Timothy J Kleinig, Lisa Murphy, For the 30/60/90 National Stroke Targets Taskforce
{"title":"30/60/90 National stroke targets and stroke unit access for all Australians: it's about time","authors":"Timothy J Kleinig, Lisa Murphy, For the 30/60/90 National Stroke Targets Taskforce","doi":"10.5694/mja2.52459","DOIUrl":null,"url":null,"abstract":"<p>Stroke is the world's second-leading cause of death and the third-leading cause of death and disability.<span><sup>1</sup></span> In Australia, stroke is the third most common cause of death and a leading cause of disability.<span><sup>2</sup></span> As a result, stroke is costly to the health system, society and the individual.<span><sup>3</sup></span></p><p>Three acute stroke interventions have broadly applicable, significant, readily quantifiable health economic benefits: stroke unit care (for both ischaemic stroke and intracerebral haemorrhage)<span><sup>4</sup></span> and ischaemic stroke reperfusion therapies, thrombolysis<span><sup>5</sup></span> and endovascular thrombectomy (EVT).<span><sup>6</sup></span> For every 17 patients treated in a stroke unit, one death or disabled outcome is prevented.<span><sup>4</sup></span> The number needed to treat to prevent disability for thrombolysis under three hours is ten,<span><sup>5</sup></span> and the EVT number needed to treat to prevent functional dependency is five.<span><sup>6</sup></span> Expediting reperfusion therapies substantially magnifies treatment benefits; “saving a minute” gains an extra day of quality-adjusted life following thrombolytic treatment,<span><sup>7</sup></span> and an extra week following EVT.<span><sup>7, 8</sup></span></p><p>Despite Australia having a national acute stroke clinical care standard,<span><sup>9</sup></span> a national stroke registry (www.auscr.com.au), several centres of excellence<span><sup>10</sup></span> and population-based reperfusion therapy rates comparable to other high income countries,<span><sup>11, 12</sup></span> Australia compares poorly internationally in stroke unit admission percentages and speed of reperfusion treatment.<span><sup>11</sup></span> In 2022, Australia's median door-to-needle (thrombolytic) time was 75 minutes.<span><sup>11</sup></span> Only 27% of patients were treated within an hour of hospital arrival, compared with 82% in Sweden,<span><sup>12</sup></span> 75% in the United States (US),<span><sup>13</sup></span> and 61% in the United Kingdom (UK).<span><sup>14</sup></span> In Sweden during 2022, 93% of patients with stroke were admitted to a stroke unit, compared with 75% in Australia. The US, from 2016 to 2019, reported median door-arterial puncture times for non-transferred EVT cases of 78 minutes<span><sup>15</sup></span> versus 115 minutes in 2022 in Australia.<span><sup>11</sup></span></p><p>Concerningly, door-to-needle times and stroke unit admission percentages have not improved over the past six years (Box 1). Regional and remote Australians are most significantly affected by these treatment gaps.<span><sup>11, 16</sup></span> Because a higher proportion of Aboriginal and Torres Strait Islander Australians live in non-metropolitan areas, improving national stroke performance is a critical Closing the Gap initiative. Given the poorer stroke outcomes associated with suboptimal stroke care, continued national inertia is unjustifiable.</p><p>In 2023, national stroke leaders proposed that the “Championing Care”-themed combined Smart Strokes/Australian and New Zealand Stroke Organisation annual conference should urgently tackle these shortcomings.</p><p>Five clear standout areas for improvement were identified. Impactful targets reasonably achievable by 2030 were agreed, subsequently termed the “30/60/90 National Stroke Targets” (Box 2), incorporating certified stroke unit admission rates, rapid thrombolytic administration, rapid EVT, and rapid door-in-door-out times for EVT-eligible patients being transferred via road ambulance (Box 3). These targets were presented to a broad representative group at a pre-conference workshop and unanimously endorsed by workshop attendees. The targets have since been ratified by every major Australian stroke-interested organisation (Supporting Information).