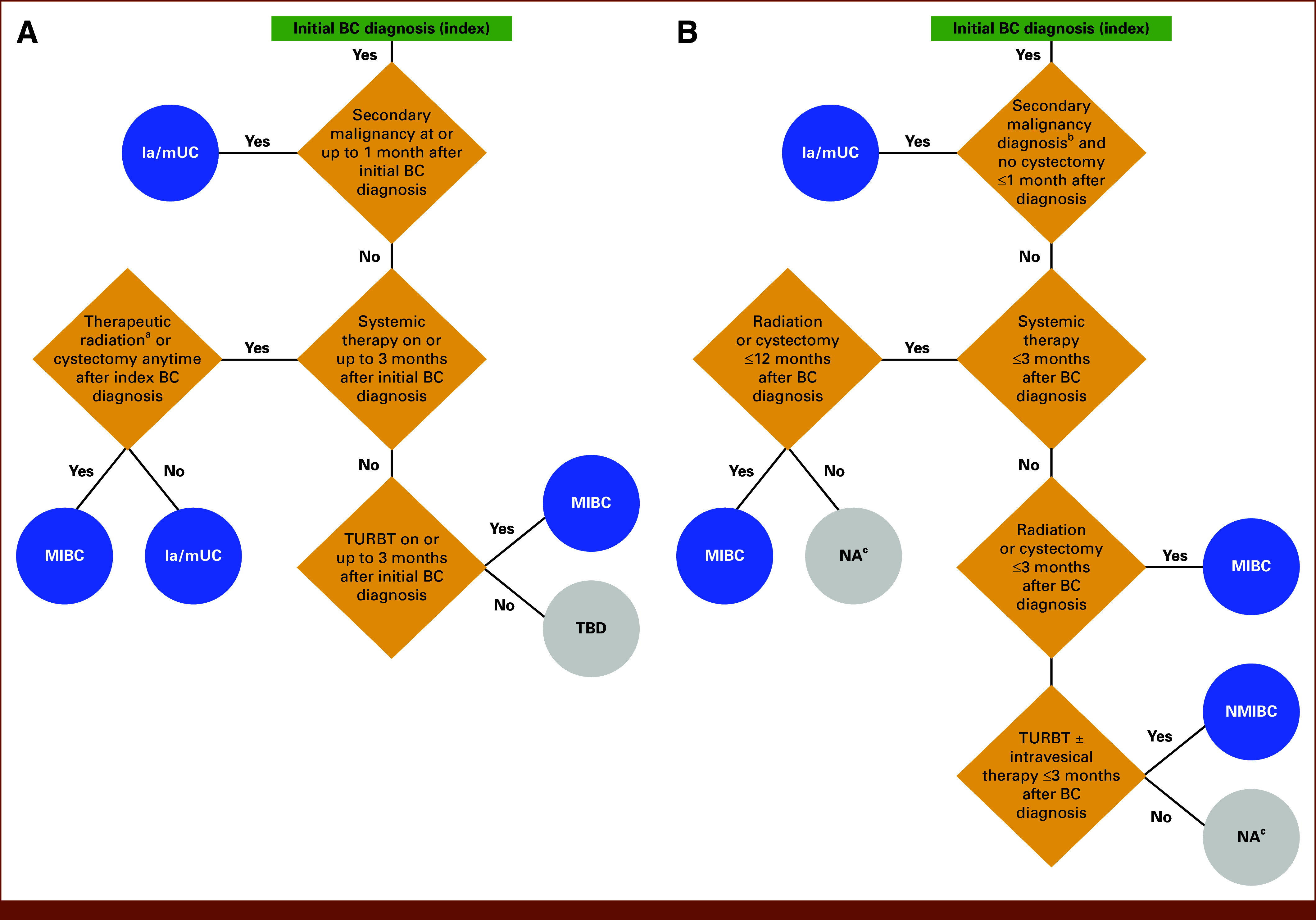
Methods: A claims-based algorithm was developed to categorize patients by disease stage on the basis of the administrative claims portion of the SEER-Medicare linked data. The algorithm was validated against a reference SEER registry, and the algorithm's parameters were iteratively modified to improve its performance. Patients were included if they had an initial diagnosis of BC between January 2016 and December 2017 recorded in SEER registry data. Medicare claims data were available for these patients until December 31, 2019. The algorithm was evaluated by assessing percentage agreement, Cohen's kappa (κ), specificity, positive predictive value (PPV), and negative predictive value (NPV) against the SEER categorization.
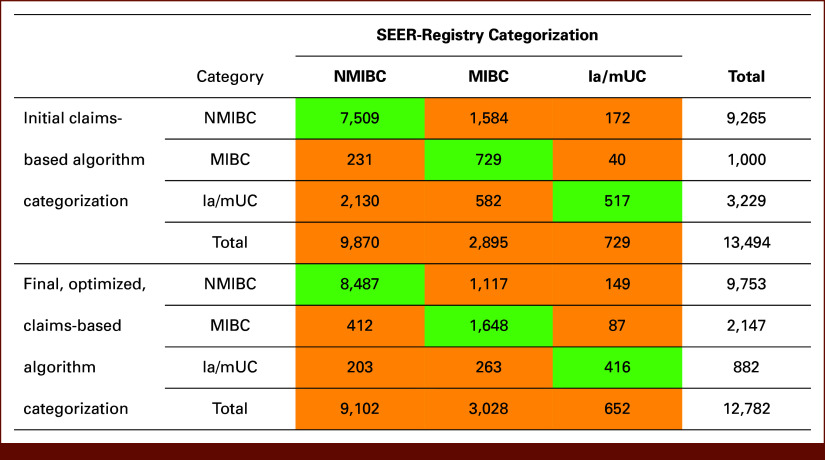
Results: A total of 15,484 patients with SEER-confirmed BC were included: 10,991 (71.0%) with NMIBC, 3,645 (23.5%) with MIBC, and 848 (5.5%) with la/mUC. After multiple rounds of algorithm optimization, the final algorithm had an agreement of 82.5% with SEER, with a κ of 0.58, a PPV of 87.0% for NMIBC, and 76.8% for MIBC and a high NPV for la/mUC of 98.0%.
Conclusion: This claims-based algorithm could be a useful approach for researchers conducting claims-based studies categorizing patients with BC at diagnosis.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
