Jue Wang, Xuan Zheng, Yajin Zhu, Guoning Zhu, Mingxi Lu
{"title":"[Application of prophylactic flow restriction in brachiocephalic arteriovenous fistulas].","authors":"Jue Wang, Xuan Zheng, Yajin Zhu, Guoning Zhu, Mingxi Lu","doi":"10.3724/zdxbyxb-2024-0092","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To investigate the effects of prophylactic flow restriction for brachiocephalic arteriovenous fistula on postoperative high-flow-related complications and patency rate in patients undergoing hemodialysis.</p><p><strong>Methods: </strong>Clinical data of patients with end-stage renal disease who underwent brachiocephalic arteriovenous fistula surgery for hemodialysis from February 2017 to May 2022 in Department of Nephrology, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine were retrospectively analyzed. During surgery, a 4-5 mm vascular suture loop was placed around the vein near the anastomosis as a flow restriction device in 43 patients (flow restriction group), while 42 patients did not receive the prophylactic flow restriction ring (control group). All patients were followed up for 1 to 5 years. The incidence rates of complications related to the hemodialysis access pathway, including distal ischemia syndrome, the formation of arteriovenous fistula aneurysms, thrombus, high-flow congestive heart failure, anastomosis of the vein within 1 cm of the anastomosis and cephalic arch stenosis, were compared between the two groups. The natural blood flow rate of the arteriovenous fistula, anastomosis size, the internal diameter of the vein near the anastomosis, primary patency rate, assisted primary patency rate, and secondary patency rate of the arteriovenous fistula, were also evaluated and compared between the two groups. Logistic regression analysis was used to investigate the factors affecting arteriovenous fistula patency rates, as well as the impact of the flow-restricting ring on postoperative factors.</p><p><strong>Results: </strong>Ultrasound measurements showed that the internal diameter of the vein at the site of the flow restriction ring in the flow restriction group was (3.7±0.6) mm at three months postoperatively, which was significantly smaller than the internal diameter of the narrowest part of the vein near the anastomosis in the control group [(4.1±1.0) mm, <i>t</i>=-2.416, <i>P</i><0.01]. The postoperative anastomotic diameter and natural blood flow rate of the arteriovenous fistula in the flow restriction group were both significantly lower than those in the control group (both <i>P</i><0.05). Furthermore, the incidence rates of various complications in the flow restriction group were significantly lower than those in the control group (all <i>P</i><0.05). At 6, 12, and 24 months postoperatively, the primary patency rate and assisted primary patency rate in the flow restriction group were significantly higher than those in the control group (both <i>P</i><0.05), while there was no significant difference in secondary patency rates between the two groups (<i>P</i>>0.05). Binary logistic regression analysis indicated that age, diabetes, and natural blood flow rate of the arteriovenous fistula at 3 months postoperatively were independent risk factors for primary patency rate, while the flow restriction for brachiocephalic arteriovenous fistula was an independent protective factor for primary patency rate (<i>P</i><0.01 or <i>P</i><0.05). The application of flow restriction was negatively correlated with anastomotic diameter at 6 and 12 months, natural arteriovenous fistula blood flow, and the incidence rates of cephalic arch stenosis and aneurysm formation (all <i>P</i><0.05).</p><p><strong>Conclusions: </strong>The prophylactic constriction during brachiocephalic arteriovenous fistula surgery in patients undergoing hemodialysis can limit the size of the anastomosis and postoperative arteriovenous fistula blood flow, reducing complications such as cephalic arch stenosis and high-flow heart failure, and increasing primary patency rates of arteriovenous fistula and delay the reintervention of the fistula.</p>","PeriodicalId":24007,"journal":{"name":"Zhejiang da xue xue bao. Yi xue ban = Journal of Zhejiang University. Medical sciences","volume":" ","pages":"623-631"},"PeriodicalIF":0.0000,"publicationDate":"2024-10-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11528141/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Zhejiang da xue xue bao. Yi xue ban = Journal of Zhejiang University. Medical sciences","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3724/zdxbyxb-2024-0092","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: To investigate the effects of prophylactic flow restriction for brachiocephalic arteriovenous fistula on postoperative high-flow-related complications and patency rate in patients undergoing hemodialysis.
