{"title":"Pathological Assessment of Men with Grade Group 2 Prostate Cancer.","authors":"Anika Jain, Lawrence Kim, Manish I Patel","doi":"10.5534/wjmh.230216","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>A variety of treatment options are now available for men with localized prostate cancer (PC); however, there is still debate in determining how and when to intervene for Grade Group (GG) 2 disease. Our study aims to formulate strategies to identify men at risk of upgrading and having adverse pathological outcomes.</p><p><strong>Materials and methods: </strong>This retrospective study includes 243 patients with GG2 PC that were treated with radical prostatectomy between 2015 and 2021. Patients on active surveillance, previous history of prostate biopsy, hormonal and/or radiation therapy prior to surgery were excluded from this study. A retrospective analysis was conducted using clinicopathological data obtained from medical records.</p><p><strong>Results: </strong>Prostate-specific antigen (PSA) and Prostate Imaging Reporting and Data System (PI-RADS) score were statistically significant variables for risk of upgrading. In men who had presence of composite poor outcomes, PSA, PI-RADS score, presence of extraprostatic extension and seminal vesical invasion on MRI, number of positive cores, percentage of high grade (pattern 4/5) on prostate biopsy and Gleason pattern 4 volume on biopsy were all statistically significant variables. Strategy 8 (PI-RADS 5 lesion or percentage high grade [Gleason pattern 4] on prostate biopsy grade >10% or >3 cores positive on prostate biopsy) had significant association to identifying the highest number of men with upgrading and composite poor outcomes.</p><p><strong>Conclusions: </strong>Our study supports the use of strategy 8 in treatment decision making of men with GG2 PC. Further validation of the use of this strategy is warranted.