</p><p>During and following this workshop, we identified barriers to previous quality improvement efforts and facilitators for target progress (Box 4); many of which are counterparts. Key barriers included a previous lack of clearly articulated and prioritised targets and timeframes, lack of a national public-facing competitive stroke data dashboard (as in the UK),<span><sup>14</sup></span> our federated health system (with a complex mix of state and federal funding) and incomplete participation of hospitals nationally in transparent quality improvement initiatives. Facilitators include cohesive national stroke organisations, improving national telestroke coverage (both for acute and post-acute care),<span><sup>17</sup></span> a national stroke registry with recent development of national data dashboards, the recent national stroke unit certification initiative,<span><sup>18</sup></span> recent refinement of the National Stroke System Framework<span><sup>19</sup></span> and innovative pre-hospital stroke technologies coordinated through the Australian Stroke Alliance.<span><sup>20</sup></span></p><p>We do not need to reinvent the key granular acute “code stroke” time-saving strategies<span><sup>13, 21</sup></span> — many other countries have managed to improve their stroke care systems — we simply need to modify these proven strategies for the Australian context.</p><p>Most importantly, clinicians, health administrators and politicians need to commit to the key goals of stroke unit care for all, and expedited reperfusion treatment for eligible individuals. Three key initiatives need to then follow.</p><p>The Australian Stroke Coalition will provide national support and will seek government or philanthropic support to adapt and optimise a “Get with the guidelines”, or similar, program.<span><sup>25</sup></span> Approaches for funding will be grounded by a health economic analysis of benefits, should targets be met. State and national progress will be assessed at annual or biannual workshops, with lessons and strategies compared and shared. Performance will be incentivised by national achievement and improvement awards, and a national 30/60/90 stroke data dashboard through the national registry, where hospitals and states can compare their performance against their peers and the targets. It is hoped that national agreement on making the data dashboard consumer-facing will be reached, to allow citizens with lived experience to also advocate for improvements.</p><p>Reaching these targets is not an end, but a beginning. It is envisaged that the current targets will be Phase 1 of a sequence of national stroke targets. Achieving these targets will not only lead to improved stroke outcomes, but the streamlining and optimisation of acute stroke treatment pathways will greatly benefit Australian stroke professional training and research, across the continuum of stroke care. The mutual focus on a well articulated meaningful goal will increase team cohesion within hospitals, between professions, between states and between professional organisations.</p><p>Additionally, the optimised pre-hospital pathways for acute stroke treatment will benefit the development of ultra-early intracerebral haemorrhage pathways,<span><sup>26</sup></span> and potentially pave the way for ultra-early minimally invasive intracerebral haemorrhage surgery.<span><sup>27</sup></span> Consumer-facing national performance dashboards (if approved) may be adopted by other data-driven specialties, such as cardiology (for acute coronary syndromes), trauma services and intensive care units. This target-based, public-facing, data-driven approach, if broadly emulated, may serve as a key facilitator of nation-wide “learning health systems”.<span><sup>28</sup></span></p><p>A concerted effort is required to improve substandard Australian stroke unit admission rates and reperfusion treatment speed. A national commitment to addressing these treatment gaps is required, at all levels of health systems and government, supported by ambulance and retrieval services, emergency and radiology departments, and the medical and nursing staff administering acute stroke treatments. Addressing these shortcomings will provide a platform for further stroke improvements, and, if successful, could serve as a template for quality improvement initiatives in other health areas.</p><p>Open access publishing facilitated by The University of Adelaide, as part of the Wiley - The University of Adelaide agreement via the Council of Australian University Librarians.