Advancing microvascular invasion diagnosis: a multi-center investigation of novel MRI-based models for precise detection and classification in early-stage small hepatocellular carcinoma (≤ 3 cm)
Mengting Gu, Sisi Zhang, Wenjie Zou, Xingyu Zhao, Huilin Chen, RuiLin He, Ningyang Jia, Kairong Song, Wanmin Liu, Peijun Wang
{"title":"Advancing microvascular invasion diagnosis: a multi-center investigation of novel MRI-based models for precise detection and classification in early-stage small hepatocellular carcinoma (≤ 3 cm)","authors":"Mengting Gu, Sisi Zhang, Wenjie Zou, Xingyu Zhao, Huilin Chen, RuiLin He, Ningyang Jia, Kairong Song, Wanmin Liu, Peijun Wang","doi":"10.1007/s00261-024-04463-w","DOIUrl":null,"url":null,"abstract":"<div><h3>Purpose</h3><p>This study aimed to develop two preoperative magnetic resonance imaging (MRI) based models for detecting and classifying microvascular invasion (MVI) in early-stage small hepatocellular carcinoma (sHCC) patients.</p><h3>Methods</h3><p>MVI is graded as M0 (no invasion), M1 (invasion of five or fewer vessels located within 1 cm of the tumor’s peritumoral region), and M2 (invasion of more than five vessels or those located more than 1 cm from the tumor’s surface). This study enrolled 395 early-stage sHCC (≤ 3 cm) patients from three centers who underwent preoperative gadopentetate-enhanced MRI. From the first two centers, 310 patients were randomly divided into training (n = 217) and validation (n = 93) cohorts in a 7:3 ratio to develop the first model for predicting MVI presence. Among these, 153 patients with identified MVI were further divided into training (n = 112) and validation (n = 41) cohorts, using the same ratio, to construct the second model for MVI classification. An independent test cohort of 85 patients from the third center to validate both models. Univariate and multivariate logistic regression analyses identified independent predictors of MVI and its classification in the training cohorts. Based on these predictors, two nomograms were developed and assessed for their discriminative ability, calibration, and clinical usefulness. Besides, considering the two models are supposed applied in a serial fashion in the real clinical setting, we evaluate the performance of the two models together on the test cohorts by applying them simultaneously. Kaplan–Meier survival curve analysis was employed to assess the correlation between predicted MVI status and early recurrence, similar to the association observed with actual MVI status and early recurrence.</p><h3>Results</h3><p>The MVI detection nomogram, with platelet count (PLT), activated partial thromboplastin time (APTT), rim arterial phase hyperenhancement (Rim APHE) and arterial peritumoral enhancement, achieved area under the curve (AUC) of 0.827, 0.761 and 0.798 in the training, validation, and test cohorts, respectively. The MVI classification nomogram, integrating Total protein (TP), Shape, Arterial peritumoral enhancement and enhancement pattern, achieved AUC of 0.824, 0.772, and 0.807 across the three cohorts. When the two models were applied on the test cohorts in a serial fashion, they both demonstrated good performance, which means the two models had good clinical applicability. Calibration and decision curve analysis (DCA) results affirmed the model’s reliability and clinical utility. Notably, early recurrence was more prevalent in the MVI grade 2 (M2) group compared to the MVI-absent and M1 groups, regardless of the actual or predicted MVI status.</p><h3>Conclusions</h3><p>The nomograms exhibited excellent predictive performance for detecting and classifying MVI in patients with early-stage sHCC, particularly identifying high-risk M2 patients preoperatively.</p></div>","PeriodicalId":7126,"journal":{"name":"Abdominal Radiology","volume":"50 5","pages":"1986 - 1999"},"PeriodicalIF":2.2000,"publicationDate":"2024-09-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Abdominal Radiology","FirstCategoryId":"3","ListUrlMain":"https://link.springer.com/article/10.1007/s00261-024-04463-w","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose
This study aimed to develop two preoperative magnetic resonance imaging (MRI) based models for detecting and classifying microvascular invasion (MVI) in early-stage small hepatocellular carcinoma (sHCC) patients.
Methods
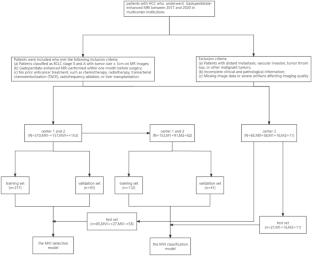
MVI is graded as M0 (no invasion), M1 (invasion of five or fewer vessels located within 1 cm of the tumor’s peritumoral region), and M2 (invasion of more than five vessels or those located more than 1 cm from the tumor’s surface). This study enrolled 395 early-stage sHCC (≤ 3 cm) patients from three centers who underwent preoperative gadopentetate-enhanced MRI. From the first two centers, 310 patients were randomly divided into training (n = 217) and validation (n = 93) cohorts in a 7:3 ratio to develop the first model for predicting MVI presence. Among these, 153 patients with identified MVI were further divided into training (n = 112) and validation (n = 41) cohorts, using the same ratio, to construct the second model for MVI classification. An independent test cohort of 85 patients from the third center to validate both models. Univariate and multivariate logistic regression analyses identified independent predictors of MVI and its classification in the training cohorts. Based on these predictors, two nomograms were developed and assessed for their discriminative ability, calibration, and clinical usefulness. Besides, considering the two models are supposed applied in a serial fashion in the real clinical setting, we evaluate the performance of the two models together on the test cohorts by applying them simultaneously. Kaplan–Meier survival curve analysis was employed to assess the correlation between predicted MVI status and early recurrence, similar to the association observed with actual MVI status and early recurrence.
Results
The MVI detection nomogram, with platelet count (PLT), activated partial thromboplastin time (APTT), rim arterial phase hyperenhancement (Rim APHE) and arterial peritumoral enhancement, achieved area under the curve (AUC) of 0.827, 0.761 and 0.798 in the training, validation, and test cohorts, respectively. The MVI classification nomogram, integrating Total protein (TP), Shape, Arterial peritumoral enhancement and enhancement pattern, achieved AUC of 0.824, 0.772, and 0.807 across the three cohorts. When the two models were applied on the test cohorts in a serial fashion, they both demonstrated good performance, which means the two models had good clinical applicability. Calibration and decision curve analysis (DCA) results affirmed the model’s reliability and clinical utility. Notably, early recurrence was more prevalent in the MVI grade 2 (M2) group compared to the MVI-absent and M1 groups, regardless of the actual or predicted MVI status.
Conclusions
The nomograms exhibited excellent predictive performance for detecting and classifying MVI in patients with early-stage sHCC, particularly identifying high-risk M2 patients preoperatively.
期刊介绍:
Abdominal Radiology seeks to meet the professional needs of the abdominal radiologist by publishing clinically pertinent original, review and practice related articles on the gastrointestinal and genitourinary tracts and abdominal interventional and radiologic procedures. Case reports are generally not accepted unless they are the first report of a new disease or condition, or part of a special solicited section.
Reasons to Publish Your Article in Abdominal Radiology:
· Official journal of the Society of Abdominal Radiology (SAR)
· Published in Cooperation with:
European Society of Gastrointestinal and Abdominal Radiology (ESGAR)
European Society of Urogenital Radiology (ESUR)
Asian Society of Abdominal Radiology (ASAR)
· Efficient handling and Expeditious review
· Author feedback is provided in a mentoring style
· Global readership
· Readers can earn CME credits




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
