A Comparative Analysis of Clinical Symptoms and Modified Pouchitis Disease Activity Index Among Endoscopic Phenotypes of the J Pouch in Patients With Inflammatory Bowel Disease.
Shintaro Akiyama, Nathaniel A Cohen, Jacob E Ollech, Cindy Traboulsi, Tina Rodriguez, Victoria Rai, Laura R Glick, Yangtian Yi, Joseph Runde, Russell D Cohen, Kinga B Skowron, Roger D Hurst, Konstantin Umanskiy, Benjamin D Shogan, Neil H Hyman, Michele A Rubin, Sushila R Dalal, Atsushi Sakuraba, Joel Pekow, Eugene B Chang, David T Rubin
{"title":"A Comparative Analysis of Clinical Symptoms and Modified Pouchitis Disease Activity Index Among Endoscopic Phenotypes of the J Pouch in Patients With Inflammatory Bowel Disease.","authors":"Shintaro Akiyama, Nathaniel A Cohen, Jacob E Ollech, Cindy Traboulsi, Tina Rodriguez, Victoria Rai, Laura R Glick, Yangtian Yi, Joseph Runde, Russell D Cohen, Kinga B Skowron, Roger D Hurst, Konstantin Umanskiy, Benjamin D Shogan, Neil H Hyman, Michele A Rubin, Sushila R Dalal, Atsushi Sakuraba, Joel Pekow, Eugene B Chang, David T Rubin","doi":"10.1093/crocol/otae045","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The modified pouchitis disease activity index (mPDAI) based on clinical symptoms and endoscopic findings is used to diagnose pouchitis, but validated instruments to monitor pouchitis are still lacking. We recently established an endoscopic classification that described 7 endoscopic phenotypes with different outcomes. We assessed symptoms and compared mPDAIs among phenotypes in inflammatory bowel disease (IBD).</p><p><strong>Methods: </strong>We retrospectively reviewed pouchoscopies and classified them into 7 main phenotypes: normal (<i>n</i> = 25), afferent limb (AL) involvement (<i>n</i> = 4), inlet involvement (<i>n</i> = 14), diffuse (<i>n</i> = 7), focal inflammation of the pouch body (<i>n</i> = 25), cuffitis (<i>n</i> = 18), and pouch-related fistulas (<i>n</i> = 10) with a single phenotype were included. Complete-case analysis was conducted.</p><p><strong>Results: </strong>One hundred and three IBD patients were included. The median mPDAI was 0 (IQR 0-1.0) in patients with a normal pouch. Among inflammatory phenotypes, the highest median mPDAI was 4.0 (IQR 2.25-4.75) in cuffitis, followed by 3.0 (IQR 2.5-4.0) in diffuse inflammation, 2.5 (IQR 1.25-4.0) in inlet involvement, 2.5 (IQR 2.0-3.5) in AL involvement, 2.0 (IQR 1.0-3.0) in focal inflammation, and 1.0 (IQR 0.25-2.0) in the fistula phenotype. Perianal symptoms were frequently observed in pouch-related fistulas (8/10, 80%) and cuffitis (13/15, 87%). Among patients with cuffitis, all had incomplete emptying (6/6, 100%).</p><p><strong>Conclusions: </strong>We correlated the mPDAI with the endoscopic phenotypes and described the limited utility of symptoms in distinguishing between inflammatory phenotypes. Further studies are warranted to understand which symptoms should be monitored for each phenotype and whether mPDAI can be minimized after pouch normalization.</p>","PeriodicalId":10847,"journal":{"name":"Crohn's & Colitis 360","volume":"6 3","pages":"otae045"},"PeriodicalIF":1.8000,"publicationDate":"2024-08-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11438232/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Crohn's & Colitis 360","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/crocol/otae045","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The modified pouchitis disease activity index (mPDAI) based on clinical symptoms and endoscopic findings is used to diagnose pouchitis, but validated instruments to monitor pouchitis are still lacking. We recently established an endoscopic classification that described 7 endoscopic phenotypes with different outcomes. We assessed symptoms and compared mPDAIs among phenotypes in inflammatory bowel disease (IBD).
