Shermila Pia, Elizabeth Stackhouse, Shehanaz Ellika
{"title":"A rare and devastating etiology of febrile seizure","authors":"Shermila Pia, Elizabeth Stackhouse, Shehanaz Ellika","doi":"10.1002/cns3.20080","DOIUrl":null,"url":null,"abstract":"<p>This 21-month-old boy with a history of multiple febrile seizures presented in refractory febrile status epilepticus. He had rhinorrhea and cough and tested positive for influenza type A. Cerebrospinal fluid analysis showed an elevated protein of 49 mg/dL (reference 10–32 mg/dL) with normal cells, glucose, lactate, meningitis/encephalitis, and autoimmune encephalitis panels. Magnetic resonance imaging revealed T2 hyperintensity, diffusion restriction, and susceptibility signal loss involving the bilateral cerebral cortices, cerebral white matter, thalami, basal ganglia, cerebellum, and brainstem (Figure 1). Metabolic screening and rapid whole-genome sequencing including <i>RANBP2</i> were unrevealing.</p><p>He was diagnosed with acute necrotizing encephalopathy (ANE) due to influenza A. He was treated with intravenous immunoglobulin (IVIG) and high-dose methylprednisolone. His course was complicated by severe paroxysmal sympathetic hyperactivity and prolonged hypoxic respiratory failure. Two months after the initial presentation, he had cortical blindness, diffuse spasticity, and dystonia without purposeful movements.</p><p>ANE is a rare but severe parainfectious disorder predominantly occuring in the pediatric age group and is associated with significant neurological morbidity and mortality.<span><sup>1, 2</sup></span> First described in 1997,<span><sup>3</sup></span> ANE typically presents with seizure and encephalopathy concomitant with viral illness. Influenza type A is the most commonly identified pathogen,<span><sup>1</sup></span> but many others have been implicated. More recently, familial/genetic ANE has been reported in association with pathogenic variants in <i>RANBP2</i>, and genetic testing is now recommended in the evaluation of these patients.<span><sup>1, 2</sup></span> Radiographically, ANE is characterized by symmetric T2 hyperintensity, diffusion restriction, and susceptibility signal loss in bilateral cerebral cortices, thalami, basal ganglia, cerebral white matter, brainstem, and cerebellar hemispheres.<span><sup>4, 5</sup></span> A characteristic trilaminar pattern of diffusion restriction on the apparent diffusion coefficient map in the thalami is specific for ANE,<span><sup>4, 5</sup></span> with the core demonstrating high signal intensity, pericore showing low signal intensity, and peripheral zone of high signal intensity, corresponding with pathologic findings of hemorrhagic necrosis in the core, pericore cytotoxic edema, and perilesional vasogenic edema.<span><sup>5</sup></span> The prognosis is poor, with less than 10% full recovery, nearly 30% mortality, and significant neurological morbidity in survivors.<span><sup>1, 2</sup></span> Early treatment with high-dose steroids is associated with improved outcomes.</p><p><b>Shermila Pia</b>: Conceptualization; writing—original draft; writing—review & editing. <b>Elizabeth Stackhouse</b>: Writing—review & editing. <b>Shehanaz Ellika</b>: Data curation; supervision; writing—review & editing.</p><p>The authors declare no conflicts of interest.</p>","PeriodicalId":72232,"journal":{"name":"Annals of the Child Neurology Society","volume":"2 3","pages":"251-252"},"PeriodicalIF":0.0000,"publicationDate":"2024-06-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cns3.20080","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of the Child Neurology Society","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cns3.20080","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
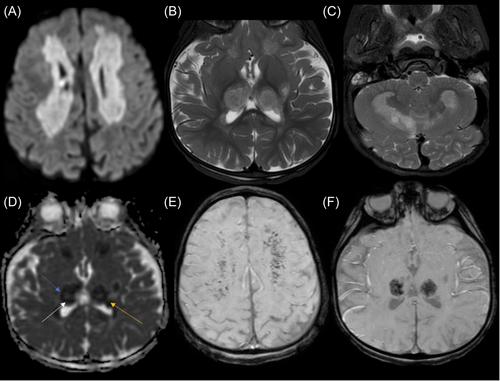
This 21-month-old boy with a history of multiple febrile seizures presented in refractory febrile status epilepticus. He had rhinorrhea and cough and tested positive for influenza type A. Cerebrospinal fluid analysis showed an elevated protein of 49 mg/dL (reference 10–32 mg/dL) with normal cells, glucose, lactate, meningitis/encephalitis, and autoimmune encephalitis panels. Magnetic resonance imaging revealed T2 hyperintensity, diffusion restriction, and susceptibility signal loss involving the bilateral cerebral cortices, cerebral white matter, thalami, basal ganglia, cerebellum, and brainstem (Figure 1). Metabolic screening and rapid whole-genome sequencing including RANBP2 were unrevealing.
He was diagnosed with acute necrotizing encephalopathy (ANE) due to influenza A. He was treated with intravenous immunoglobulin (IVIG) and high-dose methylprednisolone. His course was complicated by severe paroxysmal sympathetic hyperactivity and prolonged hypoxic respiratory failure. Two months after the initial presentation, he had cortical blindness, diffuse spasticity, and dystonia without purposeful movements.
ANE is a rare but severe parainfectious disorder predominantly occuring in the pediatric age group and is associated with significant neurological morbidity and mortality.1, 2 First described in 1997,3 ANE typically presents with seizure and encephalopathy concomitant with viral illness. Influenza type A is the most commonly identified pathogen,1 but many others have been implicated. More recently, familial/genetic ANE has been reported in association with pathogenic variants in RANBP2, and genetic testing is now recommended in the evaluation of these patients.1, 2 Radiographically, ANE is characterized by symmetric T2 hyperintensity, diffusion restriction, and susceptibility signal loss in bilateral cerebral cortices, thalami, basal ganglia, cerebral white matter, brainstem, and cerebellar hemispheres.4, 5 A characteristic trilaminar pattern of diffusion restriction on the apparent diffusion coefficient map in the thalami is specific for ANE,4, 5 with the core demonstrating high signal intensity, pericore showing low signal intensity, and peripheral zone of high signal intensity, corresponding with pathologic findings of hemorrhagic necrosis in the core, pericore cytotoxic edema, and perilesional vasogenic edema.5 The prognosis is poor, with less than 10% full recovery, nearly 30% mortality, and significant neurological morbidity in survivors.1, 2 Early treatment with high-dose steroids is associated with improved outcomes.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