</p>","PeriodicalId":54261,"journal":{"name":"World Journal of Mens Health","volume":" ","pages":"595-602"},"PeriodicalIF":4.1000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12257331/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Mens Health","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5534/wjmh.230216","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/14 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ANDROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: A variety of treatment options are now available for men with localized prostate cancer (PC); however, there is still debate in determining how and when to intervene for Grade Group (GG) 2 disease. Our study aims to formulate strategies to identify men at risk of upgrading and having adverse pathological outcomes.
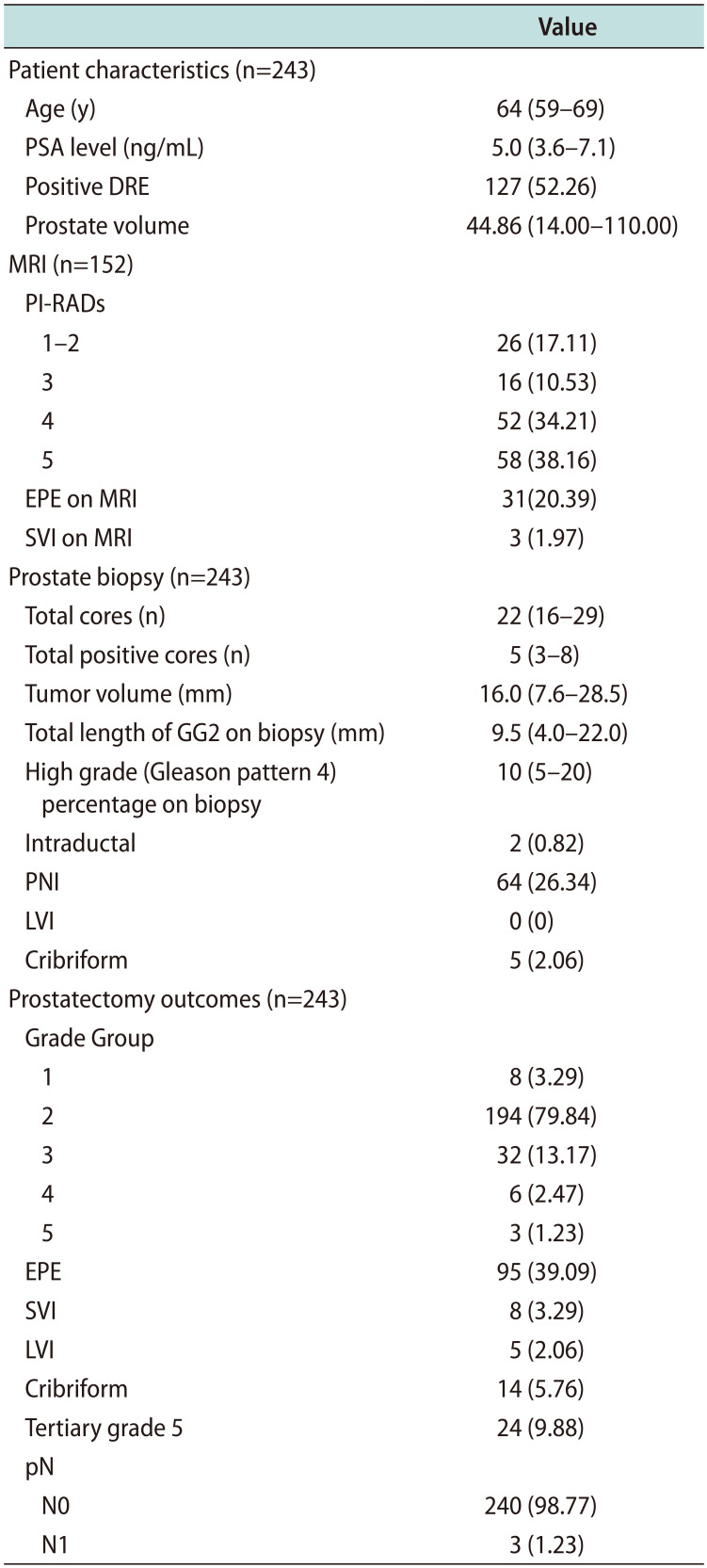
Materials and methods: This retrospective study includes 243 patients with GG2 PC that were treated with radical prostatectomy between 2015 and 2021. Patients on active surveillance, previous history of prostate biopsy, hormonal and/or radiation therapy prior to surgery were excluded from this study. A retrospective analysis was conducted using clinicopathological data obtained from medical records.
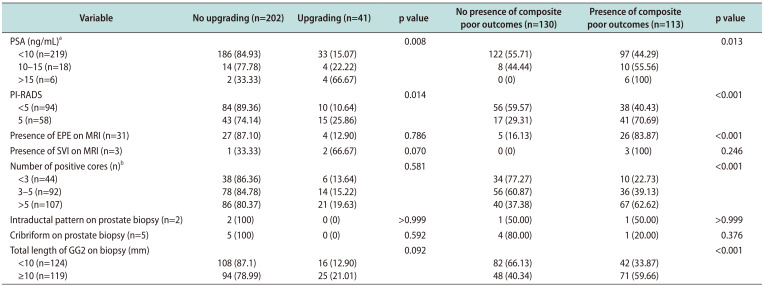
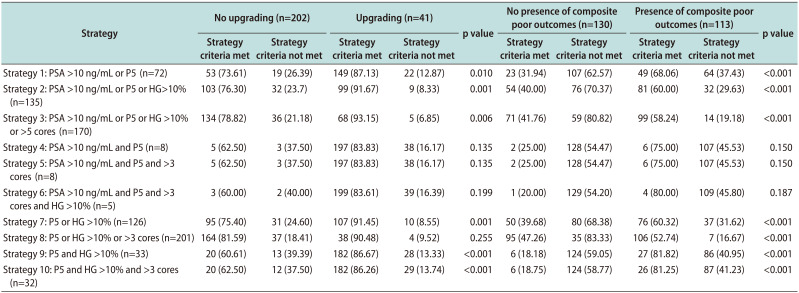
Results: Prostate-specific antigen (PSA) and Prostate Imaging Reporting and Data System (PI-RADS) score were statistically significant variables for risk of upgrading. In men who had presence of composite poor outcomes, PSA, PI-RADS score, presence of extraprostatic extension and seminal vesical invasion on MRI, number of positive cores, percentage of high grade (pattern 4/5) on prostate biopsy and Gleason pattern 4 volume on biopsy were all statistically significant variables. Strategy 8 (PI-RADS 5 lesion or percentage high grade [Gleason pattern 4] on prostate biopsy grade >10% or >3 cores positive on prostate biopsy) had significant association to identifying the highest number of men with upgrading and composite poor outcomes.
Conclusions: Our study supports the use of strategy 8 in treatment decision making of men with GG2 PC. Further validation of the use of this strategy is warranted.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