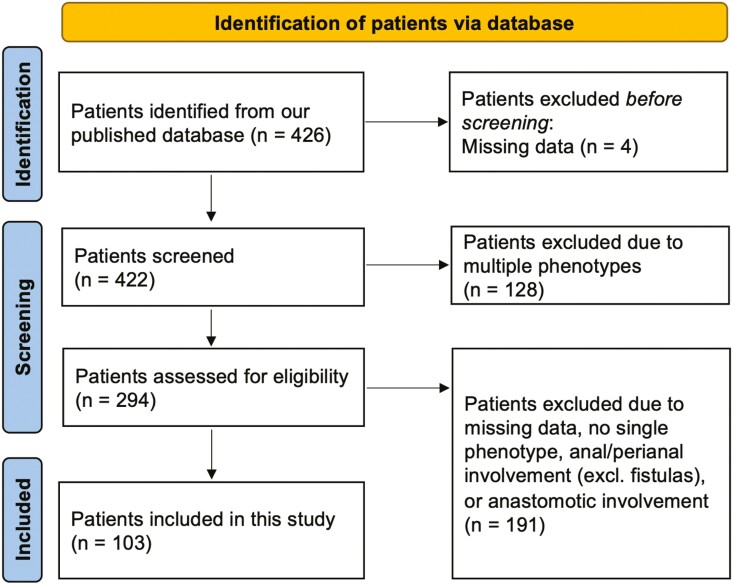
Methods: We retrospectively reviewed pouchoscopies and classified them into 7 main phenotypes: normal (n = 25), afferent limb (AL) involvement (n = 4), inlet involvement (n = 14), diffuse (n = 7), focal inflammation of the pouch body (n = 25), cuffitis (n = 18), and pouch-related fistulas (n = 10) with a single phenotype were included. Complete-case analysis was conducted.
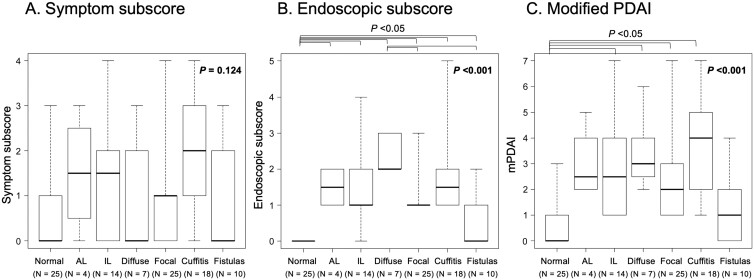
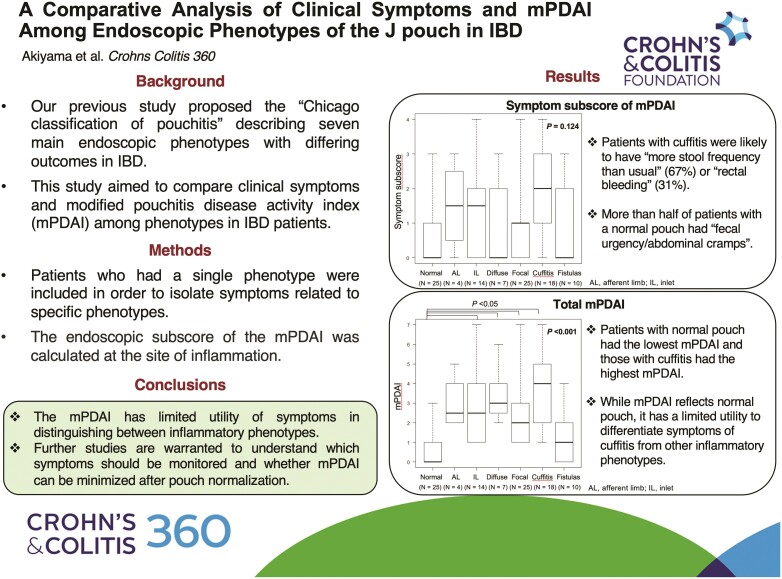
Results: One hundred and three IBD patients were included. The median mPDAI was 0 (IQR 0-1.0) in patients with a normal pouch. Among inflammatory phenotypes, the highest median mPDAI was 4.0 (IQR 2.25-4.75) in cuffitis, followed by 3.0 (IQR 2.5-4.0) in diffuse inflammation, 2.5 (IQR 1.25-4.0) in inlet involvement, 2.5 (IQR 2.0-3.5) in AL involvement, 2.0 (IQR 1.0-3.0) in focal inflammation, and 1.0 (IQR 0.25-2.0) in the fistula phenotype. Perianal symptoms were frequently observed in pouch-related fistulas (8/10, 80%) and cuffitis (13/15, 87%). Among patients with cuffitis, all had incomplete emptying (6/6, 100%).
Conclusions: We correlated the mPDAI with the endoscopic phenotypes and described the limited utility of symptoms in distinguishing between inflammatory phenotypes. Further studies are warranted to understand which symptoms should be monitored for each phenotype and whether mPDAI can be minimized after pouch normalization.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
