Impact of residual mitral regurgitation after transcatheter edge-to-edge repair in atrial functional mitral regurgitation: Results from MITRA-PRO registry
Dennis Rottländer MD, Jörg Hausleiter MD, Thomas Schmitz MD, Alexander Bufe MD, Melchior Seyfarth MD, Ralph Stephan von Bardeleben MD, Harald Beucher MD, Taoufik Ouarrak, Steffen Schneider, Peter Boekstegers MD, MITRA-PRO Investigators
{"title":"Impact of residual mitral regurgitation after transcatheter edge-to-edge repair in atrial functional mitral regurgitation: Results from MITRA-PRO registry","authors":"Dennis Rottländer MD, Jörg Hausleiter MD, Thomas Schmitz MD, Alexander Bufe MD, Melchior Seyfarth MD, Ralph Stephan von Bardeleben MD, Harald Beucher MD, Taoufik Ouarrak, Steffen Schneider, Peter Boekstegers MD, MITRA-PRO Investigators","doi":"10.1002/ccd.31242","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Transcatheter edge-to-edge repair (TEER) has emerged to address symptomatic atrial functional mitral regurgitation (aFMR) in patients who are at high operative risk.</p>\n </section>\n \n <section>\n \n <h3> Aims</h3>\n \n <p>No clinical data is available on the impact of residual mitral regurgitation (MR) following TEER in aFMR compared to ventricular functional MR (vFMR).</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>In the MITRA-PRO registry, 846 patients with FMR and MitraScore assessment for residual MR quantification were included (722 patients with vFMR and 124 patients with aFMR).</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Compared to vFMR similar procedural results in regard of residual MR following TEER were found in aFMR patients (MitraScore post TEER 2.5 ± 1.8 vs. 2.7 ± 1.9), while the amount of implanted TEER devices was increased in vFMR. 1-year survival was better in aFMR compared to vFMR regardless of relevant residual MR (MitraScore ≥ 4), while 1-year rehospitalization was comparable for both MR entities. Patients with aFMR and mild residual MR had a lower mortality rate (6.6% vs. 10.3%) and rehospitalization rate (29.1% vs. 46.2%) 1 year after mitral TEER. However, in contrast to vFMR a MitraScore ≥4 was no independent predictor of mortality in aFMR indicating a better tolerance toward residual MR.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Residual MR is an independent predictor of 1-year mortality in vFMR patients, whereas in aFMR patients, a MitraScore of ≥4 is associated with higher mortality but is not an independent predictor in multivariate analysis. Therefore, minimizing MR through mitral TEER is crucial for survival in vFMR patients, while aFMR patients tolerate significant residual MR better 1 year after the procedure.</p>\n </section>\n </div>","PeriodicalId":9650,"journal":{"name":"Catheterization and Cardiovascular Interventions","volume":"104 5","pages":"1015-1026"},"PeriodicalIF":1.9000,"publicationDate":"2024-09-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ccd.31242","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Catheterization and Cardiovascular Interventions","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ccd.31242","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Transcatheter edge-to-edge repair (TEER) has emerged to address symptomatic atrial functional mitral regurgitation (aFMR) in patients who are at high operative risk.
Aims
No clinical data is available on the impact of residual mitral regurgitation (MR) following TEER in aFMR compared to ventricular functional MR (vFMR).
Methods
In the MITRA-PRO registry, 846 patients with FMR and MitraScore assessment for residual MR quantification were included (722 patients with vFMR and 124 patients with aFMR).
Results
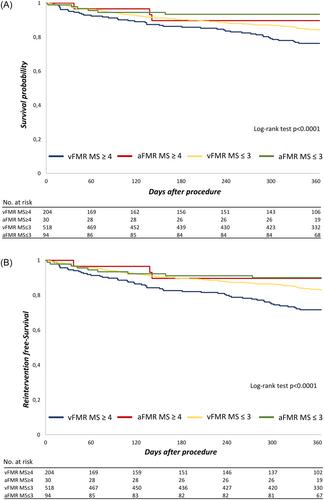
Compared to vFMR similar procedural results in regard of residual MR following TEER were found in aFMR patients (MitraScore post TEER 2.5 ± 1.8 vs. 2.7 ± 1.9), while the amount of implanted TEER devices was increased in vFMR. 1-year survival was better in aFMR compared to vFMR regardless of relevant residual MR (MitraScore ≥ 4), while 1-year rehospitalization was comparable for both MR entities. Patients with aFMR and mild residual MR had a lower mortality rate (6.6% vs. 10.3%) and rehospitalization rate (29.1% vs. 46.2%) 1 year after mitral TEER. However, in contrast to vFMR a MitraScore ≥4 was no independent predictor of mortality in aFMR indicating a better tolerance toward residual MR.
Conclusions
Residual MR is an independent predictor of 1-year mortality in vFMR patients, whereas in aFMR patients, a MitraScore of ≥4 is associated with higher mortality but is not an independent predictor in multivariate analysis. Therefore, minimizing MR through mitral TEER is crucial for survival in vFMR patients, while aFMR patients tolerate significant residual MR better 1 year after the procedure.
期刊介绍:
Catheterization and Cardiovascular Interventions is an international journal covering the broad field of cardiovascular diseases. Subject material includes basic and clinical information that is derived from or related to invasive and interventional coronary or peripheral vascular techniques. The journal focuses on material that will be of immediate practical value to physicians providing patient care in the clinical laboratory setting. To accomplish this, the journal publishes Preliminary Reports and Work In Progress articles that complement the traditional Original Studies, Case Reports, and Comprehensive Reviews. Perspective and insight concerning controversial subjects and evolving technologies are provided regularly through Editorial Commentaries furnished by members of the Editorial Board and other experts. Articles are subject to double-blind peer review and complete editorial evaluation prior to any decision regarding acceptability.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