</p><p>No relevant disclosures for named authors. The Angels Initiative (a non-promotional healthcare project of Boehringer Ingelheim International to improve stroke care around the world) provided support for the 2023 National Stroke Targets 30/60/90 workshop and logistical support surrounding this. The Angels Initiative is a member of the Australian Stroke Coalition taskforce. The Angels Initiative did not propose any target or amendment to any target, and had no input into this manuscript.</p><p>Not commissioned; externally peer reviewed.</p>","PeriodicalId":18214,"journal":{"name":"Medical Journal of Australia","volume":"221 8","pages":"402-406"},"PeriodicalIF":6.8000,"publicationDate":"2024-09-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.5694/mja2.52459","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medical Journal of Australia","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.5694/mja2.52459","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Stroke is the world's second-leading cause of death and the third-leading cause of death and disability.1 In Australia, stroke is the third most common cause of death and a leading cause of disability.2 As a result, stroke is costly to the health system, society and the individual.3
Three acute stroke interventions have broadly applicable, significant, readily quantifiable health economic benefits: stroke unit care (for both ischaemic stroke and intracerebral haemorrhage)4 and ischaemic stroke reperfusion therapies, thrombolysis5 and endovascular thrombectomy (EVT).6 For every 17 patients treated in a stroke unit, one death or disabled outcome is prevented.4 The number needed to treat to prevent disability for thrombolysis under three hours is ten,5 and the EVT number needed to treat to prevent functional dependency is five.6 Expediting reperfusion therapies substantially magnifies treatment benefits; “saving a minute” gains an extra day of quality-adjusted life following thrombolytic treatment,7 and an extra week following EVT.7, 8
Despite Australia having a national acute stroke clinical care standard,9 a national stroke registry (www.auscr.com.au), several centres of excellence10 and population-based reperfusion therapy rates comparable to other high income countries,11, 12 Australia compares poorly internationally in stroke unit admission percentages and speed of reperfusion treatment.11 In 2022, Australia's median door-to-needle (thrombolytic) time was 75 minutes.11 Only 27% of patients were treated within an hour of hospital arrival, compared with 82% in Sweden,12 75% in the United States (US),13 and 61% in the United Kingdom (UK).14 In Sweden during 2022, 93% of patients with stroke were admitted to a stroke unit, compared with 75% in Australia. The US, from 2016 to 2019, reported median door-arterial puncture times for non-transferred EVT cases of 78 minutes15 versus 115 minutes in 2022 in Australia.11
Concerningly, door-to-needle times and stroke unit admission percentages have not improved over the past six years (Box 1). Regional and remote Australians are most significantly affected by these treatment gaps.11, 16 Because a higher proportion of Aboriginal and Torres Strait Islander Australians live in non-metropolitan areas, improving national stroke performance is a critical Closing the Gap initiative. Given the poorer stroke outcomes associated with suboptimal stroke care, continued national inertia is unjustifiable.
In 2023, national stroke leaders proposed that the “Championing Care”-themed combined Smart Strokes/Australian and New Zealand Stroke Organisation annual conference should urgently tackle these shortcomings.
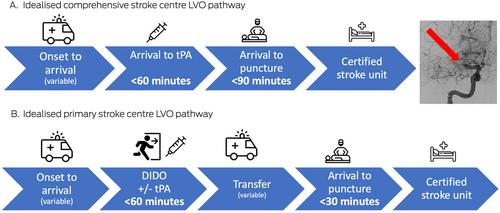
Five clear standout areas for improvement were identified. Impactful targets reasonably achievable by 2030 were agreed, subsequently termed the “30/60/90 National Stroke Targets” (Box 2), incorporating certified stroke unit admission rates, rapid thrombolytic administration, rapid EVT, and rapid door-in-door-out times for EVT-eligible patients being transferred via road ambulance (Box 3). These targets were presented to a broad representative group at a pre-conference workshop and unanimously endorsed by workshop attendees. The targets have since been ratified by every major Australian stroke-interested organisation (Supporting Information).
