Sushil K Mehandru, Supreet Kaur, Avais Masud, Kyrillos Rezkalla, Qalb Khan, Prit Paul Singh, Eric Constanzo, Walid Abboud, Tushar Vachharajani, Arif Asif
{"title":"Role of Continuous Drainage of Tense Ascites in Peritoneal Dialysis: Mehandru/Masud Technique.","authors":"Sushil K Mehandru, Supreet Kaur, Avais Masud, Kyrillos Rezkalla, Qalb Khan, Prit Paul Singh, Eric Constanzo, Walid Abboud, Tushar Vachharajani, Arif Asif","doi":"10.14740/jmc4056","DOIUrl":null,"url":null,"abstract":"<p><p>Insertion of a peritoneal dialysis (PD) catheter in end-stage renal disease (ESRD) patients with cirrhosis and tense ascites remains a challenge for nephrologists. Ascitic fluid leak at the surgical site, a common postoperative occurrence, leads to the disqualification of many patients who could be otherwise great candidates for PD. The ascitic fluid leak has been described to occur during or immediately after surgery even after the entire volume of ascitic fluid has been drained. In this study, we report a case study of three patients with ESRD, liver cirrhosis, and tense ascites on hemodialysis. The patients required super large volume paracentesis (SLVP), draining 9,000 - 15,000 cc of ascitic fluid twice weekly in an interventional radiology setup. Besides ascitic fluid drainage, the patients needed in-center hemodialysis (ICHD) 3 days a week, leading to their engagement in procedures 5 days a week. In addition, intradialytic symptomatic hypotension, hypoalbuminemia, and other adverse effects of hemodialysis lead to their poor lifestyle. To improve their lifestyle, all patients desired to switch to PD from ICHD. Upon the PD catheter insertion and drainage of the entire ascitic fluid, leaks developed at the insertion site within a few hours. To overcome these leaks, PD catheters of all three patients were attached via a transfer set to a bag for continuous drainage of ascitic fluid for about 2 weeks. No leak or complication was noted, leading to complete healing of insertion site. We recommend, for the patients with tense ascites requiring SLVP, approximately 2 weeks of healing period continuously be performed till initiation of PD training,.</p>","PeriodicalId":101328,"journal":{"name":"Journal of medical cases","volume":"15 10","pages":"287-296"},"PeriodicalIF":0.9000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11424101/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of medical cases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jmc4056","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/20 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
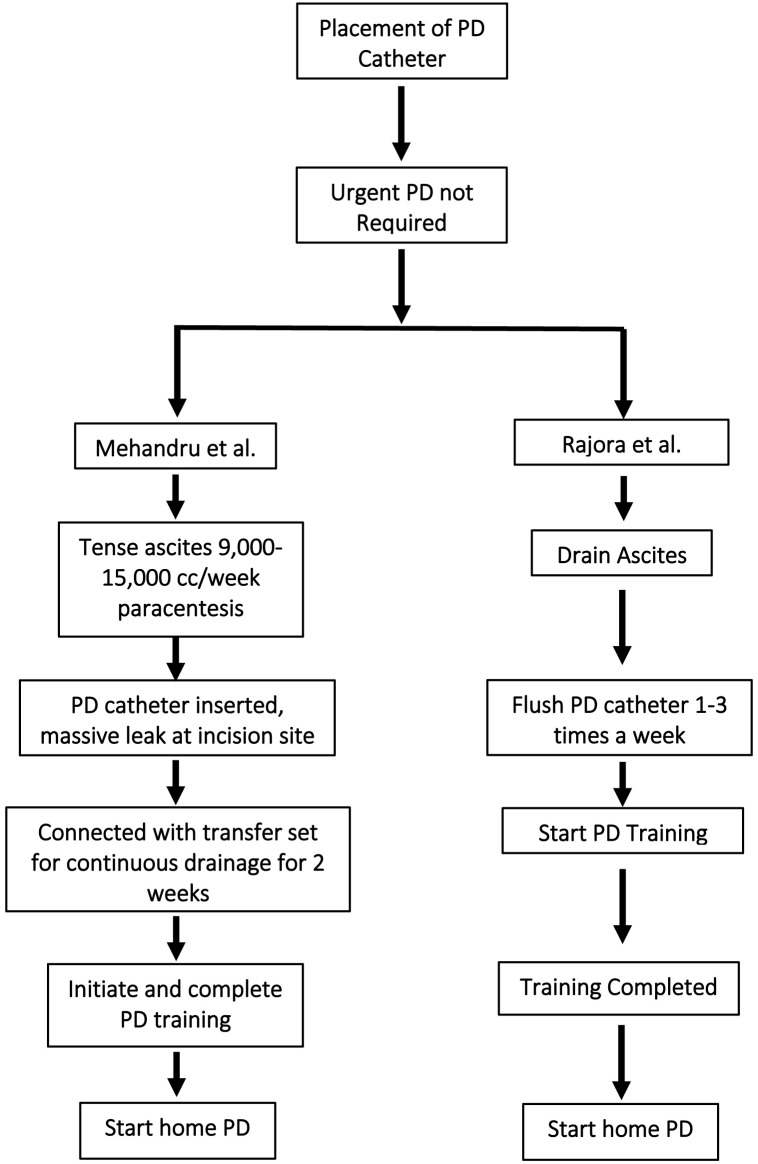
Insertion of a peritoneal dialysis (PD) catheter in end-stage renal disease (ESRD) patients with cirrhosis and tense ascites remains a challenge for nephrologists. Ascitic fluid leak at the surgical site, a common postoperative occurrence, leads to the disqualification of many patients who could be otherwise great candidates for PD. The ascitic fluid leak has been described to occur during or immediately after surgery even after the entire volume of ascitic fluid has been drained. In this study, we report a case study of three patients with ESRD, liver cirrhosis, and tense ascites on hemodialysis. The patients required super large volume paracentesis (SLVP), draining 9,000 - 15,000 cc of ascitic fluid twice weekly in an interventional radiology setup. Besides ascitic fluid drainage, the patients needed in-center hemodialysis (ICHD) 3 days a week, leading to their engagement in procedures 5 days a week. In addition, intradialytic symptomatic hypotension, hypoalbuminemia, and other adverse effects of hemodialysis lead to their poor lifestyle. To improve their lifestyle, all patients desired to switch to PD from ICHD. Upon the PD catheter insertion and drainage of the entire ascitic fluid, leaks developed at the insertion site within a few hours. To overcome these leaks, PD catheters of all three patients were attached via a transfer set to a bag for continuous drainage of ascitic fluid for about 2 weeks. No leak or complication was noted, leading to complete healing of insertion site. We recommend, for the patients with tense ascites requiring SLVP, approximately 2 weeks of healing period continuously be performed till initiation of PD training,.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
