Elaine Sang, Ryan Quinn, Michael A Stawnychy, Jiyoun Song, Karen B Hirschman, Sang Bin You, Katherine S Pitcher, Nancy A Hodgson, Patrik Garren, Melissa O'Connor, Sungho Oh, Kathryn H Bowles
{"title":"Organizational readiness for change towards implementing a sepsis survivor hospital to home transition-in-care protocol.","authors":"Elaine Sang, Ryan Quinn, Michael A Stawnychy, Jiyoun Song, Karen B Hirschman, Sang Bin You, Katherine S Pitcher, Nancy A Hodgson, Patrik Garren, Melissa O'Connor, Sungho Oh, Kathryn H Bowles","doi":"10.3389/frhs.2024.1436375","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Organizational readiness for change, defined as the collective preparedness of organization members to enact changes, remains understudied in implementing sepsis survivor transition-in-care protocols. Effective implementation relies on collaboration between hospital and post-acute care informants, including those who are leaders and staff. Therefore, our cross-sectional study compared organizational readiness for change among hospital and post-acute care informants.</p><p><strong>Methods: </strong>We invited informants from 16 hospitals and five affiliated HHC agencies involved in implementing a sepsis survivor transition-in-care protocol to complete a pre-implementation survey, where organizational readiness for change was measured via the Organizational Readiness to Implement Change (ORIC) scale (range 12-60). We also collected their demographic and job area information. Mann-Whitney <i>U</i>-tests and linear regressions, adjusting for leadership status, were used to compare organizational readiness of change between hospital and post-acute care informants.</p><p><strong>Results: </strong>Eighty-four informants, 51 from hospitals and 33 from post-acute care, completed the survey. Hospital and post-acute care informants had a median ORIC score of 52 and 57 respectively. Post-acute care informants had a mean 4.39-unit higher ORIC score compared to hospital informants (<i>p </i>= 0.03).</p><p><strong>Conclusions: </strong>Post-acute care informants had higher organizational readiness of change than hospital informants, potentially attributed to differences in health policies, expertise, organizational structure, and priorities. These findings and potential inferences may inform sepsis survivor transition-in-care protocol implementation. Future research should confirm, expand, and examine underlying factors related to these findings with a larger and more diverse sample. Additional studies may assess the predictive validity of ORIC towards implementation success.</p>","PeriodicalId":73088,"journal":{"name":"Frontiers in health services","volume":"4 ","pages":"1436375"},"PeriodicalIF":2.7000,"publicationDate":"2024-09-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11412944/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in health services","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3389/frhs.2024.1436375","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Organizational readiness for change, defined as the collective preparedness of organization members to enact changes, remains understudied in implementing sepsis survivor transition-in-care protocols. Effective implementation relies on collaboration between hospital and post-acute care informants, including those who are leaders and staff. Therefore, our cross-sectional study compared organizational readiness for change among hospital and post-acute care informants.
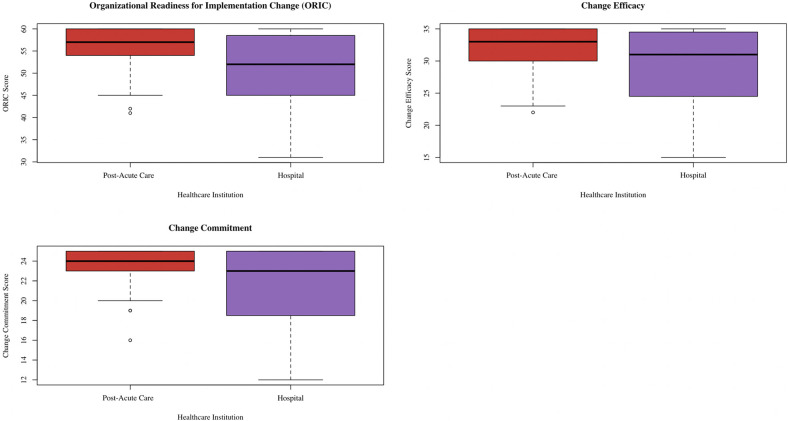
Methods: We invited informants from 16 hospitals and five affiliated HHC agencies involved in implementing a sepsis survivor transition-in-care protocol to complete a pre-implementation survey, where organizational readiness for change was measured via the Organizational Readiness to Implement Change (ORIC) scale (range 12-60). We also collected their demographic and job area information. Mann-Whitney U-tests and linear regressions, adjusting for leadership status, were used to compare organizational readiness of change between hospital and post-acute care informants.
Results: Eighty-four informants, 51 from hospitals and 33 from post-acute care, completed the survey. Hospital and post-acute care informants had a median ORIC score of 52 and 57 respectively. Post-acute care informants had a mean 4.39-unit higher ORIC score compared to hospital informants (p = 0.03).
Conclusions: Post-acute care informants had higher organizational readiness of change than hospital informants, potentially attributed to differences in health policies, expertise, organizational structure, and priorities. These findings and potential inferences may inform sepsis survivor transition-in-care protocol implementation. Future research should confirm, expand, and examine underlying factors related to these findings with a larger and more diverse sample. Additional studies may assess the predictive validity of ORIC towards implementation success.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
