Non-Medical Switching or Discontinuation Patterns among Patients with Non-Valvular Atrial Fibrillation Treated with Direct Oral Anticoagulants in the United States: A Claims-Based Analysis.
Michael Ingham, Hela Romdhani, Aarti Patel, Veronica Ashton, Gabrielle Caron-Lapointe, Anabelle Tardif-Samson, Patrick Lefebvre, Marie-Hélène Lafeuille
{"title":"Non-Medical Switching or Discontinuation Patterns among Patients with Non-Valvular Atrial Fibrillation Treated with Direct Oral Anticoagulants in the United States: A Claims-Based Analysis.","authors":"Michael Ingham, Hela Romdhani, Aarti Patel, Veronica Ashton, Gabrielle Caron-Lapointe, Anabelle Tardif-Samson, Patrick Lefebvre, Marie-Hélène Lafeuille","doi":"10.3390/jmahp12030020","DOIUrl":null,"url":null,"abstract":"<p><p>This study assessed direct-acting oral anticoagulant (DOAC) switching/discontinuation patterns in patients with non-valvular atrial fibrillation (NVAF) in 2019, by quarter (Q1-Q4), and associated socioeconomic risk factors. Adults with NVAF initiating stable DOAC treatment (July 2018-December 2018) were selected from Symphony Health Solutions' Patient Transactional Datasets (April 2017-January 2021). Switching/discontinuation rates were reported in 2019 Q1-Q4, separately. Non-medical switching/discontinuation (NMSD) was defined as the difference between switching/discontinuation rates in Q1 and mean rates across Q2-Q4. The associations of socioeconomic factors with switching/discontinuation were assessed. Of 46,793 patients (78.7% ≥ 65 years; 52.6% male; 7.7% Black), 18.0% switched/discontinued their initial DOAC in Q1 vs. 8.8% on average in Q2-Q4, corresponding to an NMSD of 9.2%. During the quarter following the switch/discontinuation, more patients who switched/discontinued in Q1 remained untreated (Q1: 77.0%; Q2: 74.3%; Q3: 71.2%) and fewer reinitiated initial DOAC (Q1: 17.6%; Q2: 20.8%; Q3: 24.0%). Factors associated with the risk of switching/discontinuation in Q1 were race, age, gender, insurance type, and household income (all <i>p</i> < 0.05). More patients with NVAF switched/discontinued DOACs in Q1 vs. Q2-Q4, and more of them tended to remain untreated relative to those who switched/discontinued later in the year, suggesting a potential long-term impact of NMSD. Findings on factors associated with switching/discontinuation highlight potential socioeconomic discrepancies in treatment continuity.