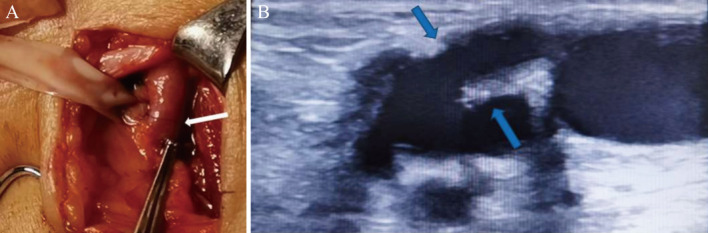
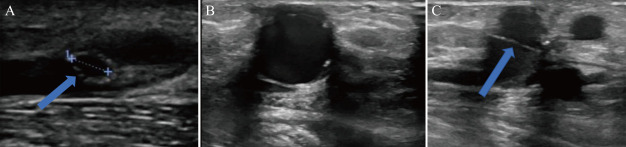
Methods: Clinical data of patients with end-stage renal disease who underwent brachiocephalic arteriovenous fistula surgery for hemodialysis from February 2017 to May 2022 in Department of Nephrology, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine were retrospectively analyzed. During surgery, a 4-5 mm vascular suture loop was placed around the vein near the anastomosis as a flow restriction device in 43 patients (flow restriction group), while 42 patients did not receive the prophylactic flow restriction ring (control group). All patients were followed up for 1 to 5 years. The incidence rates of complications related to the hemodialysis access pathway, including distal ischemia syndrome, the formation of arteriovenous fistula aneurysms, thrombus, high-flow congestive heart failure, anastomosis of the vein within 1 cm of the anastomosis and cephalic arch stenosis, were compared between the two groups. The natural blood flow rate of the arteriovenous fistula, anastomosis size, the internal diameter of the vein near the anastomosis, primary patency rate, assisted primary patency rate, and secondary patency rate of the arteriovenous fistula, were also evaluated and compared between the two groups. Logistic regression analysis was used to investigate the factors affecting arteriovenous fistula patency rates, as well as the impact of the flow-restricting ring on postoperative factors.
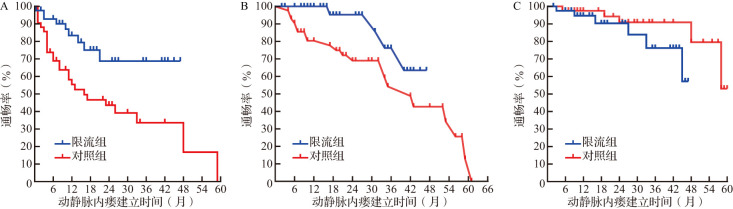
Results: Ultrasound measurements showed that the internal diameter of the vein at the site of the flow restriction ring in the flow restriction group was (3.7±0.6) mm at three months postoperatively, which was significantly smaller than the internal diameter of the narrowest part of the vein near the anastomosis in the control group [(4.1±1.0) mm, t=-2.416, P<0.01]. The postoperative anastomotic diameter and natural blood flow rate of the arteriovenous fistula in the flow restriction group were both significantly lower than those in the control group (both P<0.05). Furthermore, the incidence rates of various complications in the flow restriction group were significantly lower than those in the control group (all P<0.05). At 6, 12, and 24 months postoperatively, the primary patency rate and assisted primary patency rate in the flow restriction group were significantly higher than those in the control group (both P<0.05), while there was no significant difference in secondary patency rates between the two groups (P>0.05). Binary logistic regression analysis indicated that age, diabetes, and natural blood flow rate of the arteriovenous fistula at 3 months postoperatively were independent risk factors for primary patency rate, while the flow restriction for brachiocephalic arteriovenous fistula was an independent protective factor for primary patency rate (P<0.01 or P<0.05). The application of flow restriction was negatively correlated with anastomotic diameter at 6 and 12 months, natural arteriovenous fistula blood flow, and the incidence rates of cephalic arch stenosis and aneurysm formation (all P<0.05).
Conclusions: The prophylactic constriction during brachiocephalic arteriovenous fistula surgery in patients undergoing hemodialysis can limit the size of the anastomosis and postoperative arteriovenous fistula blood flow, reducing complications such as cephalic arch stenosis and high-flow heart failure, and increasing primary patency rates of arteriovenous fistula and delay the reintervention of the fistula.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