During and following this workshop, we identified barriers to previous quality improvement efforts and facilitators for target progress (Box 4); many of which are counterparts. Key barriers included a previous lack of clearly articulated and prioritised targets and timeframes, lack of a national public-facing competitive stroke data dashboard (as in the UK),14 our federated health system (with a complex mix of state and federal funding) and incomplete participation of hospitals nationally in transparent quality improvement initiatives. Facilitators include cohesive national stroke organisations, improving national telestroke coverage (both for acute and post-acute care),17 a national stroke registry with recent development of national data dashboards, the recent national stroke unit certification initiative,18 recent refinement of the National Stroke System Framework19 and innovative pre-hospital stroke technologies coordinated through the Australian Stroke Alliance.20
We do not need to reinvent the key granular acute “code stroke” time-saving strategies13, 21 — many other countries have managed to improve their stroke care systems — we simply need to modify these proven strategies for the Australian context.
Most importantly, clinicians, health administrators and politicians need to commit to the key goals of stroke unit care for all, and expedited reperfusion treatment for eligible individuals. Three key initiatives need to then follow.
The Australian Stroke Coalition will provide national support and will seek government or philanthropic support to adapt and optimise a “Get with the guidelines”, or similar, program.25 Approaches for funding will be grounded by a health economic analysis of benefits, should targets be met. State and national progress will be assessed at annual or biannual workshops, with lessons and strategies compared and shared. Performance will be incentivised by national achievement and improvement awards, and a national 30/60/90 stroke data dashboard through the national registry, where hospitals and states can compare their performance against their peers and the targets. It is hoped that national agreement on making the data dashboard consumer-facing will be reached, to allow citizens with lived experience to also advocate for improvements.
Reaching these targets is not an end, but a beginning. It is envisaged that the current targets will be Phase 1 of a sequence of national stroke targets. Achieving these targets will not only lead to improved stroke outcomes, but the streamlining and optimisation of acute stroke treatment pathways will greatly benefit Australian stroke professional training and research, across the continuum of stroke care. The mutual focus on a well articulated meaningful goal will increase team cohesion within hospitals, between professions, between states and between professional organisations.
Additionally, the optimised pre-hospital pathways for acute stroke treatment will benefit the development of ultra-early intracerebral haemorrhage pathways,26 and potentially pave the way for ultra-early minimally invasive intracerebral haemorrhage surgery.27 Consumer-facing national performance dashboards (if approved) may be adopted by other data-driven specialties, such as cardiology (for acute coronary syndromes), trauma services and intensive care units. This target-based, public-facing, data-driven approach, if broadly emulated, may serve as a key facilitator of nation-wide “learning health systems”.28
A concerted effort is required to improve substandard Australian stroke unit admission rates and reperfusion treatment speed. A national commitment to addressing these treatment gaps is required, at all levels of health systems and government, supported by ambulance and retrieval services, emergency and radiology departments, and the medical and nursing staff administering acute stroke treatments. Addressing these shortcomings will provide a platform for further stroke improvements, and, if successful, could serve as a template for quality improvement initiatives in other health areas.
Open access publishing facilitated by The University of Adelaide, as part of the Wiley - The University of Adelaide agreement via the Council of Australian University Librarians.
No relevant disclosures for named authors. The Angels Initiative (a non-promotional healthcare project of Boehringer Ingelheim International to improve stroke care around the world) provided support for the 2023 National Stroke Targets 30/60/90 workshop and logistical support surrounding this. The Angels Initiative is a member of the Australian Stroke Coalition taskforce. The Angels Initiative did not propose any target or amendment to any target, and had no input into this manuscript.
期刊介绍:
The Medical Journal of Australia (MJA) stands as Australia's foremost general medical journal, leading the dissemination of high-quality research and commentary to shape health policy and influence medical practices within the country. Under the leadership of Professor Virginia Barbour, the expert editorial team at MJA is dedicated to providing authors with a constructive and collaborative peer-review and publication process. Established in 1914, the MJA has evolved into a modern journal that upholds its founding values, maintaining a commitment to supporting the medical profession by delivering high-quality and pertinent information essential to medical practice.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