</p>","PeriodicalId":73811,"journal":{"name":"Journal of market access & health policy","volume":"12 3","pages":"252-263"},"PeriodicalIF":0.0000,"publicationDate":"2024-09-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11417902/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of market access & health policy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/jmahp12030020","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
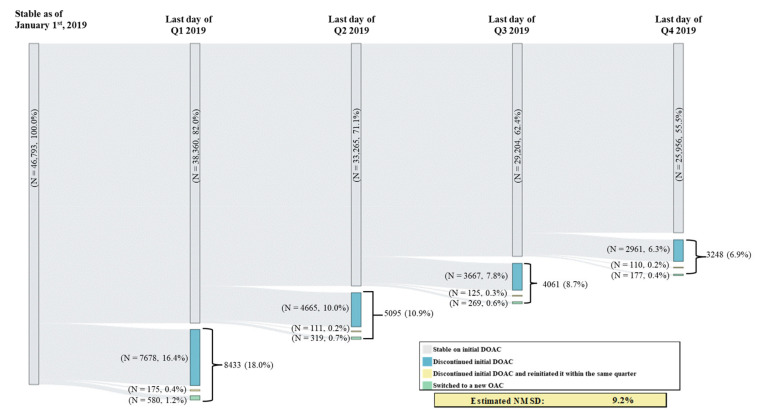
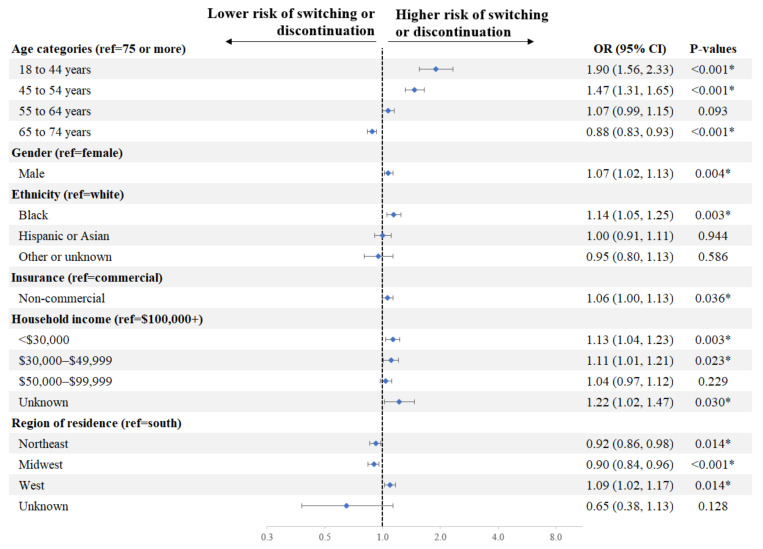
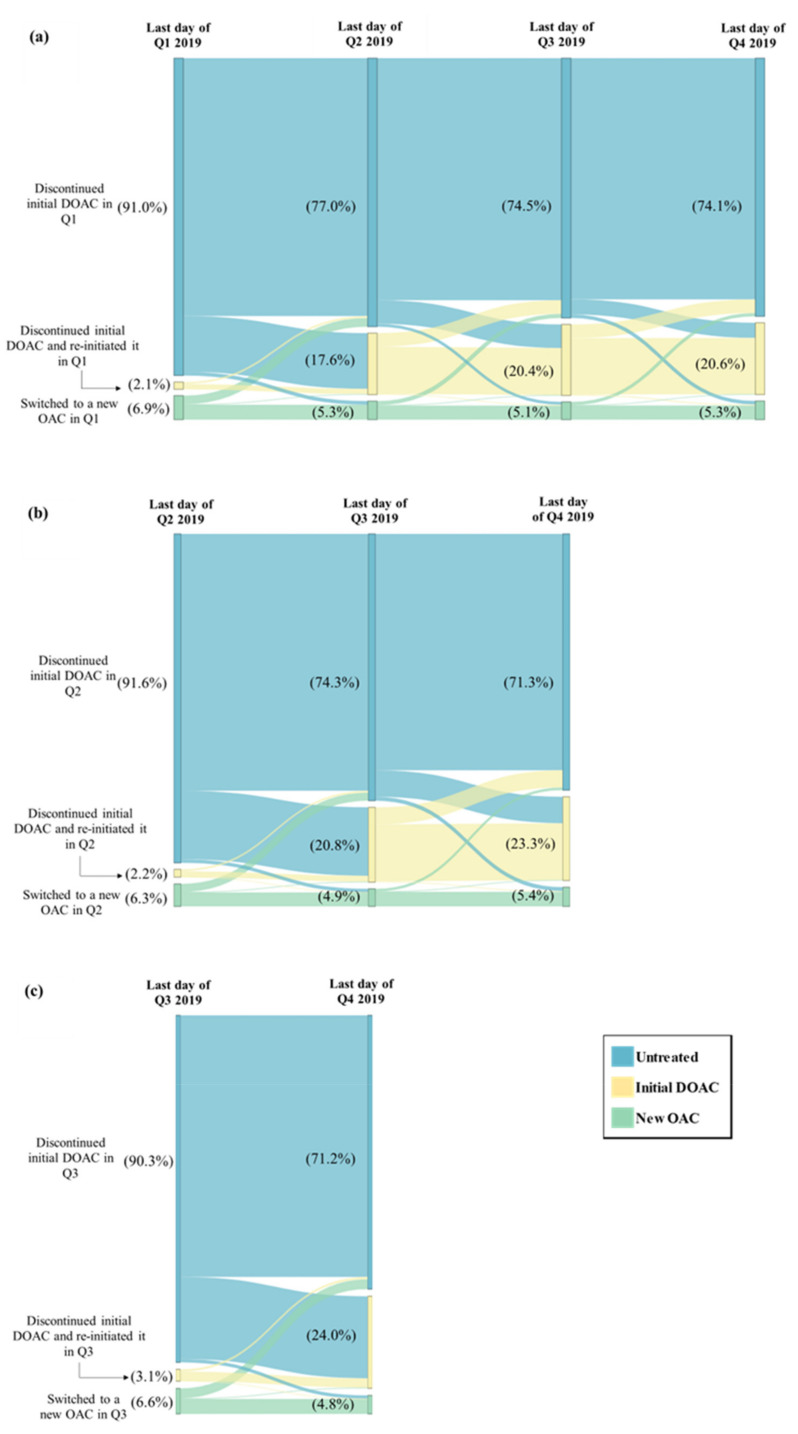
This study assessed direct-acting oral anticoagulant (DOAC) switching/discontinuation patterns in patients with non-valvular atrial fibrillation (NVAF) in 2019, by quarter (Q1-Q4), and associated socioeconomic risk factors. Adults with NVAF initiating stable DOAC treatment (July 2018-December 2018) were selected from Symphony Health Solutions' Patient Transactional Datasets (April 2017-January 2021). Switching/discontinuation rates were reported in 2019 Q1-Q4, separately. Non-medical switching/discontinuation (NMSD) was defined as the difference between switching/discontinuation rates in Q1 and mean rates across Q2-Q4. The associations of socioeconomic factors with switching/discontinuation were assessed. Of 46,793 patients (78.7% ≥ 65 years; 52.6% male; 7.7% Black), 18.0% switched/discontinued their initial DOAC in Q1 vs. 8.8% on average in Q2-Q4, corresponding to an NMSD of 9.2%. During the quarter following the switch/discontinuation, more patients who switched/discontinued in Q1 remained untreated (Q1: 77.0%; Q2: 74.3%; Q3: 71.2%) and fewer reinitiated initial DOAC (Q1: 17.6%; Q2: 20.8%; Q3: 24.0%). Factors associated with the risk of switching/discontinuation in Q1 were race, age, gender, insurance type, and household income (all p < 0.05). More patients with NVAF switched/discontinued DOACs in Q1 vs. Q2-Q4, and more of them tended to remain untreated relative to those who switched/discontinued later in the year, suggesting a potential long-term impact of NMSD. Findings on factors associated with switching/discontinuation highlight potential socioeconomic discrepancies in treatment continuity.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
